Alcoholism leads to poor health. The liver often suffers the most. Read below about what cirrhosis is, how to treat it, and what symptoms appear during the disease.
- Read in the article:
- Alcoholic cirrhosis of the liver: what is it?
- Causes of the disease
- Risk factors
- Symptoms
- Stages of liver cirrhosis: stages of damage
- Types of cirrhosis
- Small-knot
- Beer cirrhosis
- Toxic
- Complications of alcoholic cirrhosis
- Jaundice
- Ascites
- Anemia
- Brain intoxication
- Stars on the body
- Hallucinations
- Treatment methods for alcoholic cirrhosis
- Diagnosis of the disease
- Drug therapy
- Diet
- Recovery period
- Treatment of alcoholism in
- Detoxification
- Drug treatment
- Rehabilitation of an addict
Content:
- General information about the disease
- Causes of pathology
- How the disease develops
- Types of pathology
- Signs of alcoholic cirrhosis
- What does the disease lead to?
- Examination for suspected alcoholic cirrhosis
- Quitting alcohol is a prerequisite for recovery
- Complex treatment of liver cirrhosis caused by alcoholism
- What prognosis do doctors give for cirrhosis?
Does alcohol cause cirrhosis of the liver? Unfortunately, the answer is yes. Today this fact is no longer in doubt.
Alcoholic cirrhosis of the liver occurs in both men and women. The disease occurs in response to the destruction of liver cells of hepatocytes, as a result of which they are replaced by dense connective tissue.
For this disease, it is important to start treatment at an early stage. If the disease goes very far, the alcohol addict will most likely die.
Stages and forms of cirrhosis
The first signs of ADC appear after several years of regular drinking. Long-term intake of 50 g by men and 20 g of ethanol by women leads to structural changes in parenchymal tissue. Depending on the degree of functional impairment of the organ, the following stages of portal cirrhosis are distinguished:
- compensated - there are no signs of pathology, which is explained by the intensive functioning of the surviving hepatocytes;
- subcompensated - a significant part of the liver cells die, as a result of which the functioning of the organ is disrupted; The following symptoms indicate dysfunction of the digestive gland: loss of appetite, abdominal pain, fatigue;
- decompensated - necrosis of most hepatocytes is observed, as indicated by manifestations of liver failure: portal hypertension and yellowing of the skin;
- terminal - the last stage of the disease, accompanied by fatal complications: hepatic encephalopathy, edematous-ascitic syndrome, hepatic coma.
The rate of progression of ADC is determined by the frequency of binges, the strength of alcoholic beverages and their quantity.
Systematic consumption of alcohol leads to the development of degenerative processes in the liver tissues. Under the influence of ethanol, necrosis of hepatocytes occurs faster than their regeneration. After a short time, the destroyed liver cells are replaced by connective tissue, which is not able to perform a neutralizing function in the body.
Can cirrhosis be cured? The pathology is accompanied by irreversible changes in tissues, so it is almost impossible to cure a cirrhotic liver in alcoholism. In the best case, if a patient abstains from alcoholic beverages, he can live from 1 to 12 years, depending on the stage of the disease.
General information about the disease
Alcohol and liver cirrhosis are interrelated concepts. As a result of regular drinking, hepatocytes are damaged and liver failure develops. In women, it progresses faster, which is associated with increased levels of estrogen hormones.
It is impossible to say for sure how long people live with cirrhosis of the liver. But, if the disease reaches a terminal stage, death is recorded within about six months. To save life, an alcohol addict needs to undergo comprehensive treatment for alcoholism and undergo a liver transplant.
License and certificates:
Toxic
Occurs from drinking alcohol, exposure to toxins, such as taking medications or working in chemical-related industries. The structure of the liver tissue changes - healthy areas are gradually replaced by scar formations.
Causes of pathology
Symptoms of the disease occur in response to regular alcohol intake. But this does not mean that all alcohol addicts face the disease. Statistics show that only about 35% of patients have to be treated for liver pathology.
This allows us to talk about the need to combine several provoking factors at once, including:
- genetic predisposition to the disease;
- poor nutrition;
- drinking large amounts of alcohol;
- protein deficiency;
- advanced vitamin deficiency.
Possible complications and future prognosis
There is no complete cure for cirrhosis, except for an organ transplant. But the latter option is too expensive and difficult to implement, so it is not available to everyone.
If the pathology is detected at the initial stage and the correct treatment regimen has been drawn up, then the patient can hope to stop the destructive process. Then, most likely, serious complications will not occur or will occur much later. But in practice, patients have to regularly take hepatoprotective drugs after a full course of therapy in order to prevent negative consequences and somehow support the liver. And it is unlikely that it will be possible to restore damaged cells.
People with chronic cirrhosis live no more than 3 years. Therapy only helps relieve acute symptoms, but does not cure.
How the disease develops
Once ethyl alcohol enters the human body, it begins to break down. For its rapid metabolism, the liver secretes special enzymes. The more often a person drinks, the more actively the organ has to work. At some point, the hepatocyte membranes become damaged. The vascular endothelium changes its structure. Then their lumen narrows. A complete supply of liver tissue with oxygen and important elements becomes impossible.
These processes activate the accelerated formation of fibrous tissue, which gradually replaces necrotic areas of the liver. The latter ceases to cope with its basic functions - hematopoietic, protein-forming, detoxifying.
The described processes are irreversible. This means that it is impossible to remove large amounts of connective tissue from the liver using a conservative method. Only a transplant will help here. But this operation is very complex and expensive. Problems often arise with finding a donor organ - many addicts simply do not live to see this moment.
Complications of cirrhosis
If you do not start treating liver cirrhosis at the initial stage of development, it leads to the development of serious pathologies. Some violations are irreversible. The methodical destruction of liver tissue negatively affects the entire body.
Jaundice
Due to the course of pathological processes in the liver, a large amount of bilirubin is formed in the body. Normally, bilirubin is formed in the liver and spleen from hemoglobin, then the liver converts it into bile and removes it from the body. With jaundice, the process is disrupted, so bilirubin remains in the blood, being slightly excreted through the kidneys and skin.
Leave a request for a free consultation with a specialist
we will contact you as soon as possible
- Anonymously
- For free
- Around the clock
Submit your application
Or call: +7 (495) 127-02-03
Ascites
During cirrhosis, ascites forms in the abdominal cavity of a sick person, in other words, an accumulation of fluid in the abdomen. At the same time, the abdomen greatly increases in size, and the venous network on the skin differs.
