A colostomy is an artificially created fistula tract that connects the large intestine to the external environment. The name is formed by combining two words: colon - colon and stoma - opening.
Often, with various intestinal diseases, it is impossible to drain feces naturally and then specialists use a colostomy. What is this operation and what lifestyle should you lead after it? What negative consequences could such an intervention entail? Who needs a colostomy? Answers to these and other questions can be found by reading the following article.
What is a colostomy
The colon is one of the parts of the large intestine where feces are formed. Its functions also include their promotion and subsequent removal to the outside through the anus. The colon has the following structure: cecum, ascending colon, transverse colon, descending colon and sigmoid colon.
Content:
- What is a colostomy
- Types of colostomy
- Indications for colostomy
- Preparation for the operation
- Performing a colostomy. Main types of surgery
- Complications after colostomy
- Stoma care at home
- Types of colostomy bags
- Advantages and disadvantages of colostomy
- Rehabilitation postoperative period
- conclusions
Liquid digested food passes from the small intestine to the large intestine. After passing through the entire colon, the stool hardens. Therefore, in the ascending colon they are still contained in liquid form and have a slightly alkaline environment. Further along the sigmoid colon, the digested food enters the rectum, where, with the help of the sphincter apparatus, feces are retained in the ampullary section. When they accumulate, a person has the urge to defecate, which usually happens once a day.
With various interventions in this process, a colostomy is often made - a kind of hole in the abdominal wall into which the end of the colon is sewn. Thus, the waste products of the body, passing through the intestines, reach such an opening and go straight into a special bag attached to the colostomy. The operation in which this occurs is called a colostomy.
Most often, such an operation is indicated if the patient needs to bypass some part of the rectum due to injuries, inflammation, various types of tumors, as well as during the postoperative recovery period.
After such an operation, feces in patients are removed through an artificially created opening of the anus, without disturbing the functioning of the entire intestinal tract.
How a stoma is formed
The specific location of the colostomy is determined by the surgeon, taking into account the clinical situation and anatomical characteristics of the patient. In addition, the condition of the outer integument and the abdominal wall must be taken into account - scars and cicatrices significantly complicate the installation of a colostomy bag.
An ileostomy is most often located in the right iliac region; a section of the ileum is exposed to the anterior abdominal wall.
Colostomies:
- Ascendostomy , cecostoma is located in the right iliac region or right mesogastrium, formed from the ascending, cecum. Intestinal secretions are similar in composition to small intestinal contents.
- The transversostomy can be located in the right or left hypochondrium, as well as along the midline of the abdomen above the navel, at the level of the navel to the left or right of it. This type of stoma is formed from the transverse colon. Most patients experience a discharge of mushy contents, which easily irritate the skin around the stoma.
- The sigmostoma is located in the left iliac region, the sigmoid colon is removed. Through the sigmostoma, feces are released, as a rule, once or twice a day, and the consistency is semi-formed.
Types of colostomy
There are several types of colostomies, depending on the location, shape and time of application.
Ostomies can be temporary or permanent. If the lower intestine cannot be repaired, a permanent stoma is used. In other cases, a temporary colostomy is indicated.
The shape of the stoma is:
- Single-barrel or terminal, in which a longitudinal incision is made in the colon and only one hole comes out, most often used for ectomy of the descending colon and are almost always permanent.
- Double-barreled or loop ones, in which a transverse incision is made in the colon and two holes are brought out, through one of which feces are removed, and through the other various medications are administered, most often these are temporary stomas.
According to localization, artificial holes are divided into:
- Rising. Another name is ascendostomy. It is usually located on a segment of the ascending colon on the right side of the abdominal cavity. In this area, the feces are not yet fully formed, and therefore their contents will be liquid and alkaline, containing residual fragments of undigested food. In such cases, frequent cleaning of the colostomy bag is required and drinking plenty of fluids is recommended to avoid dehydration. Such a bone break is usually temporary.
