Colon cancer is the second most common cancer in the world. Thus, in the United States, colorectal cancer is diagnosed in more than 140,000 people annually and causes about 50,000–60,000 deaths per year. This is a huge number considering that the disease is potentially curable when diagnosed at an early stage.
Colon cancer stages
The stage of cancer is an important indicator on which treatment tactics and prognosis for the patient primarily depend. Colorectal cancer has 4 main stages:
- The first stage is the earliest. Such a tumor is located in the mucous membrane and does not grow deep into the intestinal wall.
- Stage 2 cancer grows deeper, sometimes through the entire intestinal wall.
- In stage 3 colon cancer, tumor cells penetrate into the lymph nodes close to the tumor (regional).
- At stage 4, distant metastases are detected, for example, in the liver, bones, and brain. Complications develop in the form of peritoneal carcinomatosis and ascites: cancer cells “spread” over the surface of the peritoneum, and fluid accumulates in the abdomen. This worsens the patient's condition and prognosis.
Who is at risk?
Although colorectal cancer can occur at any age, more than 90% of patients develop cancer over the age of 40, with the risk of developing the disease doubling every 10 years. In addition to age, risk factors include a family history of colorectal cancer, polyps and ulcerative colitis, as well as colon polyps and cancers of other sites, especially the breast and uterus.
Signs of Colon Cancer
In the initial stages there are often no symptoms. Because of this, the disease is often diagnosed in late stages and the prognosis worsens. The first symptoms of colon cancer are nonspecific, they are very similar to the manifestations of other diseases, because of this, many patients do not consult a doctor on time:
- Changes in the frequency and nature of stool, constipation, diarrhea. This symptom should be alarming if it persists for four weeks or longer.
- Blood in the stool, bleeding from the rectum.
- After visiting the toilet, there is a feeling that the intestines are not completely emptied.
- Pain, discomfort in the abdomen, feeling of heaviness, increased gas formation.
- Weight loss for no apparent reason.
- Constant weakness, increased fatigue.
With stage 4 colon cancer, various symptoms associated with metastases occur. The condition worsens significantly with the development of intestinal obstruction, peritoneal carcinomatosis and ascites.
Symptoms
In case of intestinal cancer, the first symptoms are manifestations of general intoxication, developing due to the growth of a malignant neoplasm and the immune response, as well as due to impaired digestive function. Among them:
- fatigue, general weakness;
- joint pain as a result of an autoimmune reaction;
- a steady increase in temperature to a little over 37 degrees;
- unexplained weight loss;
- aversion to the smell of meat or some other products;
- nausea;
- pale skin;
- flatulence, bloating, colic;
- dark stool with lots of mucus.
Subsequently, as the intestinal tumor grows, the symptoms increase and new signs appear;
- cramping abdominal pain with a frequency of 15-20 minutes;
- asymmetrical increase in abdominal volume;
- frequent vomiting due to general intoxication;
- alternating diarrhea and stool retention;
- traces of blood in the stool.
When intestinal obstruction occurs due to the tumor blocking the intestinal lumen, the intestinal wall stretches excessively, blood circulation in it is disrupted, resulting in necrosis of the deformed tissue and peritonitis.
Diagnostic methods. Screening.
The main method for diagnosing colon cancer is colonoscopy. It is an endoscopic examination during which an instrument in the form of a thin flexible tube with a video camera at the end is inserted into the intestine through the anus. During a colonoscopy, pathologically altered areas of the mucous membrane can be detected and a biopsy can be performed to obtain a fragment of altered tissue for examination under a microscope. Diagnostic methods such as CT, MRI, PET scanning, radiography of bones, spine, chest, ultrasound of the abdominal cavity, and intestinal radiography with contrast help to assess the extent of cancer spread and identify metastases.
Advantages of going to Ilyinskaya Hospital
The treatment strategy for patients with colon cancer at the Ilyinskaya Hospital is based on the concept of a multidisciplinary combined and integrated approach, combining the use of modern surgical technologies with the achievements of radiation, drug and immunotherapy. Each clinical case is reviewed at an oncology council (Tumor-board), which includes: a chemotherapist, an oncologist surgeon, a radiologist, a radiologist, an oncopsychologist, and a rehabilitation physician. This approach allows us to develop the most effective personalized treatment tactics for the patient, take into account all individual nuances and achieve maximum efficiency.
Modern methods of treatment
For invasive tumors, colectomy is most often used - removal of all or part of the intestine. The surgeon must remove the tumor, including the overlying and underlying unaltered areas. The remaining ends are connected and an anastomosis is performed. If this is not possible, a colostomy is formed - an opening in the skin for the passage of stool. Most often, a colostomy is placed temporarily and later closed. But sometimes you have to leave it forever. If removal of colon cancer is impossible, but the tumor blocks the intestinal lumen and leads to intestinal obstruction, palliative intervention is performed. A stent is installed into the intestinal lumen - a frame with a mesh wall, which restores patency. If single metastases are detected in other organs, sometimes they can also be removed surgically.
