The article was checked by gastroenterologist and endoscopist Kondrashova E.A. , is for general informational purposes only and does not replace specialist advice. For recommendations on diagnosis and treatment, consultation with a doctor is necessary.
Polyps are benign neoplasms - growths of normal tissues of the body. They are found in organ cavities and may externally resemble cauliflower, thickenings on a stalk or papillae. There are both single and multiple growths; the severity of the disease is related to their number and volume. Some types can develop into malignant tumors over time, which is why removal of polyps in the stomach is often the preferred method of treatment.
The stomach is lined from the inside with a special mucosal epithelium - a cellular layer that is resistant to the action of hydrochloric acid, which is contained in gastric juice, as well as to the mechanical effects of food. It is the epithelium, which takes the brunt of all harmful compounds from food, that with prolonged injury can grow and form a polyp. Depending on the type of cells responsible for the formation of the polyp body, they are divided into types: hyperplastic, adenomatous, fundic glands and others. The type of polyp is determined using histological examination to determine whether it is prone to degeneration into a malignant tumor.
Make an appointment with a gastroenterologist
Symptoms of the disease
Sometimes polyposis occurs unnoticed by a person and is discovered by chance during an endoscopic examination of the gastrointestinal tract. However, large polyps in the stomach most often cause symptoms. The main ones include:
- Soreness and cramping in the upper abdomen, especially in the left and center;
- Repeated vomiting after eating or taking medications;
- Nausea;
- Increased salivation;
- Long-term severe loss of appetite, weight loss;
- Vomiting mixed with blood and black feces are the most dangerous signs indicating bleeding from injured polyps.
Causes of the disease
The causes of the disease include all damaging factors affecting the gastric mucosa:
- Helicobacter pylori infection (bacterium H. pylori);
- Chronic gastritis, especially with high acidity;
- Peptic ulcer;
- Excessively long-term use of proton pump inhibitor drugs (Omeprazole, Pantoprazole);
- Hereditary predisposition;
- Abuse of alcohol, spicy foods;
- Smoking.
Some of these factors provoke the development of polyps of a specific type: Helicobacter pylori infection leads to hyperplastic ones, excessively long-term use of Omeprazole leads to polyps of the fundic glands.
The severity of the disease depends on the number of tumors, their size and location in the stomach. Multiple or large ones can interfere with the normal passage of food; their constant trauma can lead to the appearance of dysplasia - this is the first step in the degeneration of body tissue into malignant. The greatest danger in terms of oncology is adenomatous and some types of hyperplastic.
Sign up for a consultation
Polyps of the gastrointestinal tract
Recently, all over the world, including in Belarus, there has been an increase in the number of patients with polyps of the gastrointestinal tract (GIT). This is due, on the one hand, to a certain absolute increase in this pathology in adults and children, and on the other hand, to the rapid development of endoscopy, which is the main reliable method for diagnosing this disease. Polyps occupy a significant place among various diseases of the gastrointestinal tract and in a large percentage of cases undergo malignancy. The lack of reliable clinical criteria, characteristic only for polyps of the gastrointestinal tract, puts practitioners in a difficult position when making a diagnosis and conducting differential diagnostics, as well as treatment tactics, choosing the method and volume of surgical intervention, depending on the location, prevalence and morphological structure of the polyps .
What are gastrointestinal polyps?
Polyp is any formation on the mucous membrane that protrudes into the lumen of a hollow organ and is connected to its wall by a stalk or a wide base. The frequency of localization of polyps in different parts of the gastrointestinal tract varies; most often they are localized in the stomach, then in the rectum and colon, less often in the esophagus, duodenum and small intestine.
Esophagus:
Benign tumors of the esophagus are rare, somewhat more common in men and middle-aged people. In relation to esophageal cancer, they account for 6.2%. They most often develop in places of natural narrowing and in the lower third of the esophagus.
What are the types of benign esophageal tumors?
