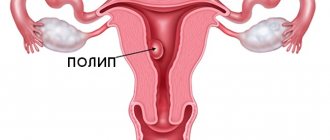
An endometrial polyp is a growth on the inner lining of the uterus into its cavity. It is formed due to excessive growth of cells in the inner lining of the uterus.
If the polyp is attached to the surface by a narrow stalk, then it is called “pedunculated”; if there is no stem - “on a broad base.”
The very concept of “polyp” means an abnormal growth of a certain type of tissue that protrudes above the membrane into the cavity of the organ. Polyps can be found in the nose, stomach, and bladder. An endometrial polyp is a growth specifically from the mucous membrane of the uterus, but this neoplasm is also found in the cervix.
Thus, there are two types of uterine polyps based on their location:
- endometrial polyp of the uterus;
- cervical polyp.
As a rule, such abnormal proliferation of endometrial cells occurs in 10% of women. Most often, an endometrial polyp occurs on an elongated stem. The size of such a neoplasm can vary from 1-2 mm to 3-4 cm, sometimes more. A pedunculated polyp can even penetrate through the cervix into the vaginal cavity. If the polyp reaches a significant size (from 8-10 mm), then it may have thin blood supply vessels.
An endometrial polyp is a benign neoplasm. In some cases, its cells can degenerate into cancerous ones, and then it becomes a malignant tumor. According to scientific research, about 0.7% of endometrial polyps contain adenocarcinoma cells.
Reasons for appearance
Endometrial hyperplasia and polyps, that is, an increase in the number of cells in the inner lining of the uterus or cervix, can occur for several reasons.
Until now, scientists and doctors have not clearly established what the main reason for the appearance is. Hormonal disorders are currently considered the main risk factor for endometrial hyperplasia. In particular, an excess of estrogen and a lack of progesterone in a woman’s body affects her.
Risk factors for education are:
- anovulation;
- persistent follicle syndrome;
- hyperglycemia (with diabetes);
- presence of follicular cysts;
- granulosa cell tumors;
- menopausal syndrome;
- obesity;
- trauma to the uterine cavity (long-term wearing of an intrauterine device);
- abortions or miscarriages;
- complications during or after childbirth;
- chronic inflammatory diseases of the internal genital organs, endometritis;
- immunodeficiency states;
- thyroiditis, thyroidosis and other diseases of the thyroid gland.
Familial adenomatous polyposis
Familial adenomatous polyposis (FAP) is a hereditary disease in which multiple formations develop on the mucous membrane of the colon, otherwise known as polyps. In most cases, there are no clinical symptoms, and the diagnosis is an “incidental finding” during routine examinations. This condition requires constant monitoring, since without appropriate treatment it leads to the development of a malignant tumor of the colon before the age of 40 years. The incidence is 1 in 8,000–14,000 people.
Polyps are detected by the age of 15 in 50% of patients, and by the age of 35 in 95%. This rare genetic disease is based on chromosomal rearrangements in the long arm of chromosome 5, affecting the APC gene (adenomatous polyposis coli gene), both in tumor cells (non-inherited mutation) and in normal cells (hereditary mutation), which leads to loss of suppressor genes that provide prevention of tumor transformation of cells.
FAP is a disease with an autosomal dominant mode of inheritance, that is, the disease will manifest itself in each subsequent generation. In FAP, there are ≥ 100 adenomatous polyps growing on the surface of the colon in the colon and rectum. If >100 polyps are detected during colonoscopy (i.e., the doctor evaluates the inside of the colon using an endoscope), patients, as well as their first-degree relatives, should undergo genetic testing to identify the specific mutation. If genetic testing is not possible, it is necessary annually, starting from the age of 12, to screen and examine the patient’s relatives using sigmoidoscopy - examination of the rectal mucosa; the frequency of screening examinations decreases with each decade. The probability of developing adenomatous polyposis of the colon in children of patients by the age of 35 is 50%, so they require annual sigmoidoscopy. Polyps are usually evenly distributed throughout the colon from the cecum to the anus, making more burdensome and expensive procedures (colonoscopy and barium enema) impractical. If polyps cannot be controlled, or if the colon and rectum are not removed, the likelihood of developing colon cancer by age 70 is estimated to be 80%.