Colorectal cancer: etiology, pathogenesis, therapy
Malignant tumors of the colon are the third most common cancer among the adult population of the planet, and colorectal cancer (CRC) has taken second place in the structure of cancer mortality. Timely diagnosis of early forms of CRC is a priority in modern oncology.
Definition and classification
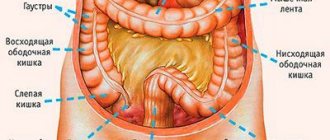
Malignant tumors of the colon are neoplasms whose substrate is the epithelial cells of the organ. In many ways, the features of the clinical course of the disease, the nature of metastasis, the choice of diagnostic measures and medical tactics depend on the localization of the primary lesion (often there are several of them). In most cases, the tumor develops in one or several anatomical areas:
- right parts of the colon (cecum, ascending and transverse colon, hepatic flexure);
- left parts of the colon (sigmoid, descending colon, splenic flexure);
- rectum (lower, middle, upper ampullary sections) [2-point 2.1.4, 6-point 1.1].
According to the histological structure, CRC in 90% of cases belongs to adenocarcinoma of varying degrees of malignancy [6-page 9]. Highly differentiated variants (G1) have a favorable course and prognosis, while undifferentiated tumors quickly progress and lead to complications.
Etiology and pathogenesis
In most cases, colorectal cancer develops against the background of existing pathological changes in the mucous membrane of the organ. The risk of malignant cells appearing in this area is especially high in persons suffering from colon adenomatosis, Mut-YH-associated polyposis, Lynch syndrome and chronic intestinal diseases (Crohn's disease, ulcerative colitis, etc.) [1-point 1.2, 6-point 1.2 ].
Traditionally, non-modifiable and modifiable risk factors for the development of colorectal cancer are distinguished. Non-modifiable risk factors include gender (the likelihood of developing colorectal cancer is higher in men), age, ethnicity, hereditary background and high stature (in patients with acromegaly, the risk of developing a malignant tumor in the colon is 2.5 times higher than in the general population). An important role in determining the risk of developing CRC is played by the geographic area in which a person lives and his socio-economic status: in developed countries (USA, Canada and Japan) CRC is more common than in economically less developed countries.
Among the modifiable risk factors for developing colorectal cancer are:
- unhealthy diet, with excess consumption of red meat, animal fats, sugar and insufficient intake of micro- and macroelements (selenium and calcium) and vitamins (eg B vitamins, vitamin D3);
- low dietary fiber intake;
- dysbacteriosis, disturbance of intestinal microflora;
- excess body weight;
- sedentary lifestyle;
- diabetes;
- smoking and alcohol abuse;
- unstable stool (diarrhea, constipation).
Additionally, the development of colorectal cancer is promoted by cholecystectomy (removal of the gallbladder), radiation therapy in the pelvic area and long-term systematic exposure to carcinogens (toxic chemicals, infectious agents, pharmaceuticals, etc.). Often the “trigger mechanism” in the development of neoplasms is stress or serious illness and the immunodeficiency that develops against them [2,3,6].
Symptoms and stages of development of colorectal cancer
The clinical picture of CRC is determined by the location of the tumor and the type of its growth (into the intestinal lumen, along the wall of the organ). When the right parts of the colon are affected, the prevailing manifestations of the disease are:
- asthenic syndrome (weakness, general malaise, weight loss, anemia, etc.);
- systematic causeless increase in body temperature, often to subfebrile levels;
- sensation of a neoplasm and/or the presence of a tumor detectable by palpation in the right half of the abdomen.
Such formations, as a rule, are characterized by slow growth and do not “declare themselves” for a long time. Intestinal obstruction with damage to the right parts of the colon develops rarely and only in the terminal stage of the disease, when the tumor reaches a large size.
For cancer of the left half of the colon, another triad of symptoms is considered typical:
- disruption of intestinal function, dyspeptic symptoms (constipation or diarrhea, discomfort and pain in the abdomen, tenesmus, etc.);
- discharge from the anus of various types (mucous, purulent, bloody);
- chronic or acute intestinal obstruction.
Often, the patient learns about his diagnosis only during emergency hospitalization in the surgical department. With acute intestinal obstruction, the patient experiences intense cramping pain in the abdomen, repeating every 10-15 minutes.
Cancer of the rectum and anal canal is characterized by a clear clinical picture. The most common manifestation of the disease is pathological discharge from the anus. 75-90% of patients have blood in their stool. Often the act of defecation is accompanied by painful sensations. In advanced cases, pain in the rectum becomes permanent.
