What is lymphoma?
Lymphoma is a lesion of the immune system and internal organs, in which altered cells accumulate, disrupting tissue function.
The tumor develops in the lymphatic system, which helps us fight infections and other diseases. The lymph circulating in it washes all the cells of the body and delivers the necessary substances to them, taking away waste. In the lymph nodes located throughout its network, dangerous substances are neutralized and removed from the body. The lymphatic system complements the circulatory system and helps fluids move throughout the body. Unlike blood, the speed of which is set by the “pump” - the heart, lymph slowly circulates on its own.
How does lymphoma develop?
Oncology begins with the appearance in the body of just one altered cell of the immune system. In total, there are 2 main types:
- B lymphocytes
: produce antibodies - proteins that protect the body from bacteria and viruses. This is where most lymphomas form. - T lymphocytes
, one part of which destroys germs and abnormal cells, and the second helps to increase or slow down the activity of the immune system.
Almost all abnormal cells are identified and destroyed by our immune system, but some of them manage to survive. They gradually multiply, spread throughout the body, create tumors, accumulate in internal organs and disrupt their functioning.
The disease can occur in any area where lymphatic tissue is located, the main areas of which are:
- Lymph nodes
are small, pea-sized organs that are collections of cells of the immune system, including lymphocytes. There are more than 500 of them in the human body. - The spleen
, located under the lower ribs on the left side of the body. It produces lymphocytes, stores healthy blood cells and filters out damaged ones, and destroys microbes and foreign substances. - Bone marrow is
the spongy tissue inside certain bones. Here new blood cells are formed, including some lymphocytes. - The thymus, or thymus gland, is
a small organ located behind the upper part of the sternum in front of the heart. It is where some lymphocytes mature and develop. - Tonsils, or tonsils, are
collections of lymphatic tissue in the back of the throat. These organs help produce antibodies, proteins that prevent inhaled or ingested microorganisms from multiplying. - Digestive Tract:
The stomach, intestines and many other organs also contain lymphatic tissue.
BULLETIN OF THE MOSCOW ONCOLOGICAL SOCIETY
Informo, ergo sum!
Moscow Oncological Society
THE DIVERSITY OF VARIANTS OF LYMPHOMA CAUSES A JUSTIFIED INTEREST IN ALL MORPHIC-IMMUNOLOGICAL MANIFESTATIONS OF THIS PATHOLOGY...
THE INFORMATION BULLETIN OF THE MOSCOW ONCOLOGICAL SOCIETY HAS BEEN PUBLISHED SINCE 1994.
| №10 (561) 2009 OCTOBER |
MEETING 561
DEDICATED TO THE MEMORY OF ACADEMICIAN N.A.
KRAEVSKY, JOINT WITH THE RUSSIAN SOCIETY OF PATHOLOGISTS will take place on Tuesday, October 13, 2009
at
17:00
in the conference hall of the clinic of the Russian Oncological Research Center named after. N.N. Blokhina
Presidium: prof. A.I. Paches, academician of the Russian Academy of Medical Sciences, prof. Yu.N. Soloviev, corresponding member of the Russian Academy of Medical Sciences, prof. I.V. Poddubnaya, prof. A.I. Karseladze
Agenda:
CLINIC AND MORPHOLOGY OF MALT-LYMPHOMA
Report:
MORPHOLOGICAL DIAGNOSTICS OF GASTRIC MALT LYMPHOMA
Kokosadze N.V., Probatova N.A., Kovrigina A.M., Zakharova E.S., Karseladze A.I. (Russian Oncology Research Center named after N.N. Blokhin)
Report:
CLINICAL ASPECTS OF MALT LYMPHOMA
Poddubnaya I.V.¹, Osmanov E.A.², Moskalenko O.A.¹, Malikhova O.A.², Sotnikova O.P.¹, Suanova Z.A.¹, Subortseva I.N.¹ (¹ Russian Medical Academy of Postgraduate Education; ² Russian Oncology Research Center named after N.N. Blokhin)
BUDGET SURPLUS OF THE MOSCOW ONCOLOGICAL SOCIETY
The Moscow Oncological Society has successfully launched a campaign to collect membership fees for the 2009/2010 production year. The basis of the life of our professional community in 2007-2008. provided 398,300 rubles, collected in the amount of 207,700 and 190,600 rubles. in 2007/08 and 2008/09 respectively. Meanwhile, the annual expenses of the Society for preparing and holding meetings, publishing and distributing printed materials back in 2007 reached 200,100 rubles. and over the past two years have been characterized by a steady upward trend. A significant item of expenditure was the cost of publishing collections of minutes of the Society's meetings. A collection of materials from 2007, entitled “JUBILEES at the Russian Cancer Research Center: 55 years of the Oncology Center and 95 years of the founder of the Russian Cancer Research Center - Academician N.N. Blokhin”, came out of print and is distributed among full members of the Society. Collections 2008-2009 are being prepared for publication.