Anemia
With cirrhosis, there is a decrease in hemoglobin content, as well as a decrease in the number of red blood cells, leading to a decrease in the supply of oxygen to tissues. For this reason, anemia develops, characterized primarily by severe weakness.
Brain intoxication
When the liver malfunctions, toxins enter the brain and have a negative effect on the central nervous system. Encephalopathy is expressed by various psychological and neurological disorders: decreased mental abilities leading to personality degradation, decreased concentration, and loss of orientation in space.
Stars on the body
With liver pathology, one of the symptoms in patients is spider veins on the body. They often appear on the cheeks or back. They appear when there is a metabolic disorder. With advanced cirrhosis, even with minor mechanical impact, a bruise may appear on the skin. All this is due to the fragility of blood vessels.
Hallucinations
When the liver is destroyed, the nervous system suffers and brain cells are damaged. Due to the impossibility of normal brain function, mental abnormalities appear, which are expressed in changes in behavior and a decrease in intelligence. Often, patients with cirrhosis can see hallucinations, which only worsen the course of the disease.
Video about liver cirrhosis, Elena Malysheva’s program, told by Professor, Doctor of Medical Sciences Sergei Vladimirovich Gauthier
Sergey Vladimirovich Gauthier - Head of the Department of Transplantology and Artificial Organs of the First Moscow State Medical University named after. THEM. Sechenova, Chairman of the All-Russian public organization "Russian Transplant Society", Honored Doctor of the Russian Federation
Types of pathology
Doctors classify liver cirrhosis caused by alcoholism into:
- small-knot;
- large-knot;
- mixed.
According to severity, the disease is:
- Compensated. There are no obvious signs of cirrhosis yet. To make a correct diagnosis, a biopsy is necessary. This is a diagnostic procedure during which a fragment of an organ is surgically removed to further study the extent of its damage and inflammation.
- Subcompensated. Signs of liver failure at this stage are clearly expressed. But the damage is still reversible. This means that if the patient begins to lead a healthy lifestyle and follows all medical prescriptions, further liver destruction will not occur.
- Decompensated. The organ becomes unable to function and its failure is recorded. Only transplantation can help here. If it is not carried out, the person will soon die.
Stages of the disease
Liver cirrhosis occurs in several stages:
- Compensated stage. At this stage, the symptoms of the disease do not appear, the organ is still coping with its work. Pathology can only be detected after a biopsy procedure
- Subcompensated stage. At this stage, initial symptoms of liver failure are noted. Laboratory tests will help identify abnormal liver function tests.
- Decompensated stage. Here there is a complete disruption of the liver and damage to other organs
Signs of alcoholic cirrhosis
How the disease manifests itself directly depends on its stage. If we are talking about the compensated stage, then the alcohol addict feels relatively well. If he has any ailments, he “attributes” them to acute ethanol intoxication. The drinker is in no hurry to see a doctor, because he does not know that his liver is in danger. Thus, it creates optimal conditions for the further progression of cirrhosis.
From the start of the abnormal process to the appearance of the first “talking” symptoms, as a rule, at least three to five years pass. You can suspect something is wrong at an early stage only if the organ greatly increases in size. But this doesn't happen often.
At the subcompensated stage, active tissue fibrosis is recorded.
Then the addict begins to complain about:
- lack of appetite;
- a sharp decrease in body weight;
- severe weakness;
- frequent nausea, vomiting;
- negative dyspeptic symptoms.
When palpating the area of the right hypochondrium, the doctor immediately detects an enlarged liver.
At the stage of decompensation, liver functions begin to fade. Then the manifestations of the cirrhotic syndrome complex are recorded, including:
- Asthenic syndrome. It manifests itself as increased fatigue, decreased appetite, and persistent depressive mood.
- Cachexia. We are talking about severe exhaustion.
- Arterial hypertension. Periodically, the patient’s blood pressure “jumps.” His nose, feet and palms remain unnaturally red all the time.
- Hormonal disbalance. In men, the production of female sex hormones estrogen increases. As a result, active deposition of fat occurs in the chest, abdomen, and buttocks. The male genital organs gradually atrophy.
White streaks on the nail plates, often appearing and slowly passing bruises on the limbs and torso also indicate liver problems. Some alcoholics' fingers become like drumsticks.
Clinical picture
In most cases, signs of liver cirrhosis in alcoholics appear after 5-7 years of regular drinking. In medical practice, cases of asymptomatic development of ADC have been reported for more than 15-20 years. At the compensation stage, there are no clinical manifestations of the disease. However, with extensive damage to the digestive gland, multiorgan disorders occur that negatively affect the patient’s well-being.
General manifestations
The first symptoms of alcoholic cirrhosis of the liver appear at the stage of subcompensation. The surviving hepatocytes cannot fully perform the functions of the destroyed liver cells. In this regard, the following clinical manifestations of ADC arise:
- muscle weakness;
- sleep disturbance;
- pain in the right hypochondrium;
- chronic fatigue;
- fever;
- darkening of urine;
- loss of appetite;
- memory loss.
The symptoms of liver cirrhosis in women differ little from the manifestations of the disease in men. Specific signs include menstrual irregularities and intermenstrual uterine bleeding, as well as tearfulness and depression. At the stage of decompensation, there is a sharp decrease in body weight and hair loss in the armpit area.
Symptoms of liver failure
Alcoholic cirrhosis of the liver is accompanied by damage to the parenchyma and dysfunction of the organ, which leads to the development of liver failure. Failures in metabolic processes lead to the development of acute metabolic stress. The accumulation of toxins and ethanol in the body leads to hepatic encephalopathy and, as a consequence, cognitive disorders.
The development of liver failure and encephalopathy is the basis for performing a digestive gland transplantation operation.
The development of liver failure is indicated by:
decreased appetite;- aversion to food;
- yellowing of the skin;
- stool discoloration;
- dementia;
- hypertrophy (enlargement) of the liver;
- spider veins on the chest and face;
- hemorrhagic diathesis;
- tremor of the limbs;
- loss of consciousness.
“Male” cirrhosis is characterized by decreased potency, testicular atrophy and the formation of mammary glands. Due to lipid metabolism disorders, fat deposits occur in the lower abdomen and thighs.
Symptoms of peripheral neuropathy
With alcohol intoxication of the body, the development of so-called peripheral neuropathy is possible. The pathology is characterized by damage to peripheral nerves, vegetative-vascular disorders and decreased sensitivity of the distal limbs, i.e. hands and feet.
A large amount of alcohol in the blood leads to dysfunction of the central and peripheral nervous systems. Damage to nerve fibers is accompanied by a violation of vascular tone and, as a consequence, deformation of the capillaries. This is why telangiectasia occurs in patients suffering from alcoholism.