- Transverse. Another name is transversostomy. This hole is located in the transverse colon in the upper region of the abdominal cavity. Most often, it is moved closer to the left bend of the spleen so as not to affect the nerve endings. These colostomies are usually temporary. A permanent stoma is placed only if amputation of the part of the intestine located below this section is necessary.
- Descending. Otherwise known as a descendostoma.
- Sigmostoma.
The last two types of stomas are located in the lower part of the abdominal cavity on the left, almost at the very end of the colon. They differ from other types of colostomies in that with such artificially recreated holes the patient is able to independently control the processes of defecation. This is due to the fact that in this part of the intestine there are nerve endings, thanks to which such control is possible. Such colostomies can be either temporary or permanent.
Small bowel stomas
The contents of the small intestine are liquid and alkaline, therefore the same chemical composition and consistency is discharged through the small intestinal stoma. The alkaline reaction of the discharge from this type of stoma is the reason why severe skin irritation occurs when the contents of the stoma get on it. Prolonged contact of chyme with the skin leads to the formation of non-healing erosions and ulcers on the skin.
When comparing the volume of discharge per day, the daily volume of liquid chyme from small intestinal stomas significantly exceeds the volume of discharge from colostomy. Due to electrolyte losses through stomas formed on a loop of the small intestine, a significant amount of fluid with a high content of potassium and sodium (the so-called blood electrolytes) - most people with a small intestinal stoma are susceptible to dehydration (dehydration) and disturbances in the electrolyte balance of the blood. The formation of kidney and gallstones is also possible: when dehydrated, the kidneys reabsorb water from primary urine, thereby producing more concentrated urine. Mineral sediment may “fall out” from such concentrated urine and stones may form in the kidneys and other parts of the urinary tract.
Indications for colostomy
Such an operation is performed in extreme cases and for health reasons, as it is an unnatural intervention in the vital functions of the body.
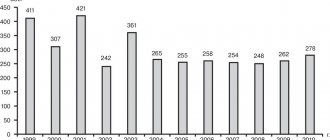
Currently, almost twenty-five percent of all operations on the large intestine result in a colostomy.
Indications for colostomy are:
- intestinal injuries;
- rectal fecal incontinence;
- congenital anomalies of the intestinal outlet;
- inoperable tumors;
- radical removal of oncological tumors of the rectum, as well as post-radiation proctosigmoiditis;
- intestinal obstruction;
- the presence of enterovaginal fistulas or enterovesical type fistulas;
- failure of the earliest anastomosis;
- wounds and injuries of the perineum;
- ulcerative colitis and diverticulitis, complicated by bleeding or intestinal perforation.
Why is a colostomy formed?
A stoma may be required if:
- Diverticulitis is an inflammation of diverticula, which are pouch-like protrusions of the intestinal wall. The disease leads to the development of abscesses - the formation of pus-filled cavities, scars, narrowing or rupture of parts of the digestive tract.
- Cancer.
- Multiple polyps - tissue growth on the inner surface of the digestive tract, which can lead to the development of oncology.
- Partial or complete intestinal obstruction.
- Injuries and damage.
- Congenital developmental defects - for example, the absence of an anus.
- Inflammatory bowel diseases, leading to damage to the internal mucous membrane.
Preparation for the operation
Almost always, a colostomy is the final stage of some other operation.
Therefore, it requires the same preparation as any other intestinal surgery, namely:
- initial examination by the attending physician;
- cleansing enema;
- fluorography;
- complete blood count and urinalysis;
- electrocardiogram;
- coagulogram;
- blood biochemistry test;
- tests for infectious markers;
- irrigoscopy and colonoscopy.
In particularly severe cases, preoperative blood or plasma transfusions and replenishment of water and electrolyte balance may be required.
Very often, a colostomy is performed as an emergency, for example, in case of acute intestinal obstruction. Then only minimal preparation is necessary to eliminate the obstruction as soon as possible. If the patient’s condition is serious, doctors postpone the main operation to eliminate intestinal obstruction until the patient’s condition improves, but a colostomy is performed urgently, placing a colostomy slightly above the blockage.