Despite the fact that the Society's expenses exceed the funds received as contributions, the budget of the professional society remains in surplus. This is provided by income received from the publication of advertising materials in the Society's publications. However, collection of membership dues remains our most important organizational campaign.
Membership fees to the Moscow Oncological Society are 100 rubles for residents and graduate students, 300 for certified oncologists and 500 for oncologist managers. In the clinical departments of the Research Institute of Clinical Oncology, Russian Cancer Research Center. N.N. Blokhin, contributions are differentiated from 100 rubles for residents to 1000 rubles for professors and heads of departments (at the same time, doctors and researchers contribute 300 rubles, senior and leading researchers who do not yet have a doctorate pay 500, and those who have already become doctors of science - 700 rubles). Of course, the Society is interested in accepting new specialists and receiving their individual contributions. However, receiving contributions in bulk makes solving organizational problems much easier. The organizing committee asks the heads of departments to instruct the most authoritative professionals to collect contributions from their teams. Obviously, this can confirm the outstanding organizational skills of the specialists involved in such gatherings.
In conclusion, the Organizing Committee recalls a number of provisions that make up the special, unique aura of the contribution collection campaign: the membership fee can be paid by transferring to the Society part of the circulation of one’s own books, scientific videos and other scientific products. Specialists who are members of other professional communities (anesthesiologists, resuscitators, radiologists, etc.) have an unconditional right to discounts.
Veterans of the society who joined it in the 1950s and 60s no longer pay dues.
PROCEEDINGS OF THE MOSCOW ONCOLOGICAL SOCIETY
Message abstracts:
PROCEEDINGS OF THE MOSCOW CANCER SOCIETY No. 561
(October 13, 2009) The Proceedings is held jointly with the society of Pathologists to honor the memory of Prof.
NAKRAEVSKY (1905-1985) CLINICAL FEATURES AND PATHOLOGY OF MALT-LYMPHOMAS
Report: PATHOLOGY OF MALT-LYMPHOMAS. By Dr. N. Kokosadze, Prof. N. Probatova, Dr. E.Zakharova, Prof. A. Karseladze (The NNBlokhin Cancer Research Center).
Report: CLINICAL FEATURES AND CURABILITY IN PATIENTS WITH MALT-LYMPHOMAS. By Prof. I. Poddubnaya, Prof. E. Osmanov, Dr. O. Moskalenko et al. (Russian Medical Academy of Postgraduate Education).
Report:
MORPHOLOGICAL DIAGNOSTICS OF GASTRIC MALT LYMPHOMA
Kokosadze N.V., Probatova N.A., Kovrigina A.M., Zakharova E.S., Karseladze A.I. (Russian Oncology Research Center named after N.N. Blokhin)
" MALT lymphoma " was first described by Isaacson PD (1980). Despite extensive experience in studying this nosological form, its diagnosis and treatment remain imperfect. The reason for this situation is the widespread opinion about the relatively favorable prognosis of the tumor, which gives rise to dynamic observation without an adequate assessment of the severity of the condition and the stage of the disease. On the contrary, chronic inflammatory processes associated with MALT lymphomas, in particular autoimmune ones, lead to the prescription of unnecessary, expensive diagnostic procedures and therapeutic measures. Obviously, the state of diagnosis and treatment of MALT lymphomas is also a consequence of insufficient coverage of these problems in the methodological scientific literature.
Clinical and morphological data
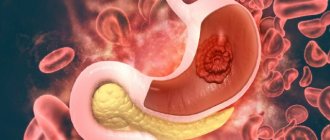
MALT lymphoma accounts for about 7-8% of all B-cell lymphomas and more than 50% of primary gastric lymphomas. Most cases occur in adults (median age 61 years), with a male to female ratio of 1.0:1.2. Most cases of MALT lymphoma are associated with prolonged inflammation, which results in the accumulation of extranodal lymphoid tissue. Chronic inflammation can be caused by infection, autoimmune or another unknown cause. Infectious agents that cause the accumulation of extranodal lymphoid tissue that precedes MALT lymphoma are Helicobacter pylori for MALT lymphoma of the stomach (Fig. 1), Chlamydia psittaci for MALT lymphoma of the orbit, Borrelia burgdoferi for MALT lymphoma of the skin, Campylobacter jejuni for a special subtype of MALT lymphoma, formerly known as “α-heavy chain disease” and now as “immunoproliferative small intestinal disease (IPSID).” Autoimmune chronic inflammation in Hashimoto's thyroiditis and Sjögren's syndrome is known to greatly increase the risk of MALT lymphoma of the thyroid and salivary glands. The gastrointestinal tract is most often affected (more than 50% of all cases) by MALT lymphoma, with 85% of gastrointestinal lymphomas localized in the stomach. Next in frequency of MALT lymphoma are: bone marrow (up to 20% of cases), head and neck organs (primarily salivary glands, orbit) and lungs (14 each), skin (11%), thyroid and mammary glands ( 4%).