There are two types of benign tumors - epithelial ( polyps, adenomas, epithelial cysts ) and non-epithelial (leiomyomas, fibromas, neuromas, hemangiomas, etc.), which are much more common. Polyps and adenomas can be localized at any level of the esophagus, but more often they are located at the proximal end or in the abdominal region. These tumors may have a broad base or a long stalk. In the latter case, they sometimes become pinched in the area of the cardia or fall out of the esophagus into the pharynx, causing corresponding symptoms. These are usually well-circumscribed, reddish, sometimes lobular tumors. When the vessels are located superficially, they bleed easily when touched. These formations should not be confused with the more common papillomatous growths on the mucous membrane of the esophagus, which occur in older people due to chronic inflammatory changes. Such papillomas do not reach large sizes.
Stomach:
Epithelial and non-epithelial benign tumors occur in the stomach. Epithelial benign tumors ( polyps and polyposis ). Gastric polyps account for 5-10% of all stomach tumors and are more common in people aged 40-50 years. Men get sick 2-4 times more often than women. The question of the possibility of a gastric polyp turning into cancer is confirmed by numerous observations of clinicians and pathologists. More often, malignant transformation (malignization) of a polyp begins from the base. A wide base, cartilaginous consistency, and the presence of ulceration in the center or at the base are characteristic macroscopic signs of polyp malignancy. Gastric polyps are localized (in approximately 80%) mainly in the antrum, but can also develop in other parts. In the area of the cardia, polyps are extremely rare. The size and appearance of polyps vary, but most often they appear as a mushroom, papilloma, or cauliflower. It is necessary to distinguish between a pedunculated and broad-based polyp; the latter form should be alarming in terms of malignancy, especially if the polyp has reached a significant size. Polyps can be single or multiple. If several polyps form within one segment of the organ - multiple polyps, if in two or more segments - polyposis.
duodenum:
Benign tumors of the duodenum are extremely rare. Most often, polyps are observed, then leiomyomas, very rarely - neuromas, as well as lipomas, fibromas, lymphangiomas and hemangiomas.
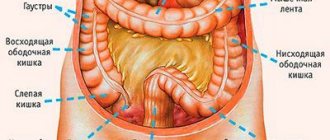
Colon:
Benign colon tumors can arise from any of the non-epithelial and epithelial tissues that make up the intestinal wall. Epithelial tumors originate from the glandular epithelium and have the appearance of individual or multiple polyps, sometimes occupying large areas of the colon. Single polyps are 3 times more common than multiple ones. A villous tumor, representing multiple papillary growths of the mucous membrane, it can either look like a separate tumor node or line the intestinal wall over a fairly extensive area. With varying frequencies (from 10 to 60% according to various statistics), a villous tumor gives rise to malignant growth, which is why knowledge of its clinical features is of great practical importance.
Reasons for the formation of polyps
There is still no generally accepted theory of the etiology of the occurrence of polyps and polyposis. There are several theories about the occurrence of polyps:
- Inflammatory theory;
- Theory of embryonic ectopia;
- Disregenerative theory;
However, there is no consensus among scientists on the nature of this disease.
Clinical manifestations of gastrointestinal polyps
The lack of reliable clinical criteria, characteristic only for polyps of the gastrointestinal tract, puts practitioners in a difficult position when making a diagnosis and conducting differential diagnostics, as well as treatment tactics, choosing the method and volume of surgical intervention, depending on the location, prevalence and morphological structure of the polyps . However, there are still certain symptoms depending on the location, size and effect on the body.
Esophagus:
Small benign tumors of the esophagus are quite common. They do not cause clinical manifestations and are often unexpectedly discovered during endoscopic examination. The disease manifests itself with the onset of dysphagia. Benign tumors rarely cause esophageal obstruction. Dysphagia was observed in only 50% of patients. With large tumors, in addition to dysphagia, patients experience a sensation of a foreign body in the esophagus, vomiting and nausea, and sometimes pain when eating. It happens that large tumors do not cause any symptoms and are accidentally detected during X-ray or endoscopic examination. Unlike esophageal cancer, dysphagia with polyps does not tend to steadily and rapidly increase and can remain unchanged for several months or even years. In the anamnesis of some patients, periods of improvement in the passage of food due to a decrease in spasms are noted. The course of polyps depends on the morphological structure and growth rate. With rapid growth of the polyp, rapid malignancy is possible, especially at a young age. The general condition of patients with esophageal polyps does not suffer. Sometimes there is some weight loss due to eating disorders and natural anxiety in such cases.