Ostomy
Ostomy is a surgical procedure, the end result of which is a stoma. Ostomy is performed when it is impossible to move biological fluids and air due to the disease blocking natural anatomical pathways.
In most cases, ostomy is performed for emergency reasons, when a person’s life is in danger due to the cessation of air movement or biological substrates.
Planned stoma has advantages over emergency surgery in all aspects - clinical and psychological, because it allows you to prepare the patient’s body and consciousness for a significant change in life activity.
Performing a colostomy. Main types of surgery
A patient with different conditions may require different types of colostomy. This may be the application or closure of a colostomy, as well as surgery for reconstructive purposes.
A colostomy is performed under general anesthesia in a sterile operating room. The procedure proceeds according to the following scenario:
- A small area of skin and subcutaneous tissue is cut off at the site where the stoma is planned to be located.
- Muscles are distributed according to the direction of the fibers. To avoid excessive pressure on the intestine, the hole is made large enough. If a colostomy is placed for a long period of time, it is necessary to take into account the fact that the patient may gain excess weight.
- The intestine is brought out through a loop and the necessary incision is made on it.
- The removed intestine is sewn to the abdominal muscles, and the edges are attached to the skin.
At the moment, there are no drainage systems or means that can take root in the stoma orifice, since the body’s immune system rejects all possible options, causing inflammation and tissue degeneration with any foreign intervention.
Therefore, sewing the edge of the intestine to the skin is still used, which subsequently heals quite quickly and well.
Closing a stoma is also called a colostomy. It is essentially the elimination of a fistula of artificial origin and is carried out approximately two to six months after the colostomy.
A prerequisite for such an intervention is the complete absence of obstructions in the intestines up to the anus.
Having retreated some distance from the edge of the colostomy, tissue is excised, after which a piece of intestine is removed and the edge in which the hole was formed is cut off. The ends of the intestine are then sutured and returned to the abdominal cavity. After this, the seam is checked for leaks and the resulting wound is sutured.
Reconstructive intervention is usually used for temporary colostomies, which are applied while the lower intestine is being treated.
Even with a successful operation to close a colostomy, the absence of some part of the intestine significantly complicates the patient’s life.
It is best to close a colostomy three to twelve months after surgery. In essence, reconstructive surgery is a colostomy.
What complications can there be if you have an intestinal stoma?
Peristomal dermatitis (skin irritation in the stoma area)
Dermatitis is observed quite often and is a consequence of mechanical irritation (frequent changes of colostomy bags, careless treatment of the skin), or chemical exposure to intestinal discharge (leakage under the plate, poorly selected, leaky colostomy bag).
Manifestations of dermatitis: redness, blisters, cracks, weeping ulcers on the skin around the stoma. Skin irritation causes itching, burning, and sometimes severe pain. It is possible to develop an allergic skin reaction to stoma care devices and products. If the allergy is severe, you should stop using adhesive bags for a while. In such cases, the question of choosing the type of colostomy bag should be decided by the doctor. Often the cause of skin complications is simply insufficient skin care in the stoma fixation area. In case of skin irritation around the stoma, consultation with a coloproctologist or specialist in the rehabilitation of ostomy patients is necessary.
Hypergranulation in the stoma area
With frequent dermatitis around the stoma, polypoid growths form at the border between the skin and the mucous membrane, which bleed easily. Typically these formations are small, a few millimeters in diameter. If such skin changes occur, consult a doctor.
Eventration of the small intestine
Eventration of the small intestine - prolapse of loops of the small intestine into the parastomy wound - occurs if the incision was made too wide to form the stoma. This complication most often occurs in restless children who cry a lot in the coming days after surgery, which causes an increase in intra-abdominal pressure and, as a consequence, the formation of eventration. In adult patients, a prolonged increase in intra-abdominal pressure (persistent cough, repeated vomiting) and violation of the therapeutic and protective regime (heavy lifting) also leads to eventration. Prolapse of small intestinal loops requires emergency surgery.