MALT lymphoma is characterized by a long clinical (indolent) course, and therefore most cases are detected in stages I-II. In primary MALT lymphomas of the stomach, lesions in extranodal locations are diagnosed in up to 25% of cases, while in primary MALT lymphomas of other organs, the frequency of lesions in extranodal locations increases to 46%. Incorrect staging of MALT lymphomas is similar to determining the stages of lymphomas affecting the lymph nodes, since with multiple extranodal tumor foci, systemic lesions (gastrointestinal tract, skin, etc.), staging does not reflect the true prevalence of the process.
Histological picture of MALT lymphoma
Using biopsy and surgical material from 115 patients with primary gastric lymphomas observed at the Russian Cancer Research Center since 1995, morphological criteria for the diagnosis of MALT lymphoma, its differential diagnostic features in comparison with reactive (non-tumor) lymphoid cell infiltrates and other peripheral small B-cell lymphomas were developed.
The morphological picture of MALT lymphoma is polymorphic due to the heterogeneous composition of the tumor infiltrate, in which marginal zone cells, small lymphocytes, scattered immuno- and centroblasts, and monocytoid-type cells are detected in various combinations (Fig. 2-3).
Morphological characteristics were assessed according to the following indicators: cellular composition, atypia of neoplastic elements, the presence of plasma cell differentiation of lymphoid cells, the severity of plasmacytic infiltration, the presence and severity of lymphoepithelial lesions, reactive lymphoid follicles with colonization phenomena, the presence of large (blast) cells.
Lymphoepithelial lesions (LELs) - aggregates of 3 or more marginal zone cells that destroy the epithelium of the glands - are found in every second case. The destruction of the glands was expressed in the distortion of their outlines and the erasing of boundaries. In 17.1% of cases, large “blastic” LELs were detected (Fig. 4).
Rice. 1.
Helicobacter pylori in the mucus on the surface and in the lumen of the glands (heme-eos stain x1000).
Rice.
2. MALT lymphoma: “dense” lymphoid cell infiltrate in the lamina propria of the gastric mucosa among the glands (heme-eos stain x200).
Rice.
3. MALT lymphoma: lymphoid cell infiltrate from a mixture of small and medium-sized cells with round-oval, centrocyte-like and irregularly shaped nuclei (heme-eos staining x400).
Rice.
4. Lymphoepithelial lesion: infiltration of the gland epithelium with small lymphoid cells (heme-eos staining x1000).
In the gastrobiopsy material, follicles and follicle-like structures were identified in 30%, reactive follicles with light reproduction centers of centrocytes and centroblasts – in 14% of cases. In almost every second case, in the presence of lymphoid follicles, their colonization was observed. The neoplastic infiltrate usually contained large cellular forms, similar in morphology to centroblasts or immunoblasts - blast cells with nuclei either round-oval or slightly irregular in shape and 1-3 nucleoli; or - with round vesicular nuclei and a compact, centrally located nucleolus. Since MALT lymphoma by definition consists predominantly of small cells, if solid proliferations of large transformed cells are present in the tumor infiltrate, the tumor should be classified as diffuse large B-cell lymphoma and the presence of concomitant MALT lymphoma should be noted.
The term “high-grade MALT lymphoma” is not recommended. In addition, the term “MALT lymphoma” should not be used to refer to large B-cell lymphoma, even if it occurs in organs with MALT and is associated with lymphoepithelial lesions.
Differential diagnosis
To develop reliable differential diagnostic criteria, reactive lymphoid cell infiltrates were studied in histological preparations of gastrobiopsies of patients with chronic gastritis associated with HP infection. It should be noted that some polymorphism, atypia, follicles and lymphoepithelial lesions are also observed in reactive infiltrates, which can coexist with the most common crypt abscesses in this nosology.
