Pathology of Meckel's diverticulum
Bibliographic description:
Burlakova, E. S. Pathology of Meckel's diverticulum / E. S. Burlakova. — Text: direct // Research of young scientists: materials of the IX International. scientific conf. (Kazan, April 2020). - Kazan: Young scientist, 2022. - pp. 17-19. — URL: https://moluch.ru/conf/stud/archive/368/15726/ (access date: 03/04/2022).
This article discusses the pathology of Meckel's diverticulum and analyzes the complications caused by this disease. There is a relationship between the features of the anatomical structure and the options for surgical removal of Meckel's diverticulum.
Particular attention is paid to the clinical case of surgical treatment of complicated Meckel's diverticulum with strangulating small bowel obstruction.
Key words: diverticulum, obstruction, complication, perforation, laparotomy.
Meckel's diverticulum (MD) was first described by the German anatomist J. F. Meckel (1781–1833). However, this pathology was known earlier - in 1598, an unusual intestinal extension was discovered by Fabricus Hildanus. But it was Meckel who studied it in detail. The scientist publishes several works (1808–1820), in which he describes the appendage in detail and proves that it appeared in the process of abnormal development of the embryo. DM is one of the most common congenital anomalies of the gastrointestinal tract and the cause of a number of severe pathological conditions. From the point of view of embryology, the DM is a remnant of the vitelline-intestinal duct, which connects the yolk sac of the embryo with the primary intestine and normally undergoes reverse development after 6–8 weeks of the prenatal period. DM is one of the earliest formations in ontogenetic terms. From the point of view of anatomical and topographical features, it should be noted that DM is a protrusion of a section of the ileum of various shapes and lengths, which resembles a vermiform appendix located at a distance of 70–100 cm from the ileocecal angle with the same structure of the intestinal wall and its blood supply being preserved. The frequency of pathology ranges from 2–3%, with clinical manifestations and complications of the disease observed in 25% of cases. The length of the process varies from a few millimeters to 15 cm, and the diameter - from 0.5 cm to 5 cm. Its shape is varied: cylindrical, spherical, worm-shaped. In the abdominal cavity, the DM lies freely or is fixed by a fibrous cord to the navel, intestine, mesentery, etc. [1, p. 104]. Histologically, its wall is built in the same way as the wall of the small intestine, but the muscular layer is less pronounced [3, p. 488].
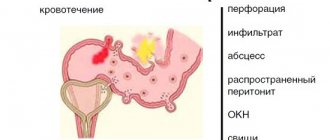
Often, complications develop in children under 10 years of age and in adults over 30 years of age. Diverticulitis is one of the most common complications, observed in approximately 20% of patients with DM. Basically, the complication develops in diverticula with a narrow neck, where food debris accumulates, and later a bacterial infection occurs. There is a possibility of developing diverticulitis as a result of torsion of the diverticulum itself and disruption of its blood supply. [2, p. 74]
Quite often there are ulcerations of the DM, which can cause perforation into the abdominal cavity, thereby causing peritonitis.
Diverticula can contribute to the formation of umbilical pathologies (about 12.5% of cases) - fistulas, cysts, fibrous cords between the diverticulum and the navel. [5, p. 146]
Another dangerous complication of Meckel's diverticulum is intestinal obstruction, which develops due to compression of the intestinal lumen by a diverticulum attached to it. Sometimes the DM fixed to the abdominal wall or to the mesentery forms something like a ring-shaped hernial orifice. As a result of the penetration of intestinal loops through them, internal strangulated hernias can occur.
Intussusception, as a complication, can occur when a diverticulum with a wide base penetrates into the intestinal lumen and, under the influence of peristalsis, moves along with the intestinal chyme, carrying with it the intestine from which it originates.
For patients with intestinal obstruction caused by Meckel's diverticulum, emergency surgery should be considered.
Options for surgical removal of Meckel's diverticulum:
- like a vermiform appendix - with a narrow base of the diverticulum;
– cutting off using a clamp followed by suturing of the ileum with a double-row suture in the transverse direction - in case of a narrow base or inflammation of the diverticulum;
– wedge-shaped excision of the diverticulum between two clamps, followed by suturing of the ileum with a double-row suture - in case of a wide base or inflammation of the diverticulum;
– resection of the ileum with a diverticulum followed by an end-to-end anastomosis - if the intestine is involved in the inflammatory process [4, p. 152].
Patient A., 37 years old, underwent surgery - mid-median laparotomy: elimination of intestinal obstruction, excision of Meckel's diverticulum, nasogastric intubation, sanitation and drainage of the abdominal cavity.
The loops of the small intestine are moderately swollen to 2 diameters, 40–50 cm from the ileocecal angle there is a diverticulum of the small intestine (Meckel), 7 cm long, 3 cm in diameter with a rod pressing on the wall of the ileum; below the rod the intestine is not thickened. The strangulation is cut, the intestinal obstruction is eliminated, the intestine in the area of strangulation is viable. Meckel's diverticulum was excised using clamps (10cm x 3cm), the intestine was sutured with a double-row suture. Sanitation of the abdominal cavity was performed. The patient was discharged after 9 days.
Postoperative care is similar to that for an appendectomy or small bowel anastomosis. Fluid and electrolyte balance is maintained intravenously until the intestines regain their ability to contract. The nasogastric tube is then removed and progressive feeding begins. Any residual inflammation, peritonitis, or drained abscess is treated with appropriate general antibiotics and blood and plasma replacement.