Evagination
Evagination is the turning of the intestine outward. Occurs more often in children. A certain role in the occurrence of this complication can be played by constantly increased intra-abdominal pressure, increased peristaltic activity of the adductor intestine, and an excessively loose aponeurosis defect. Evagination can be minor and can be eliminated with light pressure, but sometimes it is massive, for example, cecostomy is often complicated by evagination of the ileocecal angle. In most cases, surgery is not required, but the patient must continually have the prolapsed bowel adjusted.
Stoma stricture
Stoma stricture is a narrowing of the stoma outlet. It develops most often when tissues (skin) are prone to forming keloid scars. Less commonly, stenosis can be caused by suturing the anterior abdominal wall around the stoma. With this complication, emptying is delayed, and in rare cases, intestinal obstruction may develop. With the gradual formation of a narrowing (stricture) of the stoma outlet, the patient’s struggle with this complication comes down to changing the diet and the formation of soft feces, which greatly facilitates their passage through the narrowed opening. In the future, it is possible to expand the narrowing using the bougienage method, by introducing medical supplies (rubber probe, catheter) into the narrowed hole. It is not always possible to eliminate the stricture conservatively (bougienage), then they resort to surgery. During the operation, according to indications, the stoma is eliminated or its reconstruction is performed.
Bloody discharge from the stoma
In most cases, the appearance of blood is caused by damage to the intestinal mucosa due to careless stoma care or the use of rough materials. The edge of a tight hole in the plate or the rigid flange of a colostomy bag can also injure the intestine and cause bleeding. Bleeding usually stops spontaneously. But if the bleeding is heavy, you should consult a doctor.
Retraction (stoma retraction)
This is a gradual dislocation of the ostomy opening below the skin level; retraction can be along the entire circumference of the ostomy opening or partial. The presence of a funnel-shaped depression significantly complicates the care of the stoma and requires the use of special colostomy bags with a convex (concave) plate and additional care products (special pastes for leveling the surface of the skin and protecting it). If these measures are ineffective, surgical treatment (stoma reconstruction) is undertaken.
Parastomal hernias (hernias in the area of stoma formation)
This is a protrusion of the abdominal organs around the stoma due to weakness of the muscular layer of the anterior abdominal wall at the site of stoma formation, often against the background of increased intra-abdominal pressure. The risk of a hernia increases if the patient is obese. Prolonged cough and repeated vomiting in the early postoperative period contribute to the formation of hernias. To prevent this complication, elastic bandages are used immediately after surgery. Subsequently, the bandage is worn for 2-3 months.
Patients with even small parastomal hernias may experience pain, constipation, and difficulty using colostomy bags. For strangulated parastomal hernias, only surgical treatment is possible.
Complications after colostomy
After a colostomy, the following complications may occur:
- intestinal necrosis, which can be eliminated with repeated surgery;
- retraction or retraction of the stoma;
- bowel prolapse or evagination;
- paracolostomy abscesses that occur when an infection gets inside, causing redness and swelling in the colostomy area, increased pain, and increased body temperature;
- severe irritation of the skin around the stoma, which is a sign of fungal infection;
- colostomy strictures, which develop when tissue scars around the stoma, which is greatly complicated by the occurrence of intestinal obstruction.
Colostomy surgery
The intervention is carried out under general anesthesia - with the introduction of a special drug that puts the person into deep sleep and allows you not to feel pain. The operation can be performed:
- Laparoscopically
- through 2-3 small holes using special instruments and a laparoscope - a device with a light source and a camera at the end. To facilitate access, the abdominal cavity is filled with carbon dioxide, after which the doctor carries out all the necessary manipulations, looking at images of the internal tissues on the monitor screen. This method allows minimal tissue trauma, reduces blood loss and pain, and also accelerates healing, but is not suitable for all patients. - Either open method, through a large incision on the left, right or in the central area of the abdomen. After performing it, the surgeon carefully examines the abdominal cavity, dissects the intestine,, if necessary, removes its damaged fragment, and forms a temporary or permanent stoma from a healthy one. He then uses sutures or surgical staples to connect both sides of the wound on the abdominal wall, apply a bandage and attach a postoperative colostomy bag.