When peripheral neuropathy manifests itself, patients usually complain of:
- blurred vision;
- violation of temperature sensitivity;
- decreased tactile sensations;
- causeless weakness in the hands.
Over time, pathological processes in the nerves progress and spread proximally. In other words, a decrease in tactile, pain and temperature sensitivity extends to the entire body.
Symptoms of portal hypertension
Alcoholic cirrhosis of the liver leads to the formation of connective tissue cords in the organ, which prevent the outflow of venous blood from the portal system. In this regard, the hydrostatic pressure in the hepatic capillaries increases, which entails a number of complications, which include:
- splenomegaly - hypertrophy (enlargement) of the spleen, provoked by impaired blood circulation in the splenic veins;
- abdominal dropsy - accumulation of intercellular fluid (exudate) in the peritoneum caused by circulatory disorders in the portal vein;
- internal bleeding - hemorrhage in the intestines, duodenum or stomach, caused by varicose veins and increased blood pressure.
Hemorrhagic syndrome develops almost asymptomatically; bleeding of the veins is indicated by the staining of stool in a dark red color.
What does the disease lead to?
If you do not consult a doctor and find out how to treat alcoholic cirrhosis, numerous complications will not keep you waiting:
- complete and irreversible liver failure;
- varicose veins of the esophagus;
- internal bleeding;
- portal hypertension;
- ascites;
- enlargement of the abdomen and the appearance on its surface of a venous pattern resembling the head of a jellyfish;
- peritonitis;
- severe intoxication of the body;
- fainting;
- brain damage;
- pancreatitis;
- peripheral polyneuropathy;
- growth of malignant liver tumors, including hepatocellular carcinoma.
Treatment
When treating alcoholic cirrhosis of the liver, it is necessary to strictly adhere to the diet. Adjusting your diet will help stop the development of the pathological process, but will not help get rid of the disease.
The use of pharmaceuticals in the treatment of the disease should not become an additional burden on the damaged organ.
To eliminate intoxication, doctors may prescribe:
- Enterosorbents, Polysorb or Enterosgel are perfect
- Intravenous administration of Rheosorbilact, glucose and Ringer's solution
Sorbents will help quickly cleanse the intestines of toxins.
Glucocorticosteroids help suppress the breakdown of liver cells and immune mechanisms. These medications, depending on the patient’s well-being, can be administered intravenously or intramuscularly.
Hepatoprotectors (Essentiale, Ursofalk, Ursosan) are necessary to protect cells that have not yet undergone fibrosis.
To maintain the digestive process, the patient needs pancreatic enzymes, most often doctors prescribe Panzinorm, Creon.
To reduce pressure in the portal vein, Nitrosorbide and Anaprilin are required. In case of severe swelling or enlargement of the abdomen, the patient will need diuretics (Veroshpiron, Furosemide)
For the purpose of replacement, the following is prescribed:
- Stimol
- B vitamins
- Albumin solution, platelet and erythrocyte masses
The duration of the course and dosage of the drugs should be determined by the attending physician. Self-medication can lead to negative consequences.
Examination for suspected alcoholic cirrhosis
The patient is asked to undergo diagnostic testing if symptoms of liver damage are observed. He undergoes laboratory tests and undergoes an ultrasound. During an ultrasound examination, the following is recorded:
- changes in the size and structure of the liver;
- fibrous lesions;
- inflammation.
Additionally, the patient undergoes an MRI or CT scan of the abdominal organs. These techniques make it possible to obtain layer-by-layer images of the liver, to study the condition of its passages and veins.
Very informative are:
- Puncture. The procedure is performed under anesthesia. The doctor receives a sample, which is subsequently examined under a microscope.
- Elastography. Ultrasound examination showing the amount of connective tissue. Based on its results, you can unmistakably understand how far cirrhosis has progressed.
Hospital at home
22,000 months
- Home visit
- Anonymous consultation with a narcologist
- Examination by a narcologist
- Dropper capacity 1900 ml
- Therapy in tablet form
- Vasodilators
- Anticonvulsants
- Metabolic solutions, vitamins
- Antiarrhythmic
- Sedatives and pain relievers
- Duration - 24 hours
- The doctor is with the patient
- Relevant for binge drinking from 5 days
Order service
Toxic
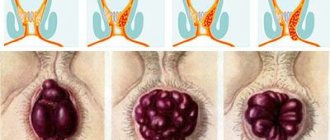
Severe chronic liver damage is characterized by the formation of larger nodes and compactions. They can be of different diameters, from 5 mm. The structure of the liver is greatly changed, gradually healthy tissues are replaced by diseased ones.
Quitting alcohol is a prerequisite for recovery
No matter how diligently an alcohol addict is treated for cirrhosis, he will definitely not become healthy until he gives up alcohol. Alcoholics usually cannot do this on their own - the craving for drinking is always too strong. Therefore, it is important to contact a qualified narcologist.
The doctor will prescribe a detoxification course that will cleanse the body of ethyl alcohol breakdown products and select the optimal coding option. Most likely, this will be psychotherapeutic coding (hypnosis or Dovzhenko’s stress therapy), since even the most gentle drug correction increases the load on the liver, which is extremely undesirable.
Course of the disease
Initially, the liver manages to cope with periodic ethanol attacks by producing a sufficient amount of enzymes. But the organ cannot constantly work in such an enhanced mode, and over time its strength runs out, and the walls become overgrown with a layer of fat. This is called fatty liver disease. Soon the hepatocides die, and they are replaced not by healthy cells, but by modified tissue structures. As a result, the structure of the liver changes, which leads to complete degradation.
Liver cirrhosis of alcoholic etiology develops quickly and according to a simple algorithm. During the processing of ethanol breakdown products, toxic substances are released, causing the following:
- injury to cell membranes;
- cell destruction;
- vascular damage and spasms;
- lack of oxygen in the organ;
- increased death of hepatocides.
Against the background of this pathology, the liver gradually stops working normally.
All of the above changes are total and cannot be corrected. A person with such dysfunctions becomes disabled, with possible death.
Complex treatment of liver cirrhosis caused by alcoholism
Doctors from various specialties take part in the fight against the disease. Usually this is a therapist, hepatologist, surgeon, gastroenterologist, narcologist. If necessary, the patient is prescribed consultations with other specialists.