Clinically, the disease is most often asymptomatic - hidden blood loss in the feces may be observed, but various extraintestinal formations of both benign and malignant nature (Gardner's syndrome) can also be observed.
Patients also have an increased risk of duodenal cancer (5–11%), pancreatic cancer (2%), thyroid cancer (2%), brain tumor (medulloblastoma with an incidence of <1%), liver cancer (and hepatoblastoma - malignant tumors developing in childhood, with an incidence of 0.7% in children aged <5 years).
Timely genetic diagnosis makes it possible to identify the “invisible killer”, prevent the development of many dangerous pathologies and prolong the patient’s life, as well as help determine tactics for his loved ones.
Sign up for a medical genetic consultation Tel.: 8 495 304 30 40
Classification
Depending on the histological structure, a classification of endometrial polyps has been developed. So, experts distinguish the following types:
- glandular polyp - the structure on histology is represented by glands and stroma;
- glandular-fibrous polyp consists of connective tissue elements and glandular structures;
- fibrous polyp – connective tissue only;
- adenomatous polyp is a precancerous neoplasm that consists of glandular and atypical cancer cells.
It is also characteristic that endometrial glandular polyps occur in young women, while adenomatous and fibrous polyps occur more often in older women during menopause.
A functional polyp is also identified, which, unlike basal type polyps, can change during the menstrual cycle. The functional type polyp consists of epithelial cells.
Symptoms of adenomatous and glandular polyposis
The first sign to start sounding the alarm is menstrual irregularities. Although sometimes the clinical picture is minimal or absent altogether.
- Bleeding and heavy menstruation. In the middle of the cycle, a woman may suddenly start bleeding, or the menstruation itself may proceed with copious amounts of blood. They can be considered abundant when the duration increases by several days or the blood volume exceeds 150-200 ml. Usually menstruation ends on the third or fifth day; if its duration exceeds seven days, then this is a reason to contact a gynecologist. But you should not pay attention to exceptions that may be caused by increased weight or a sudden change in climate, although visiting the doctor once again will not harm anyone.
- Lack of menstruation. All women may experience slight delays from time to time. In this case, it is worth waiting a few days, during which to observe possible changes in the body. But if menstruation, which always arrives on time, has been absent for a week, and pregnancy is excluded, then this indicates that it is urgently necessary to contact an antenatal clinic.
- Pain in the lower abdomen. Pain in the lower abdomen can be caused by both gynecological diseases and other problems; moreover, this pain can be false, that is, radiate from other parts of the body, and the woman thinks that she has a stomach ache. In any case, you need to visit a doctor who will determine the cause. Another symptom of endometrial polyposis is discomfort and pain during sexual intercourse. Any such signal should alarm a woman.
- Infertility. An undiagnosed polyp provokes infertility in a woman, since the outgrowths do not allow the fertilized egg to attach to the walls of the uterus. In most cases, it is during the treatment of infertility that polyps in the endometrium are identified. Unfortunately, patients do not seek help from a doctor in a timely manner, since polyposis is asymptomatic, which leads to a poor diagnosis.
One of the main reasons for the development of polyposis in the uterine cavity is considered to be heredity. This factor has been identified in 50% of women suffering from this disease. If the older generation has a tendency or polyposis itself, then the woman needs to seriously engage in examination to identify polyps in the uterus.
Clinical symptoms of endometrial polyp
If the neoplasm is small in size, then there are no signs. As a rule, such polyps are found only with an ultrasound of the pelvic organs.
When the polyp reaches a significant size or there are quite a lot of such formations, characteristic symptoms appear. Women complain about:
- menstrual irregularities;
- the appearance of intermenstrual bleeding from the vagina;
- lower abdominal pain;
- discomfort and pain during sexual intercourse;
- cramping pain when the polyp enters the cervical canal;
- the appearance of watery whitish discharge in large quantities.
