Alkalis
Unfortunately, alkalis are tasteless and practically odorless, which makes their accidental use more likely. Burns of the oral cavity are typical for the use of alkali, but their absence in no way indicates the absence of damage to the esophagus; in 25% of cases, in children with no pathology in the oral cavity, severe damage to the esophagus was observed after consuming alkalis. The stomach is affected in 20-25% of cases. When exposed to alkali on the esophageal mucosa, liquefaction necrosis occurs, quickly spreading to the underlying layers until the alkali is neutralized by tissue fluid. Accordingly, the higher the alkali concentration, the deeper the damage it causes, even to the point of perforation. There are three stages of the effect of alkali on the esophagus: the stage of liquefaction necrosis, the stage of repair and the stage of scarring. Reparation begins on day 5-6 and can last up to 2-3 or more weeks. During this phase, the scab is rejected, granulation tissue appears, and re-epithelialization occurs. Massive deposition of collagen in the third phase leads to the formation of scar strictures.
Symptoms
Symptoms of a burn to the esophagus depend on what caused the damage to the organ and how severe the inflammatory process is. Much also depends on the age of the victim (children endure chemical burns especially difficult), the presence of chronic diseases, and the individual characteristics of the body.
The main symptoms observed in most cases are:
- severe pain in the larynx, chest, stomach;
- damage to the oral cavity: redness, swelling, often affecting the lips;
- shortness of breath, suffocation;
- lack of voice, hoarseness;
- increased heart rate, lightheadedness;
- weakness, nausea, vomiting (often vomit contains blood and mucus).
It is especially difficult to diagnose a burn in children who have swallowed a chemical liquid without the knowledge of their parents. It is important to question your child to determine what the problem is as quickly as possible. In any case, if you suspect a burn to the esophagus, you must immediately call an ambulance.
Clinic
The clinical picture is dominated by the following symptoms: pain (retrosternal or epigastric), difficulty breathing, drooling, dysphagia, refusal to take fluids, vomiting. The clinical picture does not always predict the degree of damage to the esophagus. One study examining the correlation between the severity of esophagitis and the presence of three symptoms: nausea, drooling and difficulty breathing found that in the absence of all three symptoms, as well as in the presence of only one of them, there was no significant damage to the esophagus, whereas a combination of two symptoms has always been associated with severe damage.
First aid
Before specialists arrive, it is necessary to provide the victim with all possible first aid. The principles of its implementation are effective for both chemical and thermal burns. The first thing to do is rinse the stomach. It is necessary to give the victim water to drink, preferably with potassium permanganate (add a few crystals to 1 liter of water). The sooner a person vomits out the remaining toxins, the less harm they will have time to cause.
If drinking water does not help, you can speed up the gag reflex by inserting two fingers into your mouth.
After gastric lavage, it is necessary to neutralize the effect of the substance taken. The basic rule is related to the properties of acids and alkalis: one neutralizes the other. If the victim has damaged the esophagus with vinegar essence or any other acid, it is necessary to take a soda solution. To do this, dissolve half a teaspoon of baking soda in a glass of water at room temperature.
If alkali enters the body and causes a burn, you must take acid. The easiest way is to squeeze the juice of half a lemon into a glass of water at room temperature. You can alleviate the pain by taking a little warm milk.
If the cause of the burn is unknown or you are not confident in your knowledge, it is better to do only gastric lavage. Improperly neutralizing the aggressive substance that has affected the esophagus can aggravate the inflammatory process.
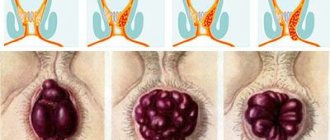
Classification
We use the following classification of caustic injuries of the esophagus:
- 0 - no damage
- 1 - erythema and swelling
- 2 - ulceration is not circular
- 3 - circular ulceration
- 4 - perforation
There are also more detailed classifications:
- 1st degree - erythema and edema (damage is limited to the superficial layers of the mucosa, their rejection with subsequent epithelization without scar formation is possible).