The patient is told to strictly adhere to therapeutic diet No. 5. It involves consuming foods that contain large amounts of protein, vitamins and minerals. Table No. 5 completely excludes from the diet:
- legumes;
- fatty cheese and full-fat milk, cream;
- hard-boiled and raw eggs;
- any refractory fats;
- sour berries, vegetables, herbs;
- freshly baked bread;
- baked goods;
- sweets;
- smoked meats;
- spicy;
- rich broths;
- alcohol;
- ice cream.
At the same time, vitamin therapy is carried out. The emphasis is on replenishing the lack of vitamins C, B, A and E.
Among the medications, the patient may be prescribed:
- products based on ademetionine, ursodeoxycholic acid;
- hepatoprotectors;
- glucocorticoids;
- choleretic;
- sorbents;
- protease inhibitors;
- diuretics;
- beta blockers.
In the presence of ascites, decongestants and albumin are used.
If cirrhosis was detected at the last stage, when drug correction is ineffective, the addict is offered to undergo surgical treatment. Its essence is a donor liver transplant.
Diagnostic methods
Diagnosis and therapy are carried out by a gastroenterologist or surgeon. The examination does not last long and the research is essentially simple:
- general and biochemical blood test;
- collection of urine and feces;
- ultrasound diagnostics of the peritoneum (shows changes in the structure of the liver and its size, the presence of fibrous tumors, whether the spleen is enlarged);
- CT and MRI – gives a complete understanding of the clinic;
- ERCP or endoscopic retrograde cholangiopancreatography – shows the liver from the inside;
- elastography - ultrasound examination that reveals the presence of pathological processes;
- biopsy – a piece of liver tissue is taken for examination.
What prognosis do doctors give for cirrhosis?
The prognosis is favorable for young people with normal body weight, especially for men, but provided that they completely abstain from alcohol and are actively treated under the constant supervision of a hepatologist.
The more the liver is damaged, the less chance a person has. Therefore, people over 45 years of age with a long alcohol history and who have other concomitant pathologies are more likely to die from cirrhosis.
Transition of alcoholic liver disease to cirrhosis
The transformation of alcoholic liver disease into cirrhosis is the terminal stage of the disease.
The incidence of liver cirrhosis increases with increasing alcohol dose to more than 30 ml/day and is maximum when drinking 120 ml/day or more. The transition of alcoholic liver disease to cirrhosis occurs in cases where the patient has not stopped drinking alcohol in any doses, has not completed a course of treatment for alcoholic liver disease, and does not adhere to strict recommendations for nutrition and vitamin therapy.
Literature:
- Kisly N. D. Alcoholic cirrhosis of the liver as a factor of destabilization of the basic functions of the body. Dissertation of Doctor of Medical Sciences: 14.00.05. Place of defense: Peoples' Friendship University of Russia (RUDN). - Moscow, 2004. - 33 p.
- Morozova T. G. Clinical, functional and social aspects of the modern course of alcoholic cirrhosis of the liver in combination therapy. Dissertation of a candidate of medical sciences: 14.00.05. Place of defense: Smolensk State Medical Academy. - Smolensk, 2008. - 18 p.
- Polikarpova T. S. Hepatorenal syndrome in alcoholic cirrhosis of the liver: the influence of polymorphism of genes and parameters of the renin-angiotensin-aldosterone system on the course and outcome, the effects of vasopressors and albumin. Dissertation of a candidate of medical sciences: 14.01.04. Place of defense: Peoples' Friendship University of Russia. - Moscow, 2010. - 16 p.
Therapy
Quitting drinking alcohol is the basis of treatment for alcoholic cirrhosis. It should be understood that ethanol not only has a destructive effect on the functioning of hepatocytes, but also reduces the effectiveness of medications. If you combine treatment with alcohol, this will lead to the premature death of the patient.
Conservative treatment of alcoholic cirrhosis of the liver is based on the use of drugs with detoxification, anti-inflammatory and diuretic effects. The attending physician draws up a treatment regimen based on the results of laboratory and instrumental examinations. As a rule, to prevent degenerative changes in the organs of the hepatobiliary system, the following is used:
adenomethionine preparations (“Heptordaily”, “Heptral”) - normalize the outflow of bile and accelerate the regeneration of hepatocytes;- hepatoprotectors (“Methionine”, “Hepatosan”) - protect parenchymal tissue from the destructive effects of toxins and ethanol;
- glucocorticosteroids (“Urbazon”, “Prednisolone”) - reduce the severity of inflammation, which promotes liver regeneration;
- tissue protease inhibitors (Sovaldi, Sofosbuvir) - prevent the formation of fibrous adhesions in the digestive gland;
- ursodeoxycholic acid preparations (Ursofalk, Ursohol) - stimulate bile secretion and prevent hepatocyte necrosis.
As a rule, alcoholic cirrhosis of the liver is complicated by pathologies that require surgical intervention. In particular, therapy for ascites involves laparocentesis, in which a puncture is made in the abdominal wall to pump out free exudate. To reduce hydrostatic pressure in hemorrhagic vessels, which occurs with portal hypertension, they resort to portosystemic shunting, i.e. creating an artificial path for the outflow of venous blood from the portal system.
The first signs of liver cirrhosis, classification
The main stages of disease development: compensation, subcompensation, decompensation.
Considering the causes of the disease, experts adhere to the following classification:
- viral (infectious) hepatitis;
- toxic (toxic-allergic);
- biliary;
- circulatory;
- metabolic and nutritional cirrhosis;
- cryptogenic.
Cirrhosis clinic. The severity of symptoms depends primarily on the cause of occurrence, the degree of organ damage and the speed of progression. Often the pathology occurs asymptomatically for a long period. The initial stage may be accompanied by discomfort in the liver area that occurs after eating, bloating, bitterness in the mouth and mild nausea. The first signs of liver cirrhosis are observed in half of the patients.
Specific symptoms:
- loss of appetite;
- yellowness of the skin;
- severe weakness, irritability;
- skin itching;
- bruises, hemorrhages;
- yellowness of the sclera.
Characteristic symptoms are “drumsticks”, redness of the palms, specific changes in the nails and telangiectasia.
You can find out more about the clinic of the disease on one of the pages of our website Dobrobut.com. At the center you can undergo a full examination and consult with a specialist. The doctor will answer your questions and tell you how long patients with the last stage of cirrhosis live. Recording 24 hours a day.
Liver cirrhosis. Issues of etiology, pathogenesis, clinical picture, diagnosis, treatment
Sadovnikova I.I.
Liver cirrhosis (LC) is a chronic polyetiological progressive disease that occurs with damage to the parenchymal and interstitial tissue of the organ with necrosis and degeneration of liver cells, nodular regeneration and diffuse proliferation of connective tissue, disruption of the architectonics of the organ and the development of varying degrees of liver failure.