Menstrual irregularities in young women are manifested not only by bleeding between periods, but also by metrorrhagia, too heavy menstruation. Blood may also be released during sexual intercourse. With the onset of menopause, bleeding from endometrial polyps can be episodic. Also, the consequence of polyposis can be infertility in women, recurrent miscarriage. Since the endometrial polyp has scant symptoms, you need to pay attention to the slightest disturbances and immediately refer the patient for additional examinations.
Colon polyps and polyposis
Polyps and adenomas are essentially intestinal tumors.
A tumor is a newly formed tissue.
The cause of tumors is a genetic pathology, as a result of which the correct and adequate growth in the cell is disrupted and it begins to develop uncontrollably, and with a violation of its differentiation.
All tumors, according to the nature of their growth, are divided into malignant and benign.
What is a "polyp"?
A polyp is a growth of glandular epithelium.
In their shape, polyps can be in the form of a mushroom cap on a thin or thick stalk.
Reasons for the formation of polyps
It is quite difficult to establish the exact cause of a polyp in a particular case, since they often do not manifest themselves in any way. Most often, such benign polyps are discovered by chance.
Such patients usually consult a doctor with complaints of intestinal dysfunction, discomfort, pain in the anus, and sometimes pathological discharge in the form of blood or pus with mucus.
Such symptoms are also typical for other diseases of the rectum and colon, for example, proctitis, hemorrhoids, anal fissure, colitis, rectal or colon cancer, etc.
Occurrence
It is not possible to indicate exact figures for the occurrence of polyps and adenomas, since most of them are simply never detected. According to the work of Russian and foreign researchers, it was found that on average the frequency of colon adenomas ranges from 2.5 to 7.5% of the total number of patients examined.
But, of course, the true incidence of colon polyps is higher, since during this examination the researchers did not examine other parts of the colon, where about 50% of all colon polyps and adenomas are located.
Among the reasons, or more precisely factors, that influence the appearance of colon polyps, one can note the state of the environment, as well as physical inactivity. An equally important factor in the formation of colon polyps is the nature of nutrition.
As you know, in modern economically developed countries, people's diets are dominated by foods rich in fat and carbohydrates, and the amount of plant fiber is low. This causes poor colon motility, stagnation of feces and bile acids, which affect the intestinal mucosa. This in turn affects the composition of the natural microflora of the large intestine, which also affects the composition of the enzymes that it secretes.
Researchers also found a relationship between the formation of polyps and factors such as male gender, vascular atherosclerosis, malignant tumors, diverticula in the gastrointestinal tract, and inflammatory bowel diseases.
Classification of benign tumors of the colon
All benign tumors of the colon can be divided into:
1. Adenomas:
- tubular
- villous
- tubular-villous
2. Adenomatosis (adenomatous intestinal polyposis)
Tumor-like lesions. These include:
1. Hamartomas:
- Peutz-Jeghers polyp and polyposis
- juvenile polyp and polyposis
2. Heterotopia 3. Inflammatory polyp 4. Hyperplastic (metaplastic) polyp 5. Benign lymphoid polyp and polyposis 6. Deep cystic colitis 7. Endometriosis
Hyperplastic polyps by small sizes (up to half a centimeter). It rises slightly above the level of the mucosa and is a growth of soft consistency and normal color.
Glandular and glandular-villous polyps are characterized by larger sizes (up to 2-3 cm in diameter). As a rule, such polyps have a stalk, sometimes even a wide base. The color of such polyps is normal, like the color of the colon mucosa, but their consistency can be denser. Often these polyps can ulcerate or bleed.
Villous adenomas by a lobulated structure. This surface looks like a raspberry. The size of such polyps is larger than that of tubular adenoma.
Classification of polyps
The most common type of all benign colon tumors are epithelial tumors. They occur in 92% of cases of all benign neoplasms. Moreover, it is glandular tumors that are most susceptible to malignant degeneration - malignancy.
According to their histological structure, colon polyps are divided into:
- hyperplastic (2%)
- glandular (51.6%)
- glandular-villous (21.5%)
- villous (14.7%)
It is noted that the size of the polyp affects the risk of its malignancy - the larger it is, the higher the risk of malignant degeneration of the polyp.