Among the morphological signs of reactive lymphoid cell infiltrates, cells with centrocytoid nuclear morphology, without signs of cytological atypia, or with mild cytological atypia, predominated. Monocytoid B lymphocytes were not detected. Plasma cells were found in large numbers in the form of layers under the surface pitted epithelium. In no case was plasmacytoid differentiation of lymphoid cells in the infiltrates detected. Follicles were found in 34.7% of cases without signs of colonization. Single large (blast) cells were detected in 8.7% of cases and were scattered among the small cell infiltrate.
Gastric lymphomas selected for differential diagnosis with MALT lymphoma were peripheral small B-cell lymphomas. In this group, follicular lymphomas, lymphomas from mantle cells, and cases of Burkitt's lymphoma were analyzed, since this nosology may have medium-sized neoplastic cells. Follicular lymphoma was characterized by a nodular or diffuse-nodular growth pattern, with an infiltrate mixed in cellular composition. PL differed in cellular composition into several types. Lymphoma from the cells of the mantle zone was characterized by focal-diffuse or diffuse proliferation of infiltrate from monomorphic or small (medium) sized cells against the background of inflammatory changes. In Burkitt's lymphoma, the tumor infiltrate extended to the integumentary pit epithelium, displacing inflammatory cells, forming single LELs; at the same time, closely lying cells of predominantly medium size with scattered macrophages formed a picture reminiscent of a “starry sky” (similar to the picture observed with damage to the lymph nodes).
Immunohistochemical and genetic studies
The classification of lymphoid tumors is based on the processing of all available information to determine the nature of the disease. The morphological picture and immunophenotype are quite sufficient for the diagnosis of most lymphomas. However, no antigenic marker for lymphomas is specific. Only a combination of morphological features and a specific panel of antigenic markers can help establish the correct diagnosis. Most B-cell lymphomas have a characteristic combination of immunophenotypic features. No pathognomonic immunohistochemical signs for MALT lymphoma have been found to date. Differential diagnosis continues to include exclusion of other small B-cell lymphomas. It is advisable to evaluate the immunohistochemical picture according to the following parameters: violation of immunoarchitecture, aberrant immunophenotype, monoclonality. In an immunohistochemical study, a comparison of the expression of CD20 and CD3 antibodies is of differential diagnostic value: the predominance of CD20-positive B lymphocytes over CD3-positive T lymphocytes indicates a violation of the immunoarchitecture observed in lymphomas. In reactive (non-tumor) processes, T-lymphocytes in the lymphoid cell infiltrate predominate over B-lymphocytes or are in equal proportions. An important feature is the coexpression of BCL-2 and the T-cell marker CD43 by B cells. To identify an aberrant immunophenotype, it is necessary to compare the expression of BCL-2 and CD43 with the expression of other T and B cell markers.
Genetic features play an increasingly important role in the classification of lymphoid tumors. For most small B-cell lymphomas and leukemias, genetic lesions have been identified. However, the molecular pathogenesis of most T-cell and NK-cell lymphomas remains unclear. PCR study of IGH gene rearrangement and T-cell receptor (TCR) gene rearrangement, in situ
hybridization (FISH) are valuable diagnostic studies, both for determining clonality in B- and T-cell proliferations (in terms of differential diagnosis with reactive hyperplasia), and for identifying translocations associated with certain tumors. In the vast majority of cases, molecular testing for the presence of clonality of Ig heavy chain gene rearrangement can confirm or refute the diagnosis of MALT lymphoma. Some mature B-cell neoplasias have characteristic genetic abnormalities, which can be used to determine their biological properties and, therefore, the possibility of differential diagnosis (and treatment). Detection of chromosomal translocation t(11;18) in patients with MALT lymphoma by FISH reaction is necessary for prescribing rational treatment, since cases of MALT lymphoma with t(11;18) are resistant to anti-Helicobacter therapy.
Report:
CLINICAL ASPECTS OF MALT LYMPHOMA
Poddubnaya I.V.¹, Osmanov E.A.², Moskalenko O.A.¹, Malikhova O.A.², Sotnikova O.P.¹, Suanova Z.A.¹, Subortseva I.N.¹ (¹ Russian Medical Academy of Postgraduate Education; ¹Russian Oncology Research Center named after N.N. Blokhin)
In the literature of the 2000s. not only the steady increase in the incidence of non-Hodgkin lymphomas is emphasized, but also the increase in the identification of various forms and/or morphological variants of lymphoproliferation; First of all, extranodal lymphomas. The identified features have both scientific and practical significance. Of greatest interest is the increase in the incidence of MALT lymphomas, as lesions of various localization and prognosis.