The above clinical case proves that Meckel's diverticulum may be one of the causes of acute intestinal obstruction. Consequently, knowledge of such anatomical anomalies as DM and the principles of its surgical treatment makes it possible to eliminate the complications caused by it.
Literature:
- Noskov A. A., Lazarev S. M., Efimov A. L., Ershova N. B., Chepak D. A. A rare observation of a giant Meckel’s diverticulum // Bulletin of Surgery named after. I. I. Grekova. 2016. No. 1. - pp. 104–105.
- Pimenov I. A., Oganesyan M. V., Merenkova I. V. Meckel’s diverticulum: anatomical features and localization options [Electronic resource] // International Student Scientific Bulletin. 2017. - No. 5. Access mode URL: https://eduherald.ru/pdf/2017/5/17335.pdf (02/14/2020)
- Littman I. Operative surgery: atlas. - Budapest: Publishing House of the Hungarian Academy of Sciences. - 1985. - 1143 p.
- Zhuk I. G. Topographic anatomy and operative surgery: textbook. — Grodno: Grodno State Medical University. - 2012. - 269 p.
- Klimov A. E., Cherepanov D. E. Cases from practice: two cases of complications of Meckel’s diverticulum // Bulletin of RUDN University, Medicine series. — 2003. — No. 3. — P. 146
Key terms
(automatically generated)
: ileum, diverticulum, intestinal obstruction, abdominal cavity, double-row suture, small intestine, subsequent suturing, surgical treatment, appendix, wide base.
Statistics
According to the frequency of congenital diseases in children, Meckel's diverticulum occurs in 2% of cases. The incidence of complications with this developmental anomaly is 5–7% of cases. In half of the cases in children under 2 years of age, diverticulum is symptomatic. When comparing data, the frequency of this developmental anomaly in boys is almost 3 times greater than in girls.
Statistics show that Meckel's diverticulum most often forms in parallel with other developmental anomalies and genetic diseases of the gastrointestinal tract:
- omphalocele – remnants of the vitelline duct (10 times);
- esophageal atresia – lack of connection between the stomach and esophagus (6 times);
- anorectal anomalies (5 times);
- Crohn's disease (3 times);
- various neurological diseases (3 times).
Treatment methods and prevention
There are not many methods for treating Meckel's diverticulum; one can say that this is surgical removal of the diverticulum. But there are many contradictions in the opinion of doctors regarding the removal of uncomplicated diverticulum. Such a diverticulum can be detected during various operations on the abdominal organs. And then the question arises: “To delete or not?”
There are many opinions and studies that Meckel's diverticulum is removed in all cases. A comparative analysis was carried out, comparing patients with complicated and uncomplicated diverticulum. This analysis found that children with complicated diverticula had much larger diverticulums. Using this analysis, it can be determined that the lifetime risk of developing complications is 6% for all ages.
There are 2 types of surgical treatment for Meckel's diverticulum.
- A median laparotomy is performed. This approach is used when the length of the diverticulum is less than 3 cm and it has a wide base. The diverticulum is resected along with part of the small intestine, followed by enteroanastomosis. This method avoids leaving part of the ectopic gastric mucosa, which can cause postoperative complications.
- Laparoscopy. Less invasive method for removing diverticulum. Indications for this method are a diverticulum length of more than 5 cm and a narrow base.
In surgical practice, there are 2 methods of resection of Meckel's Diverticulum using the laparoscopic method.
- Place a ligature at the base of the diverticulum if there are no changes (tumor) there.
- Use the endoscopic stapler ENDO-GIA 30 with a 12 mm trocar.
When using these 2 methods, the operation time is reduced and the recovery period is faster. For preventive purposes, children can undergo physical therapy and tummy massage. Avoid cases of constipation in children; this prevention will help avoid dangerous complications.
Diagnostics
Scintigraphy , a radionuclide isotope method, is the primary method for diagnosing Meckel's diverticulum in children complicated by bleeding. This method is based on radioactive isotopes that are attracted to and collected from ectopic cells located in the gastric mucosa. If scintigraphy results are negative and bleeding continues, diagnostic laparoscopy should be performed.
With this research method, the results can be false positive and false negative. The presence of a duodenal ulcer, intestinal duplication and vascular tumor means the result is false positive. The minimum content of ectopic gastric mucosa in the diverticulum means the result is false negative.
X-ray is the best way to detect intestinal obstruction and diverticulum perforation. This method is performed using a contrast agent (barium suspension).
Discussion
Surgery for Meckel's diverticulum is one of the least studied areas of abdominal diseases, especially in the adult population. Research conducted in recent years has shown the difficulty of diagnosing this pathology, which can have a hidden course and be complicated by such serious complications as intestinal bleeding. Modern development of medicine involves the use of high-tech diagnostic equipment in clinical surgery. The introduction of video capsule endoscopy for the study of the small and large intestines facilitates the diagnosis of many diseases, especially bleeding from the lower gastrointestinal tract. But many medical institutions do not have the equipment to conduct this type of examination. Therefore, when diagnosing small intestinal bleeding, one must rely on the objective condition of the patient, clinical picture, laboratory research methods, as well as the knowledge and experience of surgeons treating patients with this pathology.