- 2a degree - vulnerability, hemorrhages, erosions, exudate, blistering (mucosal, submucosal and muscular layers are involved).
- 2b degree - the same as 2a plus deep or circular ulcers.
- Grade 3a - deep ulcers, “gray or black esophagus” (transmural lesion).
- Grade 3 - extensive necrosis.
Related articles:
- Articles: ENDODIAGNOSTICS FOR ESOPHAGUS BURNS WITH ALKALI
- Articles: FEDERAL CLINICAL GUIDELINES “Toxic effect of corrosive substances”, “Toxic effect of soaps and detergents” 2014
- Articles: Zargar classification - assessment of damage to the esophagus when swallowing caustic (caustic) substances
CLASSIFICATIONS section
Complications
Thermal burns are often accompanied by complications, which are usually classified into primary, secondary and late.
- Primary complications resulting from injury are typical only for 4th degree burns. These include charring and mummification of soft tissues, thrombosis of large arteries and veins.
- Secondary complications often arise due to infection and can affect the skin, soft tissues, blood vessels and nerves, and internal organs. These include gangrene, abscesses, hepatitis, osteomyelitis, etc.
- Late complications develop during or after healing of burn wounds. These are pyelonephritis, hepatitis, dysfunction of joints and limbs, in some cases burn dermatitis and eczema.
Local complications of thermal burns include the formation of scabs, contractures and scars. A scab is a hard, necrotic tissue that encircles the limbs, neck or torso, the so-called circular scab. The scab puts pressure on the tissue, causing ischemia - a local disruption of blood flow, which can cause breathing problems. Scars and contractures form with high-grade burns and can lead to limited joint mobility. Do not self-medicate, be sure to consult your doctor.
When to perform endoscopic examination?
Initial endoscopic examination should be performed within the first 2-3 days after injury. Contraindications to it are: shock, respiratory disorders, perforation, mediastinitis.
In the period from 5 days to 3 weeks, during the repair stage, the wall of the esophagus is thinnest and the risk of perforation during endoscopy is very high, therefore, it is highly undesirable to perform it at this time. After three weeks, dense fibrous tissue usually forms and endoscopy becomes safer. In addition to endoscopic examination, radiography of the chest and abdominal cavity, clinical blood test, urea, and liver tests are indicated.
Types of esophageal burns
Depending on the factors that provoke damage to the walls of the esophagus, several types of burns are distinguished; they are shown in the table below.
| Chemical | It is provoked by the use of certain chemicals. This happens either deliberately, as an attempt at suicide, or by accident. Often adults and children burn themselves with vinegar, an affordable product available in every kitchen. |
| Thermal | Caused by consuming excessively hot food and drinks. The consequences affect both the stomach and esophagus: the mucous membranes of both organs are affected. This condition is especially dangerous for patients with ulcers and other chronic diseases of the digestive system. |
| Ray | It is rare, the main cause is a complication after radiation therapy performed to treat malignant tumors. |
Some experts classify alcohol burns as a separate group, which occurs due to drinking large quantities of alcohol or low-quality drinks. This problem occurs not only among people with an immoral lifestyle; to get a burn, it may be enough to drink a cheap, low-quality alcoholic drink once.
Treatment and prognosis
The prognosis is largely determined by the amount of damage. Thus, two independent studies carried out in the 70s of the last century showed that with 0-1 degrees of damage, the probability of stricture formation is 0, with 2 degrees it reaches 17-23%, and with 3 degrees - 100%. More recent data also suggest that acute mortality and the rate of stricture formation in stages 1-2a are minimal, burns 2b-3a lead to strictures in 70-100% of cases, and grade 3b is associated with a mortality rate of 65%. The pH of the product also plays an important role; if it is more than 12.5 or less than 2.0, the likelihood of severe damage is very high.