Stomach:
It is possible that polyps may exist without clinical symptoms; in such cases they are an incidental finding during X-ray or endoscopic examination. Painful symptoms, often observed with gastric polyps, are largely determined by the severity of the inflammatory phenomena against which the polyp exists. In most cases, pain is localized in the epigastric region, initially associated with food intake, and then becomes independent of food intake. If the polyps block the exit from the stomach, the patient vomits. Polyps that have a long stalk can prolapse into the duodenum and become pinched in the pylorus, causing attacks of sharp cramping pain in the epigastric region with irradiation throughout the abdomen. Patients complain of a bitter taste in the mouth, nausea, and belching. Appetite does not suffer. If these symptoms are mild, patients may not see a doctor for years. When the polyp is ulcerated, moderate gastric bleeding is observed (a positive reaction to hidden blood in the stool), and in more severe cases, blood is detected in the vomit and tarry stool. The usual signs of blood loss may occur: weakness, pallor of the skin, secondary hypochromic anemia. Malignization of the polyp occurs gradually: loss of appetite, general weakness, weight loss are noted, i.e. signs characteristic of stomach cancer develop. It should be noted that the beginning of the transition of a polyp to cancer cannot be detected either clinically or radiologically. Therefore, patients who have been diagnosed with gastric polyps should be under systematic dynamic supervision by an endoscopist; at the slightest suspicion of malignant transformation of the polyp, the patient should be subjected to surgical treatment.
Colon:
The clinical picture depends on the number, location and morphological structure of polyps. With single polyps there may be no complaints for a long time. With multiple polyps and polyposis, an asymptomatic course does not occur. Polyposis is manifested by pain along the colon, frequent, often painful stools mixed with blood, mucus, and pus. With polyps located in the distal parts of the colon, tenesmus is often observed, and when combined with rectal polyps, discomfort, pain, and itching in the anus. If the presence of a single polyp worries patients little, then with multiple polyposis the disease is accompanied by bleeding during and after bowel movements, diarrhea, leading to dehydration, intoxication and anemia.
Diagnosis of gastrointestinal polyps.
The main diagnostic method is endoscopic examination, which allows one to determine the location, size, shape of the polyp, and also perform a targeted biopsy. In addition, endoscopic examination makes it possible to resolve issues of further patient management tactics.
Treatment of gastrointestinal polyps.
The main method of treating gastrointestinal polyps is endoscopic polypectomy (a minimally invasive operation performed without opening cavities).
Methods of polypectomy:
- Excision;
- Electroexcision;
- Electrocoagulation;
- Photocoagulation;
- Medical polypectomy;
- A combination of several methods;
The decision on the method of polypectomy is made by the endoscopist depending on the location, shape, size of the polyp, the results of a morphological study, as well as in accordance with the available equipment and qualifications of the endoscopist.
Polyps measuring less than 5 millimeters are subject to dynamic endoscopic monitoring once every 6 months. Polyps larger than 4 centimeters in size, if endoscopic removal is impossible, are subject to surgical treatment.
Endoscopic polypectomy is performed in the endoscopic departments of surgical hospitals as part of one-day minimally invasive surgery.
After endoscopic polypectomy, control endoscopic examinations are required at 1, 3, 6 and 12 months and then once a year for life.
Head endoscopic department A.E. Danovich
Diagnostic methods
- Fibrogastroduodenoscopy
(FGDS) is the main method for diagnosing the disease; it allows not only to detect neoplasms, determine their shape and quantity, but also to perform a tissue biopsy for subsequent research. During the procedure, the doctor examines not only the stomach cavity, but also the esophagus and upper intestine. Additionally, FGDS allows you to take material to detect Helicobacter pylori infection in order to determine the degree of infection of the mucous bacterium H. pylori. - Histological examination
allows us to determine the type of polyp and its tendency to degenerate into a malignant tumor. It is carried out both after a preliminary biopsy and to study an already removed tumor. - Radiography with a contrast agent
(barium sulfate) is an important method in determining the shape and exact size of polyps, the degree of lumen overlap in various parts of the stomach. - Ultrasound examination of the abdominal organs is an auxiliary method that allows you to determine the size of polyps and identify concomitant pathologies. At the Yauza Clinical Hospital, endoscopic ultrasound is performed using a Hitachi Preirus device, which significantly increases the accuracy of diagnosis.