Oncology specialists carry out all types of operations to form any type of colostomy - quickly, without delays or queues. Our doctors are true experienced professionals in their field - candidates and doctors of medical sciences, who are fluent in both classical and high-tech innovative techniques. With us you can undergo a full examination, identify all existing diseases, perform the necessary studies, take tests and receive their results as soon as possible. We offer our patients comfortable rooms and do everything to make the stay at the Center as comfortable as possible for any visitor.
Stoma care at home
The stoma requires careful postoperative care. Typically, training in how to properly care for it is carried out by a nurse in the hospital, who is responsible for changing the patient’s colostomy bags and cleaning the colostomy. Afterwards, the patient must do this himself without fail.
To do this you need:
- Eliminate feces completely.
- Rinse the hole and the skin around it thoroughly with warm boiled water. Dry the colostomy with gauze pads.
- Treat the surface of the skin with Stomagesiv ointment or Lassara paste. Then apply gauze treated with Vaseline and cover everything with a sterile bandage. Then a gauze bandage is applied on top, which requires replacement every four hours.
- After the stoma has completely healed, it is allowed to use colostomy bags. We can talk about complete healing of the hole in the complete absence of inflammatory processes in this area, as well as when the mouth of the stoma does not protrude above the skin.
- Colostomy bags are changed in the evening or in the morning. To do this, you need to carefully remove the used fecal bag, remove any remaining fecal matter and thoroughly rinse the colostomy. Then it is necessary to treat the stoma with medications and fix the colostomy bag again.
To fix the fecal sac, in most cases, Coloplast paste is used, which has a small alcohol component. However, this drug does not cause any irritation and holds the colostomy bag well.
Sometimes, before gluing the fecal sac, a film is glued to the skin in order to prevent possible irritation or inflammation.
Colon stomas (colostomy)
For the process of digestion (fermentation) of food, the large intestine is of relatively little importance, since, with the exception of some substances, food is almost completely digested and absorbed in the small intestine. From the small intestine to the cecum - the initial part of the large intestine - an average of 500-800 ml of liquid contents arrives per day. In the colon, feces are formed due to the absorption of water, and fully formed feces enter the sigmoid colon. Thus, the segment of the intestine from which the colostomy will be formed will act as an artificial anus. Colostomy discharge has an odor that depends on the quality of food consumed. The volume and consistency of stool can be regulated by selecting an appropriate diet and the amount of fluid you drink (juice, water) per day.
Types of colostomy bags
Colostomy bags are divided into two types: one-component and two-component. The first are a disposable bag that is glued directly to the skin. When such a bag is filled approximately to the middle, it must be replaced with a new one.
Two-component ones have a base on an adhesive surface with a flange connection resembling a ring. This base is glued to the skin around the formed hole, and reusable or disposable fecal bags are hermetically attached to the flange ring. Such devices are much more convenient than single-component colostomy bags, since they allow the base to remain glued to the skin for several days, and only used bags need to be changed.
Among other things, colostomy bags are equipped with a special filter that helps eliminate gases and unpleasant odors.
The main pros and cons of various modifications of colostomy bags
Disposable colostomy bags
Single-component products are produced - a plate attached to the body and a receiving bag-container, which form one whole and are removed together as the bag is filled (up to half the volume).
Two-component colostomy bags consist of an adhesive-based plate and a replaceable bag. The plate is changed every 2-4 days. And the bag as it fills (up to half). The bag and the plate are firmly connected to each other using a flange.
Both receivers can be drainable or not.