Treatment of caustic lesions of the esophagus is difficult; they are easier to prevent than to treat. First of all, it is necessary to establish the type of caustic agent. At the pre-hospital stage, treatment should be aimed at maintaining vital functions. Previously recommended attempts to neutralize the caustic agent with weak acids (in the case of alkalis) and weak alkalis (in the case of acids) are now considered harmful because increased heat generation from the chemical reaction can further damage the tissue. In addition, the experiment proved that a 3.8% alkali solution affects the mucous and submucosal layer within 10 seconds after administration (a higher concentration of alkali over approximately the same period of time damages the muscle layer), which makes neutralization attempts pointless. The only exception is the use of 200-250 ml of water or milk within 30 minutes of consuming alkali granules, but even then the risk of vomiting must be taken into account. Attempts to “dilute” the acid with water are contraindicated because lead to increased heat generation as a result of a chemical reaction. Emetics are also contraindicated because lead to repeated exposure of the agent to the esophageal mucosa. You can allow the patient to rinse his mouth with water (spitting it out).
It is extremely important to start eating as quickly as possible. Patients with grade 1-2a lesions begin to be fed within the first 24 hours (of course, the food should not be coarse, hot or cold). In patients with more severe damage, observation for 48 hours is necessary to rule out perforation, then feeding can be started cautiously. If the esophagus is damaged at grade 2b-3 during endoscopy, it is reasonable to leave a nasogastric tube for enteral nutrition (but no more than 2 weeks). The same probe can be useful for passing a string to bougienage the resulting strictures of the esophagus. To reduce chest pain (in patients who can take liquids), you can use liquid agents containing anesthetics, for example Almagel A. Despite the fact that there are studies showing a decrease in the formation of post-burn strictures of the esophagus with the use of hormones, they are currently not widely used due to with the risk of developing infectious complications. If hormones are used, their doses vary from 1 to 2 mg/kg per day, and treatment should begin no later than 48 (and preferably 24 hours) after the burn, with gradual withdrawal of the drug over 2 months. Antibiotic therapy with broad-spectrum drugs when using hormones is mandatory. After dilatation of strictures, the use of steroids is justified, as it leads to a decrease in the number of their relapses. Sometimes recommended antisecretory therapy with proton pump blockers and H2 blockers is of questionable effectiveness. We will not dwell on the surgical treatment of this pathology.
Clinical picture
First, ENT patients experience a burning sensation in the throat, mouth and esophagus.
Then moderate pain occurs, which intensifies when swallowing. Pain can occur behind the sternum, in the back and in the epigastric region. After some time, dysphagia (disorder of swallowing function) occurs, salivation increases (hypersalivation), and vomiting mixed with blood. Patients experience severe thirst, hoarseness, increased blood pressure and body temperature. Serious disorders also occur in the body, such as:
- Shock;
- Collapse (acute vascular insufficiency);
- Intravascular hemolysis (massive bleeding and blood clotting);
- Structural and functional damage to the kidneys and liver;
- Metabolic disease;
- The central and peripheral links of the nervous regulation of the esophagus are damaged, which contributes to the occurrence of spasm and narrowing of the lumen of the esophagus.
The patient's blood pressure drops, he turns pale, and there is a decrease in heart rate. As a consequence of acute vascular insufficiency and shock, death can occur. Perforation of the esophagus or stomach is possible, which can be complicated by other diseases. Edema of the larynx may also develop, which will require tracheotomy (dissection of the anterior wall of the trachea), as well as severe intoxication (renal failure).
Friends! Timely and correct treatment will ensure you a speedy recovery!
If the course of the disease is favorable, 10-15 days after receiving a burn, pain when swallowing significantly decreases or completely disappears. The patency of the esophagus is restored, the temperature returns to normal and, as a result, the general condition of the patient significantly improves. But if you do not carry out treatment, then after 1-2 months signs of narrowing of the esophagus will appear.