During the period from 1983 to 2007, 704 patients with extranodal lymphomas were observed at the Russian Cancer Research Center. In this group, the most frequently diagnosed lesions were the stomach (33%), bones (13%), testicles (8%); other organs and tissues (46%).
The incidence of MALT lymphomas was highest when tumors were localized in the gastrointestinal tract; primarily in the stomach. The experience of the Russian Cancer Research Center is characterized by the diagnosis and treatment of 68 cases of primary gastric MALT lymphomas of stages I-II. When analyzing the clinical material, a predominance of women was noted (65%), and the variants of macroscopic growth forms were clarified. A peculiar, gastritis-like form of MALT lymphoma, characteristic of the small cell variant, has been identified. Endoscopic signs of treatment effectiveness were determined.
Other parts of the gastrointestinal tract are involved in the tumor process in lymphomas much less frequently - intestinal damage is only 4.7%. The morphological structure of these tumors also seems different - the frequency of MALT lymphomas is significantly lower than diffuse large B-cell lymphoma (DLBCL). We have experience in monitoring the course of the disease in 33 patients with primary intestinal non-Hodgkin lymphoma - MALToma and DLBCL.
Regardless of the morphoimmunological variant, this pathology often (84.9%) develops life-threatening complications of the clinical course of the disease: intestinal obstruction (92.8%), intestinal perforation (3.6%), bleeding (3.6%). This suggests that intestinal MALT-omas have clinical uniqueness and require a special therapeutic approach. Performing radical surgery in the presence of complications provides 78.3% of 5-year overall survival, but does not prevent the development of relapse - progression of the process was diagnosed in 20.8% of patients.
Rare forms of extranodal lymphomas include primary lung lesions. Among 704 patients, primary tumors were detected in only 13 (1.8%) patients. All neoplasms turned out to be of B-cell origin, among them MALT lymphomas predominated (54%), aggressive variants accounted for 32%. MALT-omas were diagnosed in the initial stages and were highly sensitive to immunochemotherapy: with R-CHOP, complete remissions were achieved in all patients. In aggressive variants of lymphomas with primary involvement of the lungs, none of the standard treatment regimens had a positive effect, which allows us to recommend intensification of the first line of therapy in these clinical situations.
It is known that the risk of developing lymphoproliferation increases in various autoimmune processes. In this regard, non-Hodgkin's lymphomas of the salivary glands are of particular interest. Of the 44 cases of salivary gland lymphoma observed, 8 patients (16%) had a history of Sjogren's disease. DLBCL is the most common morphoimmunological variant of salivary gland NHL that occurs de novo; MALT's share was 30%. This ratio changes fundamentally if lymphoma occurs against the background of Sjögren's disease: the main variant is MALT lymphoma, which is diagnosed in 78% of cases.
The sensitivity to immunochemotherapy with MALT of the salivary glands of any origin is equally high: the frequency of complete remissions corresponds to 84-100%.
The presented data demonstrate the justification for distinguishing MALT lymphomas, since these tumors constitute a heterogeneous group of neoplasms of B-cell origin with a wide variety of morphological and clinical characteristics.
Undoubtedly, the introduction of gastrosonography has become a new direction in improving the diagnosis and treatment of primary gastric MALT lymphomas. Clarifying the degree of invasion into the organ wall allows us to more adequately assess the prevalence of the process, clarify the diagnosis, and also more accurately monitor the effectiveness of the therapy. The use of the classification of the French group GELA, which carries out a multi-stage morphological assessment of the effectiveness of therapy, supported by PCR of gastroscopy material, is promising.
The materials of the Russian Cancer Research Center confirm the favorable prognosis of MALT lymphomas: the overall 5-year survival rate, depending on the morphological variants of these tumors, is 71.4; 85.9; 96.8%. Indications for anti-Helicobacter monotherapy were determined and its effectiveness was established depending on the prevalence of the process. In stage I, anti-Helicobacter therapy together with chemotherapy made it possible to achieve 87.5% of complete regressions.
New therapeutic approaches are being studied for relapsed and refractory forms of primary gastric MALT (chlorbutine in combination with rituximab, cladribine with rituximab).
Meetings of the Society are usually held on the last Thursday of every month (except July and August). Messages for discussion at meetings of the professional community of oncologists, as well as initiative proposals for new topics should be sent to the postal and email addresses specified in the output of the Society's Bulletin.
Is lymphoma cancer?
Official medicine in Russia and some other countries refers to cancer as malignant tumors - life-threatening neoplasms that develop in epithelial cells contained in the skin or mucous membranes and lining the internal surface of organs.