Other typical symptoms when the distal parts of the intestine are affected are: a feeling of incomplete emptying, tenesmus (false urges) up to 15-20 times a day, constipation, diarrhea or their alternation. In the progressive stages of the disease, asthenic syndrome develops: sudden weight loss, irritability, and changes in skin color are noted. Due to intoxication and anemia as a result of chronic intestinal bleeding, the patient constantly feels general malaise and weakness.
Often the tumor metastasizes to neighboring organs (bladder, uterus, etc.) and anatomical structures (nerves, blood and lymphatic vessels). In advanced cases, fistulas may form and peritonitis may develop [7-pages 3-4].
Diagnostics
Patient refusal or the presence of contraindications to endoscopic examination with targeted biopsy are one of the main obstacles to timely diagnosis of colorectal cancer. In some cases, a single colonoscopy does not allow obtaining a reliable morphological assessment, so the patient is prescribed a repeat examination.
CRC diagnostic standards include:
- medical interview, medical history, examination of the patient, including digital rectal examination;
- laboratory tests (general and biochemical blood tests, stool occult blood test, coagulogram, assessment of tumor markers, e.g., cancer antigen CA19-9 and cancer embryonal antigen);
- endoscopic examination (according to clinical recommendations, the most accurate examination method is a total colonoscopy with sampling of material from 3-5 different areas; if this is not possible, an X-ray examination of the intestine (irrigoscopy) or CT colonography is indicated);
- CT colonography or intestinal radiography;
- genetic testing (determining mutations in certain genes);
- search for distant foci of the disease (CT of the lungs, ultrasound of the abdominal cavity and retroperitoneal space, ultrasound of the lymph nodes, osteoscintigraphy, MRI of the pelvic organs with contrast, etc.).
Diagnosis of rectal tumors is usually not difficult. Digital examination and rectoscopy with biopsy in almost 100% of cases make it possible to accurately establish the diagnosis [1,6-point 2].
Treatment
The choice of treatment tactics is determined by a medical commission composed of oncologist surgeons, chemotherapists and radiologists. The preferred treatment for colorectal cancer is surgery. Surgical treatment can be radical or palliative. In the latter case, surgical intervention can reduce the risk of complications and/or improve the patient’s well-being.
At stages 0-I, only organ-preserving operations are possible. As the pathology progresses, surgical intervention is supplemented with the prescription of drugs (targeted drugs and chemotherapy) and/or radiation therapy. Radical treatment is often performed in two stages: removal of the tumor and removal of the colostomy, then restoration of the integrity of the intestinal tube [1.6-point 3].
Prognosis and prevention
A healthy lifestyle and a diet rich in dietary fiber form the basis of CRC prevention. Persons at risk (familial adenomatosis of the colon, intestinal polyposis, chronic inflammatory diseases of the gastrointestinal tract) should regularly visit a doctor and undergo follow-up examinations. To reduce the risk of relapse (develops in 15-20% of patients), patients who have undergone treatment are recommended to undergo dynamic observation.
Early detection and radical treatment of colorectal cancer are key factors for a favorable prognosis: the five-year survival rate of patients with timely treatment reaches 80%. At stages III-IV of the development of the malignant process, patients develop serious complications, their health worsens and their quality of life decreases [5].
Bibliography
- Clinical recommendations of the Ministry of Health of Russia: Cancer of the colon and rectosigmoid region, 2022
- Lebedeva L.N. et al. Epidemiology of colon cancer literature review, 2016; pp.1-40
- Prudnikova Ya.I. and others. Colorectal cancer: risk factors and protection // “Experimental and clinical gastroenetrology”, 2017; 145(9), pp.1-10
- Sidorova A.N. and others. Modern tactics in the diagnosis and treatment of early colon cancer (literature review) // Scientific notes of St. Petersburg State University named after. Academician I.P. Pavlova, 2020; pp. 1-10
- Denisenko V.L., Gain Yu.M. Complications of colorectal cancer: problems and prospects // News of surgery, 2011; 19/(1), pp.1-9
- Clinical guidelines of the Russian Ministry of Health: Rectal cancer, 2020
- Klyaritskaya I.L., Kurchenko M.G. Colorectal cancer // Crimean therapeutic journal, 2005; 2, pp. 15-20
Author: Emilia Kiseleva
Chemotherapy for colon cancer
Chemotherapy drugs for malignant intestinal tumors help solve various problems:
- Reduce tumor size before surgery. This chemotherapy is called neoadjuvant.
- Destroy any cancer cells that may remain in the patient's body and reduce the risk of recurrence after surgery. This is adjuvant chemotherapy.
- For advanced, inoperable cancer, chemotherapy can help control symptoms and increase life expectancy.
Radiation therapy Radiation therapy is most often used before surgery to shrink the tumor. It is prescribed alone or in combination with chemotherapy.