In addition, colon polyps can be:
- single
- multiple
There are also diffuse (familial) polyposis.
With this disease, a significant number of polyps are noted, and not only in the colon. It is worth noting that the number of polyps also affects the risk of malignancy. It is higher with multiple polyps (reaches 20%). Single polyps become malignant less often - in 1-4% of cases.
With familial polyposis, the risk of malignant degeneration is quite significant and reaches 80-100%.
A villous tumor usually has a reddish color upon external examination (via sigmoidoscopy or colonoscopy) due to the abundance of blood vessels in it. Such vessels are usually easily injured and bleed, which is important to consider, since this is not a sign of malignancy, but only a characteristic feature of them.
Manifestations of colon and rectal polyps
Most often, benign neoplasms of the rectum and colon in patients are asymptomatic, or are detected accidentally during endoscopic examination (colonoscopy, sigmoidoscopy) for other diseases.
If the polyp reaches a larger size (up to 2-3 cm), then pathological discharge appears (bloody, mucous). Patients may complain of discomfort in the abdomen and anus, and pain. Intestinal motility disorders appear, such as constipation or diarrhea.
So, the main manifestations of colon polyps are:
- Bleeding from the rectum. Rectal bleeding can be a sign of various proctological diseases, for example, hemorrhoids, anal fissure, ulcerative colitis, rectal or colon cancer. Therefore, it is very important to not be shy when rectal bleeding occurs and immediately go to a proctologist to find out the cause.
- Constipation. They are associated with partial intestinal obstruction due to polyps. With significant sizes, polyps interfere with normal intestinal motility, resulting in a slowdown in intestinal passage.
- Stomach ache. This symptom is less common with polyps and is mainly associated with inflammatory changes in the polyp.
Diagnosis of polyps of the rectum and colon
Almost all types of rectal or colon cancer arise initially from polyps. But polyps grow rather slowly, usually over several years. Therefore, research methods play a very important role in the prevention of colon cancer. Detecting the malignancy of a polyp at its early stage ensures the success of its cure in 90%.
The very first research method in proctology is digital rectal examination.
This method allows the doctor to assess the condition of the rectum up to 10 cm from the edge of the anus. This research should always be applied. Digital rectal examination can also identify other diseases of the rectum, such as hemorrhoids, rectal fistulas, and anal fissures. In addition, such a study allows you to determine the condition of the prostate in men and identify diseases of the surrounding tissue (cysts and tumors).
This is followed by another, no less important diagnostic method for diseases of the colon and rectum - sigmoidoscopy.
Before performing sigmoidoscopy, the patient is given a cleansing enema and laxatives are prescribed. The sigmoidoscopy method cannot replace any other methods, such as fluoroscopy, ultrasound, etc., since it allows the doctor to see with his own eyes the presence of polyps and assess the condition of the rectal wall.
It is known that more than half of all colon polyps are localized in the rectum and sigmoid colon, i.e. they can be detected with a proctoscope.
If polyps are detected in the sigmoid colon, it is recommended to study higher parts of the colon, since quite often such polyps are combined with polyps in other parts of the gastrointestinal tract.
For this purpose, X-ray contrast methods are used, as well as endoscopic methods for examining the stomach and intestines - gastroscopy, colonoscopy.
Irrigoscopy is an X-ray method for examining the colon. It consists of injecting a barium suspension into the colon, after which an x-ray is taken. Irrigoscopy allows you to identify polyps larger than 1 cm. Small polyps can be identified less frequently using irrigoscopy. In this case, a colonoscopy is recommended.
Colonoscopy is an endoscopic method for examining the colon. It differs from sigmoidoscopy in that it uses a longer, flexible tube that is inserted into the rectum and advanced above the sigmoid colon. To perform a colonoscopy, careful preparation of the patient with enemas is required.
Biopsy - this method consists in the fact that, having discovered a suspicious area of tissue, the doctor takes a piece of it for histological examination. A biopsy can be performed during a sigmoidoscopy or colonoscopy. This is the only method that allows us to reliably state whether there is cancer in a given case or not.
