Gallstone disease (GSD) is the formation of stones in the cavity of the gallbladder and ducts. The gallbladder is an organ that is a hollow “sac” with a volume of up to 60 ml, into which bile synthesized by the liver flows. In the bladder, bile is concentrated and becomes a participant in the digestive process. Through the ducts, through the duodenum, viscous black-green bile enters the food mass, where it emulsifies fats and participates in other biochemical processes. Stones in the bile duct (choledocholithiasis) can form independently or be thrown from the bladder.
Main types of stones
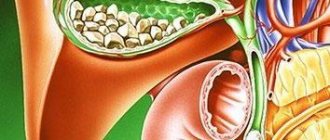
Gallstones vary in size, shape, color and chemical composition.
Size
. There are no large single stones in the common bile duct (common bile duct), which is due to the diameter of the cystic duct. Smaller ones are lighter and leave the bladder with a flow of bile. Large ones remain at the bottom under their own weight.
Form.
If stones with “edges” are found in the ducts, it can be argued that they came from a bladder: this shape appears from the close adhesion of the stones to each other. Basically, the shape of bile formations is round, oval.
Color
depends on the chemical composition:
- cholesterol - predominantly yellow, greenish, golden in color;
- bilirubin (pigment) - soft and black in color;
- calcium (calcareous) formations are whitish, sometimes their surface is like an egg shell;
- with parasitic or bacterial infection - brown.
The classification is based on the predominance of one of the chemical elements. At the same time, the other two are also present. In addition to the main ones, dead cellular elements, protein parts and other components are mixed into the structure.
Prevention of pathology
To prevent the formation of stones in the liver, you need to lead a healthy lifestyle, eat right, avoid fatty and fried foods, and drink plenty of fluids. If there is a hereditary predisposition to the pathology, you should carefully monitor your health. It is recommended to periodically do blind probing - eating food or medications that promote the expansion of the bile ducts, the release of bile and small stones. But this type of prevention should be discussed with your doctor.
Mechanism of formation of gallstones
When there is a metabolic disorder and an increase in the amount of cholesterol in the blood, the bile is also oversaturated, and crystals are deposited, which merge with each other and attach protein, calcium and bilirubin molecules to themselves. A round body is formed, similar to a small stone. When the gallbladder contracts, the calculus is released into the cystic duct and then into the common duct. The cholesterol type is the most common. Stones appear directly in the ducts most often in patients whose gallbladder has already been removed.
Bilirubin is formed during cirrhosis of the liver or chronic conditions that lead to the breakdown of red blood cells - red blood cells. The level of bilirubin pigment in the blood and bile increases. Reacting with calcium, it forms compounds that crystallize and become the basis of black gallstones. More often observed in children.
In people living in poor hygienic conditions and suffering from helminthic infestations, the parasite (often roundworms or Chinese fluke) enters the duodenum into the common bile duct, where it becomes overgrown with bilirubin and calcium salts.
Causes of stone formation:
- unhealthy diet leading to increased blood cholesterol;
- liver diseases;
- metabolic disorders;
- conditions leading to the destruction of red blood cells;
- hereditary factors;
- helminthic infestations;
- removed gallbladder and others.
Women get sick more often than men, and young people less often than older people.
Why do they appear?
The formation of stones in the liver is due to the physicochemical and physiological properties of the environment. If it is impossible to dissolve organic or inorganic compounds that are in bile, suspended substances precipitate. It is believed that the formation of sediment occurs as a result of metabolic disorders, which can be congenital or acquired (poor nutrition, destructive processes, poisoning).
Stones can form in the liver and bile ducts due to a sedentary lifestyle, due to dietary habits, fever, and climatic conditions. A prerequisite for the formation of a calculus is a violation of the secretory and resorptive activity of the organ, stagnation of bile or inflammatory processes.
It is believed that due to strictures of the bile ducts, bile stagnation occurs in the gland, the motility of the ducts is disrupted and atony develops, which leads to the formation of an abscess, biliary cirrhosis, and sepsis. When bile secretion is impaired, the concentration of dissolved substances in the bile increases, but they cannot be excreted because there is no component that should bind them, as a result, they precipitate.
With inflammation, stagnation of liver secretions occurs, and this also leads to sedimentation, changes in salt solubility and deterioration in the functioning of protective colloids. The stones are divided into a core and a layer. The core of any stone is an organic or colloidal substance (desquamated epithelium, leukocytes, thick mucus, fibrin, protein sediment, bacteria) on which inorganic compounds are layered over time.
The composition of the stone formation also determines its strength (it can be soft, like compacted sand, or very hard)
At first, the stones are small, the size of crystals or grains of sand, but gradually they become covered with salts and increase in size. Even small single formations can disrupt the flow of bile, and once they get into the gland duct, they can clog it, which will provoke a disruption of the digestive process and an inflammatory reaction.