Rehabilitation
In the first few days after surgery, the patient is given intravenous nutrition. In the future, it is necessary to adhere to special nutritional principles, consuming only liquid and pureed foods. A special diet for intestinal cancer is prescribed taking into account the individual characteristics of the body, but the menu must include liquid dishes, fresh and boiled vegetables and fruits. In addition, during the recovery period it is necessary to avoid physical and psychological stress, regularly visit a doctor, and take prescribed tests.
Survival prognosis for colon cancer
The prognosis is determined by the five-year survival rate, which, in turn, depends on the stage:
- At the first stage, colon cancer is treated quite successfully, the five-year survival rate is maximum and is 92%.
- At the second stage - 63–87%, depending on how far the cancer has spread.
- At stage 3 – 53–69%.
- How long do you live with stage 4 colon cancer? The chance of being alive 5 years after diagnosis is 11%. The chances are low, but treatment methods are improving. Even if remission is not possible, doctors will try to prolong the patient’s life as much as possible.
Booking Health helps you get treatment abroad
If you want to find out prices for treatment of colon cancer in Germany, treatment of colon cancer in Israel or other countries, contact the medical tourism operator Booking Health. Fill out the “Send a request” form on the company’s website, and a medical consultant will contact you on the same day.
Booking Health specialists will also help you with such important points:
- Choosing the right clinic based on the annual qualification profile
- Direct communication directly with the attending physician
- Preliminary preparation of a treatment program without repeating previously conducted examinations
- Ensuring favorable prices for clinic services, without surcharges and coefficients for foreign patients (savings up to 50%)
- Make an appointment for the desired date
- Control of the medical program at all stages
- Assistance in purchasing and shipping medications
- Communication with the clinic after completion of treatment
- Control of invoices and return of unspent funds
- Organization of additional examinations
- Service of the highest level: booking hotels, plane tickets, transfers
- Translator and personal medical coordinator services
Types of operations
In my work, I use the most modern technologies, which in most cases make it possible to perform reconstruction without a colostomy.
For colon cancer, the following operations are performed:
- Right hemicolectomy – removal of the right half of the colon, the right half of the mesentery (fat containing feeding vessels and lymph nodes) with lymph nodes of the 1st and 2nd orders. Used for cancer of the right colon.
- Extended right hemicolectomy with complete mesocolonectomy (CME) – removal of the right half of the colon and most of the transverse colon with complete removal of mesenteric fatty tissue, skeletonization of vessels that cannot be removed. Used for cancer of the hepatic flexure and transverse colon. This operation is more traumatic, so it should not be used for all tumors of the right half of the colon.
- Resection of the splenic flexure - removal of the splenic flexure of the colon. The complexity of this operation lies in the need to perform lymphadenectomy in 2 directions at once: to the superior and inferior mesenteric arteries.
- Left-sided hemicolectomy - removal of the left half of the colon, the left half of the mesentery (fat containing feeding vessels and lymph nodes) with lymph nodes of the 1st and 2nd orders. Used for cancer of the left colon.
- Resection of the sigmoid colon - partial or complete removal of the sigmoid colon with the mesentery and lymph nodes of the 1st and 2nd order. Performed for sigmoid colon cancer.
All operations are performed by me both openly and laparoscopically. In my work, I give preference to laparoscopic interventions, after which patients recover faster and experience less discomfort without compromising the radicalness of the treatment.
In men
Men usually get colorectal cancer. Its symptoms are as follows:
- Anus hurts;
- Diarrhea and constipation;
- Blood or mucus appears in the stool.
If the process of metastasis has begun, the prostate may be affected.
The neoplasm can be palpated by a proctologist.
Cancer in men can develop due to the use of harmful substances, poor diet, the presence of intestinal polyps, ulcers, colitis, hemorrhoids, and excess weight.
The first organ in which metastases develop in this type of cancer is the liver. The process occurs at the last stage of the disease. With proper treatment, a patient with this diagnosis can live up to two years.
Metastasis can also occur in the pelvic organs, peritoneum, pancreas, lungs, retroperitoneal space, and bladder.
The processes of metastasis are as follows:
- Initially, the tumor grows into the fatty tissue;
- Perforation of the colon;
- Cancer cells are found in neighboring organs.
First, the rectum is examined by palpation.
Next, colonoscopy and sigmoidoscopy are performed. During the latter, the doctor examines the rectal mucosa. Sections of the sigmoid colon can be examined.
During endoscopy, the surgeon performs a biopsy, followed by a histological examination.
To diagnose colon cancer in the early stages, protein levels are determined. Thanks to these tumor markers, bowel cancer can be detected in the absence of symptoms.
Treatment
Comprehensive treatment is recommended: surgery, chemotherapy, radiation therapy, radiotherapy.