In economically developed countries, cirrhosis of the liver is one of the six leading causes of death at the age of 35-60 years and ranges from 14 to 30 cases per 100,000 population. In the world, 40 million people die annually from viral cirrhosis of the liver and hepatocellular carcinoma, which develops against the background of carriage of the hepatitis B virus. In the CIS countries, CP occurs in 1% of the population.
Etiology and pathogenesis
The most common causes of liver cirrhosis are chronic alcohol intoxication (according to various sources, from 40-50% to 70-80%) and viral hepatitis B, C and D (30-40%). The most important stages in the development of alcoholic cirrhosis of the liver are acute alcoholic hepatitis and fatty liver degeneration with fibrosis and mesenchymal reaction. Alcohol-viral cirrhosis with rapidly progressive dynamics of the disease is characterized by a particularly severe course. They most often transform into hepatocellular carcinoma. Much less often, diseases of the biliary tract (intra- and extrahepatic), congestive heart failure, and various chemical and drug intoxications play a role in the development of liver cirrhosis. Rare forms of liver cirrhosis are associated with genetic factors leading to metabolic disorders (hemochromatosis, hepatolenticular degeneration, α1-trypsin deficiency) and occlusive processes in the portal vein system (phleboportal cirrhosis). The cause of primary biliary cirrhosis remains unclear. In approximately 10-35% of patients, the etiology of cirrhosis cannot be determined. Such observations are attributed to cryptogenic cirrhosis, the causes of which are still unknown.
The formation of liver cirrhosis occurs over many months or years. During this time, the gene apparatus of hepatocytes changes and generations of pathologically altered cells are created. This process in the liver can be characterized as immunoinflammatory. The most important factor in the genesis of alcoholic cirrhosis of the liver is damage (necrosis) of hepatocytes, caused by the direct toxic effect of alcohol, as well as autoimmune processes. Sensitization of immunocytes to the body's own tissues is an important factor in pathogenesis in cirrhosis that develops in patients with viral hepatitis B, C and D. The main target of the autoimmune reaction here appears to be hepatic lipoprotein. The dominant factor in the pathogenesis of congestive liver cirrhosis is hepatocyte necrosis associated with hypoxia and venous stagnation.
The further stage of development of the pathological process: portal hypertension - increased pressure in the portal vein system, caused by obstruction of intra- or extrahepatic portal vessels. Portal hypertension, in turn, leads to the appearance of portocaval shunting of blood, splenomegaly and ascites. Thrombocytopenia (increased deposition of blood platelets in the spleen), leukopenia, and anemia (increased hemolysis of red blood cells) are associated with splenomegaly.
Ascites leads to limited mobility of the diaphragm (risk of pulmonary atelectasis, pneumonia), gastroesophageal reflux with peptic erosions, ulcers and bleeding from esophageal varices, abdominal hernias, bacterial peritonitis, hepatorenal syndrome.
Hepatogenic encephalopathies are often observed in patients with liver cirrhosis.
The leading place in the origin of primary biliary cirrhosis belongs to genetic disorders of immunoregulation. Initial changes include destruction of the biliary epithelium followed by necrosis of tubular segments and, in a later stage of the disease, their proliferation, which is accompanied by impaired bile excretion; the epithelium is infiltrated with lymphocytes, plasma cells, and macrophages. In the evolution of the disease, 4 stages can be traced: chronic non-purulent destructive cholangitis, ductular proliferation with destruction of bile canaliculi, scarring with a decrease in bile canaliculi and the development of large-nodular cirrhosis and cholestasis.
Classification
The World Association of Hepatologists (Acapulco, 1974) and WHO (1978) recommended a simple morphological classification of liver cirrhosis, based on a minimum of criteria, according to which they distinguish:
- small-nodular, or small-nodular (diameter of nodes from 1 to 3 mm);
- large-nodular, or macronodular (diameter of nodes more than 3 mm);
- incomplete septal;
- mixed (in which different sizes of nodes are observed) form.
In accordance with the latest classification (Los Angeles, 1994), cirrhosis is distinguished by etiology, degree of activity determined by biochemical tests (ALT activity), and morphological changes in the liver.
Depending on the etiology, liver cirrhosis is distinguished: viral, alcoholic, drug-induced, secondary biliary, congenital (hepatolenticular degeneration, hemochromatosis, a1-trypsin deficiency, tyrosinosis, galactosemia, glycogenosis), congestive (circulatory failure), disease and Budd-Chiari syndrome, metabolic - nutritional (small intestinal bypass, obesity, severe forms of diabetes mellitus) and liver cirrhosis of unknown etiology (cryptogenic, primary biliary, Indian childhood).
It is considered advisable to divide liver cirrhosis depending on the severity of hepatocellular failure (compensated, subcompensated, decompensated), the degree of portal hypertension and the activity of the process. Depending on the activity of the process, which means the severity of inflammatory reactions, all cirrhosis is divided into active and inactive.
Hepatocellular function in liver cirrhosis is assessed by Child-Pugh.
Compensated cirrhosis is indicated by the indicators of group A, the indicators of group B and C correspond to decompensated cirrhosis (technique of using criteria: one indicator of group A is estimated at 1 point, the same indicator of group B is estimated at two points, and in group C - at 3 points). The proposed system is suitable for assessing the prognosis, especially outside of a sharp exacerbation of cirrhosis and its complications. In recent years, to determine the prognosis of patients with cirrhosis at the time of the development of complications such as gastrointestinal bleeding, coma, sepsis, etc., the SAPS (Simplifed Acute Physiology Score) criteria system has been used, which includes basic physiological parameters, most of which are not directly related with liver condition. These include: age, heart and respiratory rate, systolic blood pressure, body temperature, diuresis, hematocrit, white blood cell count, serum concentrations of urea, potassium, sodium, and bicarbonates, stage of hepatic coma
Clinical picture
Liver cirrhosis is more often observed in men: the ratio of male to female patients is on average 3:1. The disease occurs in all age groups, but more often after 40 years.
The difficulty of early diagnosis of liver cirrhosis is largely due to the diversity of its first clinical manifestations. The most common clinical manifestations include general symptoms such as weakness, decreased ability to work, abdominal discomfort, dyspepsia, fever, and joint pain. Flatulence, pain and a feeling of heaviness in the upper abdomen, weight loss, and asthenia are often observed. Upon examination, an enlarged liver is revealed with compaction and deformation of its surface, the edge of the liver is sharpened. In the initial stage, there is a uniform moderate increase in both lobes of the liver; subsequently, the increase in the left lobe often predominates. Portal hypertension is manifested by moderate splenomegaly.