Lymphoma is not a cancer, but an oncological disease. It is formed from lymphocytes, and its cells are also able to divide uncontrollably, accumulate in tissues, disrupting their work, and create additional foci of disease in various parts of the body.
general information
The diagnosis of malt lymphoma of the stomach was introduced into practice relatively recently. Previously, this pathology was considered “pseudolymphoma,” until in 1983 scientists proved the origin of the entire tumor from one malignant cell. The term MALT stands for mucosal associated marginal zone lymphoma. They can appear in any extranodal (primary focus outside the lymph nodes) organs and structures of the body, most often affecting the digestive system (30-40%). The stomach accounts for 60-75%.
This pathology belongs to non-Hodgkin lymphoma. Women get sick somewhat more often than men. In most cases, the disease develops after 50-60 years. Usually the process occurs locally (one focus) in the antrum of the stomach (the body or cardia is less commonly affected). More often the disease is diagnosed in the initial stages (about 70%).
Types of lymphomas
Doctors distinguish 2 main classes of them:
- Hodgkin's lymphoma, or lymphogranulomatosis
: Most often starts in the lymph nodes of the upper body - in the chest, neck or armpits. It usually spreads to various lymph nodes through the lymphatic vessels, but in rare cases, in later stages it enters the bloodstream and spreads to other parts of the body, such as the liver, lungs or bone marrow. This diagnosis is made when special cells are identified in the body - Berezovsky-Reed-Sternberg, which are modified B-lymphocytes.
- TO non-Hodgkin's lymphomas
include all other types of the disease - there are about 30 of them. Each of them has its own special characteristics: the location of the primary tumor, the structure and speed of development.
Types of lymphomas by aggressiveness
Since there are many diseases that are included in this group, they are usually divided into groups according to different criteria. One of them is the aggressiveness of the current.
So-called flaccid lymphomas (also known as indolent lymphomas) develop slowly and do not threaten the patient’s life for several years. With timely treatment, the chances of a long and lasting remission are high. This group includes lymphocytic as well as follicular lymphoma.
Aggressive forms, which include diffuse (mixed and large cell) forms, can kill the body within months, and highly aggressive forms - even within weeks. The latter, for example, include T-cell leukemia and Burkitt's lymphoma. In the treatment of any disease and in maintaining the adequate condition of the patient, timely professional assistance plays an important role.
Causes of lymphoma development
Doctors and scientists do not know exactly why the disease begins to develop in the human body. They only know about the factors that increase the likelihood of developing each type of cancer.
For Hodgkin's lymphomas
they look like this:
- Epstein-Barr virus
, which causes infectious mononucleosis - damage to lymphoid tissue, including adenoids, liver, spleen and lymph nodes. In some patients, parts of the virus are found in Berezovsky-Reed-Sternberg cells, but in most patients there are no signs of it. - Age
: Diagnosis can be made at any age, but it is most common in 20-year-olds and people over 55. - Gender
: The disease is more common among men than among women. - Heredity and family history
: The risk is increased for siblings and for identical twins. Identical twins develop from a single egg fertilized by a single sperm. They come in only one gender, have the same genes and are extremely similar in appearance. owners of Hodgkin's lymphoma. The reason for this is not exactly known - perhaps the whole point is that members of the same family suffer the same infections in childhood, or have common inherited gene changes that increase the likelihood of developing this type of oncology. - Weakened immune system
. The chances of receiving this diagnosis increase in people with HIV infection and disorders of the immune system, which develop, among other things, due to the use of drugs that suppress it, which is often required after an organ transplant.
List of such factors for non-Hodgkin's lymphomas
looks different:
- These include exposure to radiation
, including doses received during radiation therapy used to treat other types of cancer. - Various substances
, including herbicides and insecticides that kill weeds and insects, as well as chemotherapy drugs. - Age
: as a rule, the older the person, the higher his risks - in most cases the disease occurs at the age of 60+, but some types also occur in younger people. - Malfunctions of the immune system
affect the chances of developing all types of lymphomas. - Some viruses
can influence the DNA of lymphocytes, which encrypts all the information about our body, and convert them into cancer cells. - Infections that constantly stimulate the immune system and force our natural defenses to work harder also increase the risk of receiving a serious diagnosis.
- Having close blood relatives - parents, children, brothers or sisters - with this diagnosis also increases the likelihood of developing the disease.
- Some studies have shown that breast implants, especially those with a rough surface, may cause anaplastic large cell lymphoma. It develops on the skin, lymph nodes, or scar tissue formed at the site of the incision.