Photo: Drainable one-component colostomy bag
Drainable bags have a channel (at the end opposite the attachment point) for discharging the contents. The drainage is closed with a clamp or other means. Through the drainage, as necessary, the contents of the collection are evacuated directly into the toilet, the hole is wiped and closed again with a clamp.
Photo: Non-drainable one-component colostomy bag
Pros:
- the flexible plate gives greater freedom
of movement to the patient, tightly adhering to the skin and ensuring odorlessness and confidence in fastening; - almost invisible under clothes
.
Minuses:
- more expensive to use (the cost of one product is from 100 rubles); the cost of use is also increased by the barrier paste for ostomy required for tightness (from 250 rubles);
- the adhesive base of the plate can cause irritation on the skin, despite the use of hypoallergenic compounds.
Reusable colostomy bags
There is also an option for containers for collecting intestinal contents. There are few similar offers in pharmacy chains and online stores.
Flaws:
- The main drawback of the design is its “unreliability”. A non-flexible ring with eyes is used. It is fixed to the body by pressing with an elastic band. The ribbon is worn around the torso. When changing body position (tilting, turning the body), leakage of the ring to the skin may occur. This causes the contents of the container to leak and produce an unpleasant odor. The solution in some situations is specially designed overlay plates that prevent excessive movement and maintain the stability of the connection.
- Another issue that confuses patients is its considerable size. The ring and the elastic band that holds it in place may be visible under clothing.
Advantages:
- Reusable colostomy bags are cheaper to use, since the main component of the product is used for a long time and repeatedly. Can be subjected to hygienic treatment (washing, sterilization). Only polymer bags with a ZIP clamp are regularly replaced with new ones; their cost is relatively low (20-40 rubles).
Photo: Reusable colostomy bag with fixing tape
Advantages and disadvantages of colostomy
In some cases, this procedure simply saves the patient’s life. This is the most important advantage of a colostomy. And with the use of modern devices, you can live comfortably even with such a diagnosis.
The main disadvantage of this procedure is the emotional and psychological factor, which often causes depression in patients. But this can also be overcome by listening carefully to the doctor, who is obliged to conduct explanatory conversations with the patient, tell him how to properly care for a colostomy, and what sensations may haunt the patient.
Many consider one of the main disadvantages to be the presence of an unpleasant odor. However, modern colostomy bags are equipped with powerful filters that eliminate odor, as well as special magnetic covers. Also, today there are various types of deodorants designed specifically for such purposes.
The availability of modern supplies and medications makes such a problem simply non-existent.
Will I be able to control the bowel movement if I have a stoma?
An intestinal stoma should be considered as an anus (an unnatural anus), but located in a different place, on the abdomen. A feature of the new unnatural anus is the absence of a sphincter apparatus, and therefore no holding function.
Often you will not feel the urge to defecate, feces and gases will pass spontaneously, you will not be able to control this process. However, having received the necessary advice on care and modern colostomy bags, you can cope with this new feature of self-hygiene and everyday life.
Modern colostomy bags compensate for the functions lost after surgery; the contents of the intestine (feces and gases) are reliably isolated in a sealed ostomy bag made of gas-tight materials. Colostomy bags are designed not only to collect stool, but also to protect the skin around the stoma, and are fixed to the skin of the abdomen immediately after the formation of the stoma at the end of the operation. Modern colostomy bags offered by manufacturers are compact and invisible under clothing.
Rehabilitation postoperative period
After the operation, after about two to three months, the person can return to a normal lifestyle and even work. In this case, the patient should not have any complications, and his profession should not be associated with heavy physical activity.
The main thing that rehabilitation should be aimed at is tangible support from family and friends, as well as overcoming the psychological barrier and a positive emotional attitude.
Colostomy is not a death sentence. People with this diagnosis continue to live full lives, get married and have children.
An important factor in the postoperative period is proper nutrition of patients. In this case, it is necessary to take into account the influence of various foods on the digestive processes. You should not eat foods that contribute to increased gas formation: eggs, cabbage, legumes, mushrooms, chocolate, onions, beer and carbonated drinks.