The period of the developed clinical picture is diverse in its symptoms and reflects the involvement of almost all body systems in the pathological process. The main, characteristic symptoms are associated with the presence of hepatic cellular failure and portal hypertension. The most common complaints are weakness, fatigue, decreased performance (bloating, poor tolerance of fatty foods and alcohol, nausea, vomiting, diarrhea), sleep disturbance, irritability. Especially often there is a feeling of heaviness or pain in the abdomen (mainly in the right hypochondrium), impotence, itchy skin, and menstrual irregularities in women. The most common objective symptom is hepatomegaly (70%). The liver has a compacted consistency, a pointed edge, and little or no pain. In 30% of patients, the nodal surface of the organ is palpable. In the terminal stage of the disease, in 25% of cases there is a decrease in liver size, splenomegaly in 50% of patients.
External symptoms of cirrhosis are often found: palmar or plantar erythema, spider veins, scanty hair in the axillary and pubic area, white nails, gynecomastia in men. These changes are explained by the appearance of signs of hyperestrogenemia against the background of hepatic cell failure. Weight loss is characteristic, often masked by the simultaneous accumulation of fluid. Half of the patients have elevated body temperature. In most cases, the fever is low-grade and persists for several weeks. The temperature associated with necrosis of hepatocytes is often accompanied by intense jaundice, increased activity of aminotransferases and serum alkaline phosphatase, and leukocytosis. The increase in temperature is associated with the passage of intestinal bacterial pyrogens through the liver, which it is not able to neutralize. Fever is not treatable with antibiotics and only goes away when liver function improves. Relatively late symptoms of cirrhosis, characterizing severe hepatocellular failure and portal hypertension, include jaundice, ascites, peripheral edema (primarily swelling of the legs), and external venous collaterals. Hepatolienal syndrome is often accompanied by hypersplenism, characterized by a decrease in blood formed elements (leukopenia, thrombocytopenia, anemia) and an increase in cellular elements in the bone marrow.
One of the most common signs of liver cirrhosis is varicose veins of the esophagus, stomach, intestines, including the duodenum, bleeding from which, due to the frequency of deaths, is the most serious complication of liver cirrhosis. Other venous collaterals, including mesenteric vessels, detected only by angiography or surgery, can become a source of severe bleeding with a fatal outcome. Bleeding is also possible from hemorrhoidal veins, but they are observed less frequently and are less intense.
Encephalopathies occur both against the background of hepatocellular and portal-hepatic failure.
Etiological variants of liver cirrhosis
Viral cirrhosis of the liver is in most cases macronodular. There are two types of viral cirrhosis: early, developing during the first year after acute hepatitis (usually hepatitis D, which occurs with jaundice and severe cytolysis or cholestasis syndrome), and late, developing after a long latent period (5-15 years).
The clinical picture resembles the acute phase of viral hepatitis: jaundice, fever with chills, asthenovegetative and dyspeptic syndromes. Jaundice is moderate but persistent; hyperbilirubinemia persists despite therapy. The form of cirrhosis with cholestasis is accompanied by intense jaundice, persistent itching, and high levels of alkaline phosphatase. Peripheral abdominal collaterals do not have time to develop, telangiectasias are absent. Hepatomegaly is combined with splenomegaly. A marker of D infection is the detection of anti-delta antibodies of the IgM and IgG classes. The late (more common) form of viral cirrhosis occurs gradually, slowly as a result of chronic viral hepatitis B and C. Patients develop anorexia, heaviness in the right hypochondrium, flatulence, muscle and joint pain, nosebleeds, body weight deficiency, muscle wasting, dryness skin. Hepatomegaly, splenomegaly with hypersplenism, icterus of the skin, sclera, spider veins and palmar erythema, portal hypertension and encephalopathy develop. Functional liver failure appears early and coincides with periods of exacerbation of the disease. In the stage of established cirrhosis, dilated veins of the esophagus and hemorrhages are observed. Ascites occurs in the later stages of the disease.
Alcoholic cirrhosis of the liver develops in approximately 10% of alcohol abusers within a period of 5 to 20 years. Men get sick more often.
In the advanced stage, dyspeptic complaints predominate - loss of appetite, vomiting, diarrhea. Dyspeptic syndrome is caused by concomitant gastritis and alcoholic pancreatitis. Signs of dystrophy and vitamin deficiency are revealed much earlier than with viral cirrhosis. Systemic effects of chronic alcohol intoxication lead to polyneuritis, myopathy, muscle atrophy, Dipuytren's contracture, enlarged parotid glands, hair loss and testicular atrophy. In addition, alcoholism causes damage to the kidneys, heart, and moderate arterial hypertension.
Secondary biliary cirrhosis of the liver develops as a result of long-term disruption of the outflow of bile at the level of large intra- and extrahepatic bile ducts: with obstruction of the bile ducts by a stone, postoperative scar, benign tumors, it is also observed with primary sclerosing cholangitis, common bile duct cysts, lymphogranulomatosis. The main pathogenetic links: initial cholestasis, perilobular fibrosis, cirrhosis. Due to mechanical obstruction of the biliary tract, biliary hypertension occurs and the flow of bile components into the periductal spaces is noted. Elimination of cholestasis promotes the reverse development of the process. Biliary cirrhosis is characterized by pain, fever, chills, leukocytosis, hepatomegaly, splenomegaly, cholestasis syndrome - skin itching, severe jaundice, hyperbilirubinemia, increased levels of cholesterol, bile phosphatase, bile acids.
Primary biliary cirrhosis of the liver. The etiology is unknown in most cases.
The prevalence is 23-50 people per 1 million adult population, among all liver cirrhosis it is 6-12%. Mostly women during menopause are affected.
This gradually beginning progressive liver disease is characterized by granulomatous non-purulent destructive cholangitis with the development of fibrosis and cirrhosis. The first sign of the disease is itching, which is caused by an increased level of bile acids in the blood. Jaundice appears several years after the onset of itching. Skin pigmentation, xanthomas, xanthelasmas, and scratching are typical. The liver is moderately enlarged, splenomegaly is detected in later stages of the disease. With prolonged jaundice, systemic osteoporosis is detected: changes in the bones of the pelvis, skull, spine, ribs. Signs of portal hypertension (varicose veins of the esophagus, etc.) appear later than in common forms of liver cirrhosis. Of the biochemical tests, high levels of IgM and alkaline phosphatase in the blood serum, hypercholesterolemia, and hypertriglyceridemia have the greatest diagnostic value. In 90% of cases, antibodies to mitochondria are observed.