Fecal occult blood analysis: this is an important method for studying gastrointestinal pathology. It involves examining stool for the presence of blood components. To do this, you must follow your doctor's instructions. They consist in the fact that the day before the analysis you should not brush your teeth or take certain medications (in particular iron supplements). A stool occult blood test is not specific for polyps. Polyps may not bleed at all, and the presence of blood in the stool can occur in many other diseases of the rectum and colon, which we have already mentioned.
Among the new methods for studying the gastrointestinal tract for the presence of polyps and other neoplasms, computed tomography can be noted.
Hyperplastic polyps are usually small growths about 5 cm in size that rise above the mucous membrane of the colon. They have a soft consistency and are characterized by a normal color.
It is characteristic of adenomatous polyps that they can reach sizes of up to 2-3 cm, be pedunculated or broad-based. Their color is similar to the intestinal mucosa, but their consistency is denser.
Adenopapillomatous polyps (glandular-villous) are usually more than 1 cm in size. They have a velvety surface, which can sometimes be finely lobed. Such polyps can erode and bleed.
Diagnosis of endometrial polyps
In order to clarify the presence and type of polyp, it is necessary to undergo an external examination:
- ultrasound examination of the pelvic organs - makes it possible to detect fibrous and glandular-fibrous polyps;
- hysteroscopy is the best diagnostic method, which also allows removal of the tumor;
- histological examination of scrapings (histology of endometrial polyps) - allows you to determine the structure of the polyp.
Ultrasound signs of an endometrial polyp are quite typical, but a final diagnosis cannot be made. During examination, varying degrees of expansion of the uterine cavity can be detected. Inside, neoplasms of a homogeneous structure with clear contours are found. To clarify the diagnosis of endometrial polyp, hysteroscopy is necessary. It is carried out using a system with special optics, which is inserted into the uterine cavity. Neoplasms are located mainly in the area of the fundus and corners of the uterine cavity. Hysteroscopy can also be used to remove endometrial polyps. After this, it is imperative to conduct a histological examination, since approximately 0.7% of polyps have signs of malignant degeneration.
Why are endometrial polyps dangerous?
In this article we will look at the two most commonly diagnosed forms of the disease: adenomatous polyp and glandular polyp, presented in the form of glands and stromas.
The appearance of any polyps is considered to be a disease that should be treated, especially if the growth becomes permanent and widespread. Even if the neoplasms are benign, this condition is diagnosed as precancerous. For women who are still planning to have children, this disease is especially dangerous, as it often leads to infertility.
- Adenomatous polyp.
It is a type of adenoma that manifests itself in the proliferation of endometrial tissue. The endometrium is the mucous membrane that covers the inner surface of the uterus (during menstruation, the functional layers of the endometrium come out in the form of bloody clots that are dark in color).
Adenoma is essentially a benign tumor, and it appears only in organs that have glandular epithelium. The danger of not treating it is as follows: in most cases, this disease leads the patient to oncology - cancer; this risk increases if you do not consult a specialist in a timely manner. An adenomatous polyp can appear on other organs, but its occurrence in the uterine cavity is most dangerous for a woman’s life.
- Glandular polyp.
Already from the name itself you can understand that this type of polyp is formed from glands and endometrial tissue. These polyps are recognized as the smallest and safest among similar neoplasms. The diameter of a glandular polyp can only rarely exceed 1.5 cm.
Such formations are almost never malignant, although medicine knows of cases where endometrial cancer developed due to glandular polyps. In some cases, the lumen of the glands forms cysts, then we are talking about a glandular-cystic polyp. Glandular cystic polyp is not a separate type. Typically, such polyps appear in the form of a node and are located in the stroma of the mucous membrane, which, in turn, is located in the places where the fallopian tubes drain.
Surgery to remove endometrial polyp
The operation to remove an endometrial polyp is technically simple and does not take much time. The intervention is carried out using general anesthesia. The patient's uterine cavity is scraped out, polyps and the endometrial layer are removed. The polyps are sent for histology, and the patient is prescribed care and rehabilitation therapy. Pregnancy after surgery is possible – both after IVF and during natural conception.