Best materials of the month
- Coronaviruses: SARS-CoV-2 (COVID-19)
- Antibiotics for the prevention and treatment of COVID-19: how effective are they?
- The most common "office" diseases
- Does vodka kill coronavirus?
- How to stay alive on our roads?
You should also exclude from your daily diet those foods that increase intestinal odors: garlic, eggs, fish, cheese, onions and various spices. With a colostomy, fractional meals are necessary. That is, eat often, but in small portions, and you also need to chew your food thoroughly.
You should also be careful to limit strengthening or debilitating foods in your diet to avoid possible constipation or diarrhea.
What diet is preferable for an ostomy patient?
It is very important that the diet of ostomy patients is balanced and varied, including a wide variety of foods. As a rule, no special diet is required. After surgery, you should return to your normal, regular diet. It is best to gradually expand the diet, adding one type of food per day, while noting changes in the nature and frequency of stool and drawing appropriate conclusions. You should try to eat slowly, often and little by little, chewing your food well.
It must be taken into account that some foods strengthen the stool, while others, on the contrary, cause it to weaken. By changing your diet, the patient can adjust the frequency of bowel movements to once or twice a day.
White bread, pasta, slimy soups, rice porridge with water, butter, boiled meat and fish, hard-boiled eggs, broths, mashed potatoes, black tea, cocoa, some fruits (pear, quince) have a fixing effect.
Laxative: black rye bread, oatmeal, fried meat, fish and lard, raw milk, kefir, yogurt, sour cream, most vegetables and fruits (cabbage, beets, cucumbers, grapes, apples, plums, figs).
Beans, cabbage, sugar, and carbonated drinks contribute to increased gas formation. An unpleasant odor from the colostomy may appear if the patient eats too many eggs, onions, and garlic.
conclusions
Colostomy is an operation in which part of the colon is brought out through an artificially created opening in the abdominal cavity and forms a colostomy, a kind of fistula that facilitates the removal of gases or feces. This operation is indicated for various intestinal diseases, and is also often a companion for cancer patients. Most often, for malignant neoplasms, permanent colostomies are placed, with which people live their entire lives.
Such an operation often helps save a person’s life, and with the availability of modern accessories and tools, people subsequently even forget about their delicate problem. Having a colostomy is not a death sentence; the main thing is to overcome the psychological barrier in this problem and take it for granted. People with a colostomy continue to live full, normal lives, get married, give birth and raise children. The main thing is to follow a healthy diet, do not forget about daily personal hygiene, and the problem will disappear on its own.
More fresh and relevant information about health on our Telegram channel. Subscribe: https://t.me/foodandhealthru
We will be grateful if you use the buttons:
Stoma is not a death sentence
In many countries, active work is underway to adapt people with certain characteristics to the social environment. The countries of North America and Europe have been very successful in this. Entire communities of people with stomas (urostomies, colostomies, tracheostomies, etc.) have been created and supported there. People with similar problems communicate and share their experiences and knowledge.
Under the auspices of the UN, since 1993, World Ostomy Day has been celebrated on October 2.
Thanks to new inventions and care products, patients with the consequences of operations can lead a normal, active lifestyle. These include colostomy bags and hygiene products. They are available to a wide range of buyers and are easy and convenient to use. Carrying out operations and ostomy often gives people more than one year of life, the opportunity to enjoy the world and communicate with family, friends, work and play sports. And the fullness of life of a patient with an ostomy largely depends on his optimism and the support of loved ones.
Diarrhea
May be caused by the following reasons:
- consumption of certain foods: spicy foods, beans, peas, chocolate, plums, spinach, raw fruits, alcohol (especially beer),
- nervous reaction, bad mood or travel-related stress.
What to do?
Try for a while not using those foods or drinks that you think contribute to diarrhea, and gradually reintroduce them into your diet in the future. If diarrhea continues, consult a doctor.