Complications of liver cirrhosis
The most severe complications of liver cirrhosis: hepatic coma, bleeding from varicose veins of the esophagus (less often the stomach, intestines), thrombosis in the portal vein system, hepatorenal syndrome, and the formation of liver cancer. Often, especially with alcoholic cirrhosis, infectious complications are observed - pneumonia, “spontaneous” peritonitis with ascites (it is assumed that opportunistic intestinal bacterial flora plays an important role in its development - under the influence of swelling of the intestinal loops as a result of lymphostasis and immunity disorders, the intestinal flora penetrates into the free abdominal cavity and acquires clear pathogenic properties), sepsis.
Diagnosis of liver cirrhosis
Anamnestic data - alcohol abuse, previous viral hepatitis B, C or D. Typical complaints of nosebleeds, dyspeptic disorders, weakness, abdominal pain, etc. allow one to suspect the formation of cirrhosis of the liver in the patient.
During an objective examination, the following indicators attract attention: telangiectasia in the area of the shoulder girdle and face, erythema of the palmar and digital eminences, blanching of the nails, phenomena of hemorrhagic diathesis, loss of nutrition and atrophy of skeletal muscles, grayish-pale skin tone or moderate icterus of the sclera, thickened liver with a sharp lower edge, splenomegaly, endocrine disorders.
Data from laboratory and instrumental research methods include: blood tests, leukothrombocytopenia, anemia, characteristic biochemical changes: hyper-g-globulinemia, hypoalbuminemia, increased activity of aminotransferases, hyperbilirubinemia due to the conjugated fraction of pigment, etc., decreased prothrombin index, other indicators of coagulation blood systems. Immunological methods for studying blood serum are used to confirm one or another etiological form of liver cirrhosis. The concentrations of immunoglobulins in active cirrhosis are usually increased; alcoholic cirrhosis is characterized by an increase in the level of IgA; for viral cirrhosis, it is predominantly IgG and IgM. A particularly significant increase in IgM concentration is observed in patients with primary biliary cirrhosis. In the same case, antibodies to mitochondria are detected in the blood serum. Among antimitochondrial antibodies, a number of fractions have been isolated, such as M-2 and M-9, the latter has a special role in the early diagnosis of primary biliary cirrhosis.
The significance of instrumental research methods for this disease varies.
Ultrasound of the liver allows you to determine the size of organs - the liver and spleen, the density of their parenchyma, visualize the presence of nodes and the spread of the process, and identify signs of portal hypertension.
Computed tomography is a more informative method, especially in patients with ascites and severe flatulence; allows you to obtain information about the density and homogeneity of the liver tissue; Even small amounts of ascitic fluid are well captured.
Radionuclide scanning. Research is carried out with colloidal preparations 197Au and 99mTc. In liver cirrhosis, a diffuse decrease in the absorption of the isotope in the liver is observed. The method is not very informative.
Angiographic examination - celiacography and splenoportography. Used to visualize blood vessels and determine the presence and extent of portal hypertension.
A puncture biopsy of the liver is the most informative procedure, since it allows for a histological examination of the biopsy material, determining the type of pathological process and its stage.
Laparoscopic examination of the abdominal cavity, despite its traumatic nature in these patients, allows us to obtain additional information about the condition of the abdominal organs and blood vessels.
Treatment
Treatment and preventive measures for patients with cirrhosis begin with secondary prevention:
- prevention of infection with acute viral hepatitis, which, according to statistics, leads to the death of 50-60% of patients during the first year from the moment of its development;
- categorical refusal of alcohol, which can significantly improve the prognosis and life expectancy of patients;
- protection against hepatotoxic drugs.
There is currently no etiotropic therapy for most forms of cirrhosis.
A complete, balanced diet of 5-6 meals a day is prescribed for better outflow of bile and regular bowel movements (diet within table No. 5). In case of encephalopathy, protein intake is reduced to a level at which symptoms of ammonia intoxication do not appear. Table salt is limited; for ascites, a salt-free diet is prescribed, supplementing the diet with foods rich in potassium. For itching and bradycardia, reduce the volume of meat proteins, legumes containing tryptophan, tyrosine, cystine and methionine, which are sources of toxic metabolites and ammonia.
Patients in the inactive compensated stage of liver cirrhosis do not need drug therapy. They are periodically prescribed a complex of vitamins for oral administration.
For moderately active liver cirrhosis, medications that include vitamins (vitamins B6 and B12, co-carboxylase, rutin, riboflavin, ascorbic acid, folic acid), lipoic acid, milk thistle extract are recommended to improve liver cell metabolism. Courses of therapy are designed for 1-2 months. Herbal medicines are becoming increasingly important among this group of drugs. A purified dry extract obtained from the fruits of milk thistle, containing flavolignans and flavonoids, the drug Silimar has a pronounced hepatoprotective effect: it suppresses the growth of indicator enzymes, stabilizing the cell membrane of hepatocytes, inhibits the processes of cytolysis, and prevents the development of cholestasis. It exhibits antioxidant and radioprotective properties, enhances the detoxification and exocrine function of the liver, and has an antispasmodic and slight anti-inflammatory effect. Improvement in clinical manifestations in the form of a decrease in subjective complaints from patients and a decrease in biochemical indicators of the activity of the process in the liver have been reliably proven. According to the experiment, the following indicators were obtained: on the 7th day, the inhibition of the increase in activity for AST and ALT was 54.8%, on the 14th day - 66% of the initial background of ALT and a slightly smaller slowdown for AST, distinct (by 33-60%) dose-dependent decrease in GGT activity in blood serum. These changes were recorded in both acute and chronic experiments. The choleretic function of the drug was clearly visible at a minimum dosage of 50 mg per kg of body weight for 1 and 2 hours of the study and revealed its increase by 31.6% and 26.3%, respectively. Indicators of cholestasis syndrome such as cholesterol, triglycerides, alkaline phosphatase completely returned to normal, and bilirubin and g-glutamine transpeptidase decreased to figures exceeding the norm by 1.4 and 2.1 times, and initially they exceeded the norm by 3.1 and 5 ,4 times. In addition, clinical trials showed a clear normalization of gallbladder function in patients with manifestations of hypomotor dyskinesia. It is these points that make it possible to use Silymar in patients with liver damage due to cholestasis syndrome, in contrast to its analogues. The drug is used at any age in a course from 25 days to 1.5 months, 1-2 tablets 3 times a day 30 minutes before meals.