Removal of endometrial polyp by hysteroscopy
Hysteroscopy for uterine endometrial polyp is not only a diagnostic, but also a therapeutic procedure - a minimally invasive surgical intervention. It is performed during an examination, when a thin optical instrument is inserted into the uterine cavity and the condition of the endometrium is determined. Hysteroscopy also involves taking bioptic material from altered areas of the inner lining of the uterus or curettage of an endometrial polyp. As a rule, a simple diagnostic hysteroscopy of an endometrial polyp is performed without anesthesia and lasts from 5 to 20 minutes.
If surgical hysteroscopy is performed to remove an endometrial polyp, then a hysteroscope with a micro-instrument in a tube is inserted into the uterine cavity. This allows for minor removal operations. Using special microscissors, you can remove a tumor or separate small adhesions in the uterine cavity. This therapeutic hysteroscopy, in contrast to a simple diagnostic one with curettage of the endometrial polyp, allows you to specifically get rid of the pathology inside the uterus. This cannot be done using a conventional curette, as there is a high risk of injury to the inner lining and cervix.
Surgical hysteroscopy or surgery to remove an endometrial polyp can only be performed in large clinics or centers that are authorized to use narcotic analgesics and equipped with resuscitation equipment. After removing the polyp using this method, conservative treatment and observation of the woman’s condition in the hospital lasts for 24 hours.
Hysteroresectoscopy of an endometrial polyp is a full-fledged surgical operation, which is indicated for patients with gross pathology in the uterine cavity, as well as for abnormalities in the development of this organ. During the operation, a special instrument is used, which, under video control, will allow for optimally precise manipulations in the uterine cavity. Hysteroresectoscopy of an endometrial polyp lasts from 30 to 90 minutes. It can only be performed under general anesthesia. After removal of the endometrial polyp in this way, treatment is conservative and the patient is monitored in the hospital for 2-3 days.
Simple and therapeutic hysteroscopy, as well as hysteroresectoscopy for endometrial polyps, is indicated for:
- treatment of fibrous polyp;
- treatment of endometrial glandular polyp;
- treatment of glandular fibrous polyp;
- treatment of adenomatous polyp.
Other treatments for endometrial polyp
When an endometrial polyp should be removed, hysteroscopy is not the only method. In urgent situations or when the size of the tumor is too large, curettage is resorted to. The operation is more traumatic and more likely to cause relapses, which is why it is now rarely used or combined with hysteroscopy.
A more modern technique is laser removal of endometrial polyps. It is used only in some clinics. The operation is indicated for women of childbearing age, since after it the chance of secondary infertility decreases. If an adenomatous endometrial polyp is identified, removal of the uterus, sometimes with appendages, is indicated. This type of neoplasm is mainly typical for older women, so the operation does not affect fertility.
When should I get tested for Adenomatous polyposis coli APC: Glu1317Gln (E1317Q)?
- identification of predisposition to adenomatous polyposis of the colon
- familial adenomatous polyposis
If a family mutation is known, family members at increased risk are usually offered predictive genetic testing in early adolescence.
It is recommended to study all known polymorphisms of this gene:
- APC: 1309Del5
- APC: Ile1307Lys (I1307K)
- APC: Glu1317Gln (E1317Q)
- APC: 1061Del5
Treatment after endometrial polyp removal
If surgery to remove an endometrial polyp was performed by hysteroscopy or laser, the risk of complications is minimal. But in the first three days, patients are advised to take no-shpa three times a day. The fact is that after the intervention, spasm of the muscles and neck may occur, which leads to the accumulation of blood in the cavity of the organ. No-spa allows you to relax the muscles and prevents this phenomenon. Short-term antibiotics and anti-inflammatory drugs are also prescribed in the postoperative period.
If an endometrial polyp, its symptoms arose due to hormonal imbalances, combined oral contraceptives may be prescribed as regulators. Women who do not plan to become pregnant in the coming years are recommended to have an intrauterine device installed, which releases gestagen. Hormonal therapy is mandatory for adenomatous polyps in young women if the uterus has not been removed.