Stones in the human liver can be formed from bile pigment, calcium salts, and cholesterol. They can be round, oval, or polygonal. Their color depends on their composition, for example, cholesterol stones are yellow, and bilirubin stones are brown or black (as in the photo below). The size of the formation can be up to 3 cm. Stones in the liver grow relatively slowly, increasing by about 10 mm in six months.
Most often, cholesterol stones are formed; stones from phosphorus or calcium carbonate are extremely rarely formed. For the formation of cholesterol stones, three factors must be met: excess cholesterol in the bile, its precipitation in the form of crystals and impaired liver function.
Thanks to bile acids and phospholipids, cholesterol in bile is in a dissolved state; if cholesterol-retaining factors are insufficient, it precipitates. Sometimes bile becomes lithogenic due to increased secretion of cholesterol, which occurs with obesity, hypothyroidism, diabetes, pregnancy, and fatty hepatosis.
Any pathology that leads to metabolic disorders in the liver can trigger the process of stone formation in the liver. This may be obesity, inflammatory processes both in the liver itself and in other organs, for example, the bladder, urinary tract, pancreas. Pigment stones appear in the gland if the patient's red blood cells are rapidly destroyed (thalassemia or sickle cell anemia).
Liver stones can grow due to increased levels of bad cholesterol in the diet (eating fried, fatty, smoked foods), alcohol abuse, and hormonal disorders.
Symptoms of choledocholithiasis
The disease is asymptomatic as long as the stones are freely evacuated through the duodenum and intestines. Severe symptoms occur when the lumen of the common bile duct closes. It is similar to the signs of cholecystitis:
- intense pain in the right hypochondrium, radiating to the back. When the area of the papilla of Vater (the place where the ducts from the gallbladder and pancreas flow into the duodenum) is blocked, it becomes the surrounding papilla. Drawing, aching, dull, sometimes sharp;
- alternately increasing and decreasing yellowness of the mucous membranes and skin. The first yellowing occurs 10-12 hours after the onset of pain;
- light yellow or white stool;
- dark brown urine;
- Body temperature may rise.
The pain subsides when the stone passes into the duodenum and the bile flow is restored. When the next stone migrates, the whole picture will repeat itself. The condition gets worse if inflammation begins.
Diagnosis of the disease
The diagnosis is made based on a medical examination; anamnesis collected through questioning and studying medical documentation about previously performed operations and manipulations; laboratory diagnostics; instrumental research.
Based on the results of laboratory diagnostics, one can judge the stage of the disease, the presence or absence of an inflammatory process, damage to the pancreas, and so on.
The instrumental methods include the following:
- Ultrasound examination (ultrasound) of the abdominal organs - performed through the skin of the abdomen;
- MRI cholangiography. All ducts, location and size of stones are visible on a computed tomograph;
- computed tomography (CT) allows you to see neoplasms or other organic external causes of narrowing of the ducts;
- Videodoudenoscopy allows for a detailed examination of the area of the papilla of Vater.
The method of instrumental examination is chosen by the doctor depending on the patient’s condition, symptoms and medical history.
General principles of liver surgery
An unspoken rule in hepatology is that removal of more than 70% of organ tissue with healthy or more than 60% with impaired liver function leads to severe postoperative complications. This is due to the inability of the remaining part of the liver to cope with its metabolic responsibilities.
Technical problems during liver interventions are caused by several factors:
- the difficulty of creating full operational access to the organ;
- rich blood supply to the liver, leading to an increased risk of massive bleeding;
- a large number of tubular structures (vessels, bile ducts) requiring ligation before intersection;
- The soft consistency of the organ makes its suturing difficult.
To level out these difficulties, a number of operational methods and techniques are used. Firstly, during surgical interventions on the liver, special instruments are used: costal retractors, electrocoagulators with additional attachments and knives, ultrasonic destructors-aspirators, vascular clamps for the hepatic veins, clippers for vessels and bile ducts, devices for reinfusion (reverse infusion) of blood, hemostatic films and sponges.
Secondly, to ensure a good field of activity, they resort to special surgical approaches. They involve large incisions running both along the right side of the chest and along the anterior abdominal wall. There are more than 70 modifications of access to the liver (according to Quino, Petrovsky-Pochechuev, Borovsky and others). Most of them are traumatic, and some involve resection of sections of the ribs.
The choice of access is carried out individually, based on the volume of the planned resection. However, the bisubcostal approach with vertical extension is generally accepted and the most convenient. It involves incisions under the costal arches and along the midline of the abdomen. The xiphoid process of the sternum is removed. The main advantages of this access are ease of operation for any type of operation and a wide working field for surgeons.