Incidence of non-Hodgkin's lymphomas (NHL)
More than 90% of NHL is diagnosed in adult patients. Most often, NHL occurs between the ages of 60 and 70 years. The risk of developing this tumor increases with age.
The lifetime personal risk of developing NHL is approximately 1 in 50.
Since the beginning of the 70s, there has been an almost twofold increase in the incidence of NHL. This phenomenon is difficult to explain. This is mainly associated with infection caused by the human immunodeficiency virus. Part of this increase can be attributed to improved diagnostics.
Since the late 90s, there has been a stabilization in the incidence of NHL.
NHL is more often detected in men compared to women.
In 2002, 5,532 cases of NHL in adult patients were identified in Russia.
In the United States in 2004, according to preliminary data, 53,370 cases of NHL in adults and children are expected.
Symptoms and signs of lymphoma
As a rule, in the early stages this type of oncology does not manifest itself in any way, and its owner feels well and is not aware of the disease - almost all of its symptoms appear later, in advanced stages.
One of the most common signs is the appearance of swelling in the neck, armpits, groin, or above the collarbone.
, which is an enlarged lymph node. Typically, such a tumor does not hurt, but over time it often increases, and new lumps appear next to it or in other areas of the body.
Lymphomas that begin to develop or grow in the abdominal cavity can cause swelling
or
abdominal pain, nausea,
and
vomiting
. Such sensations occur due to enlargement of the lymph nodes or internal organs, such as the spleen or liver, or the accumulation of large amounts of fluid.
An enlarged spleen can put pressure on the stomach, causing loss of appetite.
and
a feeling of fullness after a small amount of food
.
Enlarged thymus Thymus, or thymus gland -
a small organ located behind the upper part of the sternum in front of the heart.
It is where some lymphocytes mature and develop. or lymph nodes in the chest may put pressure on the trachea, which carries air to the lungs. This leads to coughing
,
difficulty breathing, pain
or
heaviness in the chest
.
Brain lesions can cause headaches, weakness, personality changes, and problems with thinking
and
seizures
.
Other types of the disease can spread to the tissues surrounding the brain and spinal cord, causing the patient to see double and have a numb face
and
speech deteriorates
.
Lymphomas of the skin often appear as itchy red bumps
or
cones
.
In addition, symptoms may include:
- weight loss;
- chills;
- night sweats;
- elevated temperature;
- severe fatigue;
- bloating;
- frequent or severe infections;
- Easy bruising or bleeding.
Diagnosis of lymphoma
Most patients see a doctor because they have certain signs of illness or feel unwell. Specialists begin the examination with an examination and questioning about family diagnoses, possible risk factors and other health problems. Then the lymph nodes and other parts of the body that contain lymphatic tissue are examined, including the spleen and liver. After which a number of studies are prescribed:
- Blood tests
: measure the levels of various cells in the blood, detect bone marrow damage, evaluate kidney and liver function, and detect infections and other problems. - Biopsy
is the removal of a piece of suspicious tissue and its transfer to a laboratory for examination. Depending on the course of the disease, doctors may need to biopsy lymph nodes, bone marrow, cerebrospinal fluid, pleural fluid, which is found in the chest, or peritoneal fluid, which is found in the abdomen. - Computed tomography
- allows you to identify foci of the disease in the abdominal cavity, pelvis, chest, head and neck. - Magnetic
resonance
imaging, MRI
, creates a detailed image of soft tissue. The method is usually used to study the spinal cord or brain. - X-ray
– helps detect enlarged lymph nodes in the chest or bones. - Ultrasound, ultrasound
- used to study enlarged lymph nodes or various organs, such as the liver, spleen or kidneys. - Positron
emission
tomography, PET
, can detect lymphomas in enlarged lymph nodes, even those that appear normal on CT. In addition, it can be used to determine whether the disease is treatable.
In the oncology department, a complete diagnosis of lymphoma is carried out - quickly, without queues and loss of precious time, using the most modern equipment. Our specialists guide the patient “from” to “to” – from examination to any treatment.
Advantages of Top Ichilov
- Top-class specialists with unique experience in lymphoma therapy. Despite their already high level of training, our doctors strive to constantly improve their knowledge and introduce the most modern methods into clinical practice.
- Examination of patients at the center is carried out using high-precision equipment, which ensures unsurpassed accuracy of differential diagnosis.
- The clinic's doctors treat lymphoma using a wide range of the latest techniques - from modern highly effective combined chemotherapy regimens to irradiation of patients using external radiotherapy devices.
- By contacting us, the patient does not risk anything, since there is no prepayment, and all payments are made through the medical center’s cash desk.