Adenomatous polyps
Precancerous diseases of the colon can become malignant, i.e. transform into a malignant tumor. The most common precancers are adenomatous polyps and hereditary polyposis.
Adenomatous polyps have malignant potential. Typically, about 10 years pass from the moment a polyp appears until cancer develops in it. The likelihood of developing an adenomatous polyp increases with age. Half of people over 80 years old have adenomas, most often they are located in the sigmoid and rectum.
There are three types of adenomas:
— Tubular adenoma is usually pedunculated, so the tumor can be removed during colonoscopy. Of all adenomas, it has the lowest risk of malignant transformation, especially if its size is less than 2 cm.
— Villous adenoma does not have a stalk and is located on a broad base directly on the intestinal mucosa, which is why in some cases it is necessary to remove the polyp along with part of the intestine. Often malignant.
— Tubulovillous adenoma has features of both tubular and villous adenoma.
Symptoms of adenomatous polyps are bleeding from the rectum, anemia, blood in the stool, diarrhea or constipation, abdominal pain, prolapse of the polyp along with the mucous membrane from the anus, intestinal obstruction (for large polyps).
Diagnostic measures for adenomatous polyps and intestinal polyps include digital examination of the rectum, X-ray contrast study with barium, fecal occult blood test, sigmoidoscopy, colonoscopy.
During colonoscopy, detected polyps are removed and sent for histological examination. If cancer is detected in a polyp, a second operation is performed in which part of the intestine is removed. In addition, such an operation is performed for flat polyps (usually villous adenomas), the removal of which, due to their connection with the intestinal wall, by other means can be difficult.
Hereditary syndromes of colon polyposis
With some hereditary syndromes, a very large number of polyps can develop in the intestine. Such syndromes (polyposis) significantly increase the risk of developing colon cancer in humans, so these syndromes are classified as precancerous conditions.
Hereditary polyposis syndromes include:
· Familial adenomatous polyposis, in which hundreds and thousands of polyps are present in the mucous membrane from childhood and adolescence, which without treatment necessarily transform into a malignant tumor.
· Hereditary nonpolyposis colorectal cancer is characterized by fewer polyps. A person with this syndrome has a 70-80% lifetime risk of developing colorectal cancer.
Diagnostic measures, in addition to those listed above, for hereditary polyposis include genetic counseling.
Treatment for familial adenomatous polyposis (which, if left untreated, leads to cancer in 100% of cases by age 40) involves early removal of the colon. This usually occurs between the ages of 15-20 years.
With partial removal of the colon or with complete removal of the colon, there is still a risk of malignancy of polyps in the remaining rectum, so regular examination (colonoscopy, sigmoidoscopy) with the removal of all newly formed polyps is very important. When the colon and rectum are completely removed, an ileostomy is formed (an artificial exit of the small intestine onto the surface of the abdominal wall), but the risk of developing cancer in this case is significantly lower.
In case of hereditary non-polyposis colorectal cancer, prophylactic removal of part (as a rule, with this hereditary syndrome, tumors arise in the right parts of the intestine) or the entire colon is also carried out. In addition, patients with this syndrome have an increased risk of developing cancer of the stomach, small intestine, liver, pancreas, kidney, brain tumors, and in women - cancer of the uterus and ovaries.
Treatment with folk remedies
Traditional treatment can sometimes be a fairly rational solution, because alternative methods sometimes turn out to be very effective. Among the folk remedies for the treatment of endometrial polyps, garlic pulp is used, which is placed in gauze, a tampon is made with a long string and inserted into the vagina overnight. The course of folk treatment with garlic is 4 weeks.
Egg yolks and pumpkin seeds are also used. This folk method of treating endometrial polyps has been effectively used for decades. You need to take 6 chicken eggs, boil them, separate the yolks. Add 5 tablespoons of crushed pumpkin seeds and pour in 0.5 liters of sunflower oil. Heat this mass in a water bath and cool. You need to take one teaspoon orally in the morning and evening for 5 days. Then take a break for 1 week and repeat the 5-day course again.
These traditional methods of treatment, as a rule, do not produce any side effects, but may not always be effective.