- Fecal occult blood analysis
makes it possible to detect even slight bleeding from damaged tissues.
At the Yauza Clinical Hospital, the ERK-17000 video processor is used to diagnose polyps of the stomach and intestines, which significantly improves the quality and accuracy of the study.
Introduction
Gastric polyps (GPS) are benign tumors of the stomach. This is a fairly common pathology, detected in 1-6% of gastrointestinal endoscopy results and in 0.1-0.8% of autopsy results [1]. The pancreas may not be accompanied by pain or dyspeptic syndromes and is detected during esophagogastroduodenoscopy (EGDS), performed during examination in connection with other diseases or during preventive examinations. The relevance of the study of pancreas is also given by the uncertainty of the prognosis with the possibility of malignancy [2]. There is no standard for the quality of medical care for patients with pancreas in Russia; the main method of treatment is endoscopic polypectomy followed by histological verification of the formation. In addition, as a drug therapy for patients with pancreas and gastric dyspepsia, proton pump inhibitors (PPIs) are often empirically prescribed without studying the level of intragastric acidity.
It has been proven that the risk of developing pancreas increases with increasing degree of atrophy of the gastric mucosa, especially when the body of the stomach is damaged [3]. However, there is very little data in the literature on the results of studying the acid-forming function of the stomach in pancreas. Currently, 24-hour intragastric pH-metry has almost completely replaced fractional sounding and is considered the optimal method for assessing the level of acidity in the stomach and esophagus [4].
The purpose of the study was to study the characteristics of the level of daily intragastric acidity in patients with pancreas.
Treatment of stomach polyps at the Yauza Clinical Hospital
The effectiveness of treatment for gastric polyposis is directly dependent on the quality of diagnosis and correct interpretation of the results of clinical, laboratory and instrumental methods of examining the patient.
The Department of Gastroenterology is equipped with foreign equipment unique to Moscow in order to accurately diagnose polyps in the stomach. Treatment can be either conservative or with surgery, depending on the severity of the patient’s condition, the location, size and histology of the polyps. Experienced gastroenterologists will give recommendations not only on drug therapy, but will also develop an individual diet that will help prevent the appearance of new polyps after surgery or eliminate the symptoms of the disease in those patients for whom polypectomy is not indicated.
Polypectomy methods in most cases achieve complete cure, but relapses of polyps may occur, requiring repeated interventions.
The price of treatment depends on the volume of necessary diagnostic studies and consultations of related specialists. The estimated cost of removing stomach polyps can be clarified by phone.
Make an appointment
results
According to a survey of patients, the most common complaint was epigastric pain - in 52 (86.7%) of the subjects. At the same time, 12 (20%) patients experienced pain soon after eating; 40 (66.6%) people did not note a connection between pain and food intake. “Hungry” and night pain, characteristic of hyperacid conditions, were practically not recorded.
A significant number of patients noted heaviness and fullness in the epigastrium - 26 (43.3%). At the same time, some patients limited portions of food, trying to avoid unpleasant sensations.
Nausea was significantly more common than vomiting, in 28 (46.7%) and 5 (8.3%) patients, respectively. A bitter taste in the mouth was noted by 8 (13.3%), and a sour taste by 9 (15%) patients, and belching of air by 23 (38.3%) patients.
31 (51.7%) patients complained of heartburn. In 11 (18.3%) patients, a decrease in appetite was noted. In addition, 7 (11.7%) patients noted significant (more than 5 kg over the previous six months) weight loss. A tendency to constipation was detected in 4 (6.7%) patients, and to diarrhea - in 19 (31.7%). In 37 (61.7%) patients, stool was predominantly daily, formed.