In the decompensated stage of liver cirrhosis with encephalopathy, ascites or severe hemorrhagic syndrome, the dose of lipoic acid or lipamide is increased to 2-3 g per day, the course of treatment is 60-90 days. Oral administration is combined with parenteral administration of drugs for 10-20 days. The course of treatment for Essentiale is carried out similarly: 2-3 capsules orally 3 times a day and 10-20 ml intravenously 2-3 times a day in an isotonic solution. The course of combined treatment is from 3 weeks to 2 months. As the symptoms of hepatic cell failure disappear, they move on to taking capsules orally. The total duration of treatment is up to 6 months.
For viral liver cirrhosis of moderate activity with the presence of serum markers HBV, HCV, the use of prednisolone in a daily dose of 30 mg per day is indicated. Severe cytopenia is also an indication for use. The dose is gradually reduced by 2.5 mg every 2 weeks. Maintenance dose - 15-7.5 mg is selected individually and taken for 2-3 years. A high degree of activity and a rapidly progressive course require high doses of the drug - from 40 to 60 mg. The use of corticosteroids in the decompensated stage of the disease is not indicated, since they contribute to the occurrence of infectious complications and sepsis, ulcerations of the gastrointestinal tract, osteoporosis, catabolic reactions leading to renal failure and hepatic encephalopathy.
Treatment of patients with ascites is carried out by combining diuretics: aldosterone antagonists and thiazide drugs. Combinations of spironolactone - ethacrynic acid, spironolactone - triampur, spironolactone - furosemide are effective. Daily diuresis should not exceed 2.5-3 liters to avoid a noticeable imbalance of electrolytes. With the advent of powerful diuretics, paracentesis was practically stopped due to the resulting loss of protein and the risk of infection.
There is no effective treatment for primary biliary cirrhosis. Corticosteroids do not have a significant effect on the course of the disease, but slow down its progression. D-penicillamine suppresses the inflammatory reaction of connective tissue, the development of fibrosis, reduces the content of immunoglobulins and the level of copper in hepatocytes. A noticeable effect is observed only with long-term use (1.5-2 years). Ursodeoxycholic acid at a dose of 10-15 mg per kg of body weight for a period of 6 months to 2 years leads to an improvement in biochemical blood parameters with the disappearance of skin itching, weakness, and anorexia. Plasmapheresis brings temporary relief. Liver transplantation is performed.
Indications for surgical treatment of cirrhosis are: severe portal hypertension with esophageal varices in those who have suffered bleeding, with esophageal varices without bleeding; if a sharply dilated coronary vein of the stomach is detected in combination with high portal hypertension; hypersplenism with a history of esophageal bleeding or its threat. Various types of portacaval anastomoses are used: mesentericocaval, splenorenal in combination with or without splenectomy. Contraindications to surgical intervention are progressive jaundice and age over 55 years.
Forecast
Life expectancy of more than 5 years from the moment of diagnosis is observed in 60% of patients with alcoholic cirrhosis, in patients with viral cirrhosis - in 30%. With primary biliary cirrhosis, life expectancy is 5-15 years. The degree of compensation of the disease has a very noticeable effect on the prognosis. Approximately half of patients with compensated cirrhosis live more than 7 years. With the development of ascites, only a quarter of patients survive 3 years. Encephalopathy has an even more unfavorable prognostic value, in which patients in most cases die within the next year. The main causes of death are hepatic coma (40-60%) and bleeding from the upper gastrointestinal tract (20-40%), other causes are liver cancer, intercurrent infections, hepatorenal syndrome.
Literature 1. Bronovets I.N., Goncharik I.I., Demidchik E.P., Sakovich M.N. Handbook of gastoenterology. - Minsk, 1997. 2. Burchinsky G.I. Clinical gastroenterology. - Kyiv, 1979. 3. Gastroenterology 2002.3. 4. Ivashkin V.T., Komarov F.I., Rapoport S.I. A short guide to gastroenterology. - Moscow, 2001. 5. Komarov F.I. Diagnosis and treatment of internal diseases. Volume 3. - Moscow, 1992. 6. Komarov F.I., Grebenev A.L. Guide to gastroenterology. Volume 2. - Moscow, 1995 7. Clinical perspectives of gastroenterology and hepatology 2003.1. 8. Martynov A.I., Mukhin N.A., Moiseev V.S. Internal illnesses. Textbook for universities. Volume 2. - Moscow, 2001. 9. Podymova S.D. Liver diseases. - Moscow, 1984. 10. Rasmussen HH, Fallingborg JF, Mortensen PB et al. Hepatobiliary dysfunction and primary sclerosing cholangitis in patients with Crohn's disease // Scand. J. Gastroenterol/ - 1997. - Vol. 32(6). - P. 604-610 11. Sherlock Sh., Pooley Y. Diseases of the River and billary system Blackwell Science. — 10th edition. — 714 p. 12. The Merck Manual of diagnosis and therapy / Ed. M. H. Beers, R. Berkow, 1999, [Merch Research Laboratories, Division of Merck A. Co inc. 17th edition. - P. 2833.
Dietary recommendations for liver cirrhosis
For cirrhosis, prepare meals without salt, reduce the amount of free liquid and introduce foods rich in potassium.
Nutritional balance
The main parts of food are proteins, fats, carbohydrates, water, minerals and vitamins, which must be strictly balanced. The ratio between proteins, fats and carbohydrates should be 1:1:4. Animal proteins should make up about 60% of the total protein. Of the total fat, 20-25% should be vegetable oils as a source of polyunsaturated fatty acids. The balance of carbohydrates is expressed in the ratio of starch, sugar, fiber and pectin. Sugars should be represented by fruits, berries, dairy products, and honey. It is extremely important to maintain a balance of vitamins and minerals, which must be supplied to the body daily in accordance with daily requirements.
Diet
This is the number of meals and the interval between them during the day. For healthy people 3-4 times a day at 4-5 hour intervals. For some diseases, such as obesity, it is necessary to eat 5-6 times a day
up
Forms of the disease
Without treatment, cirrhosis passes from one form to another:
- compensated: the damage has already begun, but the organ is functioning normally;
- subcompensated: some functions are impaired, health worsens;
- decompensated: some functions are not performed, severe symptoms appear.
The compensated form of cirrhosis is best treated: liver function can be restored by stopping drinking alcohol.
In the decompensated form, the changes are irreversible. You have questions?
We will call you back within 30 seconds
or call the number
Clicking the "Submit"
, you automatically consent to the processing of your personal data and accept the terms of the User Agreement.