- The best conditions have been created for patients in the clinic - cozy rooms have everything they need, and a personal curator-translator oversees the coordination of doctors and the translation of medical documents.
- 5
- 4
- 3
- 2
- 1
(5 votes, average: 3 out of 5)
Lymphoma stages
Immediately after detecting the disease, doctors determine its stage - find out how far it has spread and what tissues it has damaged. This information is extremely important for specialists, since it allows not only to understand the patient’s prognosis, but also to select the most appropriate treatment for him.
Stages of Hodgkin lymphoma:
I
: Changed cells are found in only one group of lymph nodes or one lymphoid organ, such as the tonsils.
II
: they are present in 2 or more groups of lymph nodes located on one side of the diaphragm, or have spread from one damaged lymph node to an adjacent organ.
III
: lymphoma cells are present in the lymph nodes on both sides of the diaphragm;
or not only in the lymph nodes above the diaphragm, but also in the spleen. IV
: The disease has spread to at least one organ outside the lymphatic system, such as the liver, bone marrow, or lungs.
Stages of non-Hodgkin's lymphomas:
I
: altered cells are found only in 1 group of lymph nodes or one lymphoid organ, for example, tonsils;
or in 1 area of one organ outside the lymphatic system. II
: they are present in 2 or more groups of lymph nodes on 1 side of the diaphragm;
either in the lymph nodes and 1 area of an adjacent organ, or in another group of lymph nodes on the same side of the diaphragm. III
: lymphoma cells are present in the lymph nodes on both sides of the diaphragm;
or they are present in both the lymph nodes above the diaphragm and the spleen. IV
: The disease has spread to at least one organ outside the lymphatic system, such as the liver, bone marrow, or lungs.
Lymphoma treatment
Treating lymphoma is not an easy task.
To solve it, you need not just one doctor, but a whole team of professionals - a chemotherapist, radiologist, surgeon, oncologist, hematologist and others. The oncology department has all the necessary specialists - world-class doctors who conduct a full diagnosis of the disease and any necessary therapy. With us, you don’t have to retake tests, redo studies and ask the question “what to do next?”
We fully guide the patient and give him a clear action plan, following which he gets the best possible result. Several methods are used to combat this type of cancer:
The main one is chemotherapy
– drugs that destroy altered cells. They are taken in pill form or injected into a vein, enter the bloodstream and spread throughout the body. Treatment is carried out in cycles, each lasting several weeks, followed by a period of rest during which the body recovers.
Bone marrow transplantation
or stem cells from which blood cells are formed. The procedure allows higher doses of chemotherapy, sometimes along with radiation, to be given, which helps kill the lymphoma more effectively. Transplantation is possible not only with donor material, but also with your own material, collected several weeks before the intervention.
Radiation therapy
– destruction of altered cells using radiation. This method is suitable for most patients, and works especially well if the disease has affected a small amount of tissue. It is used both independently and in combination with chemotherapy.
Immunotherapy
– drugs that help a person’s own immune system better recognize and destroy abnormal cells. There are several types used for lymphomas. These include:
- monoclonal antibodies are proteins designed to attack a specific substance on the surface of lymphocytes;
- Immune checkpoint inhibitors - drugs that prevent altered cells from masquerading as healthy ones;
- T-cell therapy: removal of immune cells from the patient’s blood and modification in the laboratory, their reproduction and return to the body, where they find and destroy foci of the disease.
Surgery
: Often used to obtain samples of suspicious tissue and determine its type, but rarely for therapy itself. In rare cases, operations are prescribed for lesions of the spleen or other organs that are not part of the lymphatic system - for example, the thyroid gland or stomach.
Complications and relapse
After treatment for gastric lymphoma, the risk of complications and relapse will depend on which methods were used. After long-term use of antibiotics, drug resistance, allergic reactions, intestinal dysbiosis, intoxication of the whole body or individual organs may appear. When using chemotherapy drugs, the toxic damage will be several times stronger, taking into account the regimens and doses used. There may be a decrease in the number of blood cells, suppressed immunity, damage to peripheral nerves, etc.
If during irradiation of the stomach neighboring organs and tissues are exposed to rays, typical post-radiation complications will be observed. After surgery, early and late undesirable consequences may occur. In the postoperative period the following cannot be excluded:
- bleeding;
- suture infection;
- failure of the gastric stump;
- state of shock;
- peritonitis;
- thromboembolism;
- pneumonia;
- myocardial infarction and other complications associated with surgery for lymphoma or anesthesia.
When visiting a specialized clinic, where modern equipment is used and qualified doctors work, the risk of complications and recurrence of gastric lymphoma is significantly reduced.