The duration of the anamnesis, that is, the time since the first detection of the pancreas, varied from 1 to 19 years, averaging 5.2 ± 0.68 years. During observation by a physician (gastroenterologist) regarding the pancreas, 58 (96.7%) patients, either prescribed by a doctor or independently, underwent a course of PPI treatment; another 2 patients independently took only H2-histamine blockers without determining the acid-producing function of the stomach (Table 1)
Table 1. Taking antisecretory drugs in patients with gastric polyps.
Note. PPIs—proton pump inhibitors; * — the difference between groups is statistically significant (рχ2<0.05).
. Antispasmodics, prokinetics, and enzyme preparations were prescribed to 60 (100%) patients.
About 30% of all those examined received long-term courses of antisecretory drugs in full doses as prescribed by a doctor. When taken independently, short courses and half doses predominated. At the same time, 13.3% of patients independently took PPIs in combination with H2-histamine blockers.
Only 31 (51.7%) patients were examined for Helicobacter pylori infection at the outpatient stage, 22 (36.7%) received eradication therapy (without monitoring the effectiveness of eradication). When examined at the time of inclusion in the study, 17 (28.3%) patients with pancreas were Helicobacter pylori-positive, which is lower than population values.
During endoscopy, catarrhal distal esophagitis was detected in 7 (11.7%) patients; erosive esophagitis was not noted. According to histological examination, in 22 (36.7%) patients the polyps were adenomatous, in 38 (63.3%) they were hyperplastic. According to 24-hour pH measurements, patients with pancreas showed a decrease in intragastric acidity (Table 2)
Table 2. Main indicators of the level of acidity in the stomach in patients with gastric polyps.
Note. *—the difference between day and night for this indicator is statistically significant (p<0.05).
.
The average value of the antral pH level in pancreatic patients corresponded to the indicators of hypoacidity and anacidity. When performing 24-hour intragastric pH-metry, only 14 (23.3%) patients did not experience a decrease in acid-forming function (Table 3) Table 3. Distribution of patients with gastric polyps according to the intensity of basal acid formation.
Note. *—the difference between day and night for this indicator is statistically significant (p<0.05).
.At night, 80% of those examined showed hypo- or anacidity.
Disease prevention
The risk of new polyps will help reduce:
- Timely treatment of gastritis, gastric ulcer. Regular examination by a gastroenterologist for existing chronic diseases of the gastrointestinal tract;
- Elimination of Helicobacter pylori infection: treatment must be under the supervision of a specialist;
- Revision of drug prescriptions in favor of forms of drugs that are safer for the stomach;
- Refusal of self-medication, uncontrolled taking of pills;
- Reducing the amount of alcohol consumed, giving up strong alcoholic drinks, smoking;
- A balanced diet with a predominance of boiled and steamed food, fresh vegetables and fruits. Reducing the amount of hot spices and too hot food.
In the esophagus
The starting material for esophageal polyposis is epithelial cells. Most often, the disease affects middle-aged males. There are several places in the esophagus where outgrowths form especially often - in the area of the gastroesophageal sphincter, in the area of narrowings, on the mucous membrane of the lower part of the esophagus (this area is affected by more damaging factors). They are also characterized by two types of structure, like the others. A pedunculated polyp is dangerous because it can fall into the lumen of the pharynx (if it is close to it) or become pinched in the cardiac region.
Large growths rarely form in the esophagus. As a rule, they are discovered accidentally during research not related to the search for polyps, for example, during fibrogastroscopy. Heredity, concomitant diseases (esophagitis, gastritis, ulcers), and chronic stress predispose to the development of the disease. Injuries from hot and hard foods, alcohol, and cigarette smoke can also affect the formation of outgrowths. The injured area needs healing, and at some point the epithelial cells grow too much.
Symptoms depend on the number of formations, location and size. With large formations, a person feels a lump in the throat, compression in the chest, and heartburn. If the polyp is pinched in any way, pain may occur, especially while eating. As mentioned above, polyps are often discovered by chance - they are usually small in size and grow slowly.
If the formations still go unnoticed and manage to grow, the patient will face complications and serious symptoms, in particular:
- constant painful sensations;
- urge to vomit;
- severe pain when eating;
- loss of appetite;
- weight loss;
- irritability.
Diagnosis and treatment
The disease is diagnosed by one of three methods - examination and history taking, endoscopic examination, x-ray.