Thirdly, surgical technique on the liver involves the use of special techniques. For example, special hemostatic sutures are used to close a wound. They are performed with a blunt-tipped atraumatic needle and thread. For quick and durable suturing of blood vessels or bile ducts, clippers can also be used. During surgery, intraoperative ultrasound examination of the liver and other invasive research methods are also often used.
Treatment
Removing a stone from the bile duct cannot be done with medication or other non-invasive methods. The optimal method for diagnosing and treating choledocholithiasis is ERCP (Endoscopic retrograde pancreatic cholangiography). Using an X-ray contrast agent introduced through an endoscope, the condition of the biliary system can be assessed using a series of images. If the diagnosis is confirmed, the endoscopist surgeon immediately makes a decision on treatment. Large stones are crushed. When the area of the papilla of Vater narrows, it is dissected. The advantages of the technique are that there is no need to move the patient between examination and treatment procedures - everything takes place in one operating room, on one equipment, by one doctor.
If ERCP is impossible or ineffective, laparoscopic surgery is performed. Stones in the bile ducts are removed mechanically, after dissecting the wall of the duct. The gallbladder is also removed. In difficult cases, they resort to classical abdominal surgery.
Pathogenesis
Liver stones form by two mechanisms. This process is called lithogenesis and can be primary or secondary.
Primary lithogenesis carries with it a functional disorder in the formation of bile. This type of cholelithiasis may not manifest itself for a long time and makes itself felt only when another pathology is added that narrows the bile ducts and makes it difficult for the stones to pass out.
Secondary lithogenesis is the result of cholestasis (stagnation of bile).
If the bile duct blocks a stone in the liver, the external manifestations correspond to the clinical picture of obstructive jaundice. This is facilitated by infection and connective tissue scars.
Consequences of choledocholithiasis
After treatment and following the doctor’s recommendations, the patient quickly returns to his normal life. However, if you do not seek medical help promptly, complications may arise.
- The presence of stones provokes inflammatory processes that are severe and painful.
- Since the bile and pancreatic ducts connect before entering the duodenum, if the mouth is blocked by a stone, the ducts become swollen and damage to the pancreas is possible. Acute pancreatitis can result in the death of the patient.
- Communicating with the liver, the inflamed biliary system disrupts the functional activity of this organ (and the liver participates in digestion, hematopoiesis, deposits necessary substances, utilizes and deactivates unnecessary ones, and so on). As a result, there is an imbalance in the functioning of almost all body systems.
Anesthesia
Before surgery, the patient must be examined by an anesthesiologist. He assesses the general condition and the possibility of performing the operation, and also predicts the course of general anesthesia (anesthesia) and possible risks from it.
For liver operations, multicomponent inhalation endotracheal anesthesia is used. For anesthetic management, several groups of drugs are used that selectively affect body functions (suppression of consciousness, sensitivity, memory, pain relief).
The choice of drugs for inducing anesthesia and maintaining it is one of the important stages of preparation for surgery. The anesthesiologist approaches this process with great responsibility, since some anesthetics inhibit liver function and can lead to or aggravate existing functional failure of the organ.
Why is it important to consult a doctor at the first symptoms?
Since choledocholithiasis often has an asymptomatic course, the onset of the inflammatory process can be missed. Trying to get rid of pain or other symptoms on their own, a person wastes time, and this is absolutely forbidden to do, in order to avoid the development of irreversible processes. This is especially true for patients with a removed gallbladder. Timely diagnosis and treatment ensures a favorable outcome.
The Yusupov Hospital has all the conditions for high-quality diagnostics and treatment. Here you can conduct a preventive examination if you have had a cholecystectomy in the past or if there are cases of cholelithiasis in the family.
Recovery period
The course of the postoperative period largely depends on the general health of the patient and the functional state of the remaining part of the liver. In the early postoperative period, the patient is in the intensive care unit under the close supervision of medical personnel. The main tasks at this stage are:
- maintaining vital functions;
- adequate pain relief with narcotic and non-narcotic analgesics;
- monitoring liver function;
- prevention of postoperative complications;
- postoperative wound care and drainage;
- adequate infusion and transfusion therapy;
- parenteral administration of balanced nutritional mixtures, and then a gradual transition to a normal healthy diet.
In the early postoperative period, the patient should remain in bed, devote more time to rest, and adhere to all recommendations of the attending physician. In late rehabilitation periods (more than 1 month after surgery), the patient can return to their usual lifestyle with restrictions on physical activity and nutrition. In addition, during this period a full control examination of the main organ systems, the liver and its functional activity is required.