The results of the examination and survey allow one to suspect the presence of growths and prescribe appropriate diagnostic measures. Endoscopic examination successfully assesses the condition of the mucosa and is highly likely to detect formations. It allows not only to determine the condition of the mucosa, but also to take a biopsy sample for further examination for signs of malignancy.
If endoscopic examination is impossible for some reason, a decision is made to use radiography with contrast. Thanks to the contrast agent, the walls of the organ and all the protrusions and outgrowths on it are visible in detail.
Treatment, as in other cases, is surgical. It is necessary to start it as quickly as possible in order to avoid ulceration, internal bleeding, and pinching of the polyp, which causes pain. Removal is performed endoscopically using a loop, which cuts off the polyp and immediately “seals” the vessels to prevent bleeding. This method is also suitable for removing multiple polyps. It only takes 1-2 weeks to heal.
During the recovery period, you should consume warm, soft foods, steamed or boiled. You should not take sour, peppery, salty foods, hot or cold foods. Foods with fiber, fatty meat, and some cereals are excluded from the diet. A more detailed consultation on diet is provided by a gastroenterologist.
Removal
A promising method of treating cardia polyps is surgery, but not all surgeons strive to remove tumors at once. If the cardia polyp is single and does not bother you clinically, then a wait-and-see approach can be chosen with monitoring the condition and dynamics of the tumor at least twice a year.
There are three types of surgery for cardial polyps.
Endoscopic correction
Endoscopic manipulations are among the most common and safest methods of removing tumors. The indication for the procedure is a cardia rosette polyp with a diameter of no more than 3.5 cm and no signs of cancer.
Contraindications include:
- presence of a pacemaker,
- complicated clinical history,
- high risks of gastric bleeding,
- some blood diseases.
Before the procedure, patients drink a sodium bicarbonate solution to completely dissolve the mucous component of the stomach.
There are two operational approaches:
- Laparoscopy - punctures in the peritoneum in the projection of the cardia of the stomach and the introduction of endoscopic instruments;
- Endoscopy is the insertion of flexible probes with paths for surgical instruments through the pharynx and esophagus, as during gastroscopy.
Removal is carried out under general anesthesia (anesthesia is used). During endoscopic manipulation, the patient is placed on his left side, with his knees brought to his stomach. During laparoscopy, the patient is placed on his back. A tube with an optical tip and a special loop is inserted into the esophagus. The stalk of the polyp is cut and removed using an endoscope. The resulting polyp is sent for histological examination. The total duration of the operation is 30-60 minutes. The rehabilitation period lasts up to 14 days.
Regular endoscopic examinations and therapeutic manipulations damage the gastric mucosa, which can provoke relapses or intensive growth of small polyps.
Treatment with coagulation
Electrocoagulation is carried out according to the same algorithm as endoscopic polypectomy. The main difference is the use of biopsy forceps with a current function instead of a metal loop.
The method has many advantages, including:
- stopping bleeding,
- reduction of infectious risks,
- availability.
An analogue of coagulation with electric current is electroexcision. During the intervention, a dielectric loop is used.
It is possible to coagulate blood vessels and the wound bed using a laser, but laser removal of cardiac polyps is rarely used due to the complexity of the procedure and multiple limitations.
Abdominal surgery
A radical surgical method is indicated for:
- total polyposis (the number of neoplasms cannot be counted),
- the diameter of the growth is more than 3.5 cm,
- high risks of malignancy of tumor cells.
The operation is performed under general anesthesia. The patient is placed on the operating table, an incision is made along the anterior wall of the peritoneum, and gastric juice is removed. The polypous tissue is scraped off with a scalpel, and the resulting material is sent for histology.
If the result for cancer cells is negative, then the stomach is sutured with self-absorbable threads. If the risks are high or an oncological process occurs, then the damaged part of the stomach is removed within healthy tissue.
The indication for resection is necrotic changes in the mucous membranes.
Postoperative recommendations and rehabilitation
With endoscopic removal methods, the rehabilitation period lasts up to 14-18 days. Abdominal surgery requires a longer recovery.
Among the main medical recommendations are::
- Following a gentle diet (puree-like lean dishes, weak broths);
- Taking enzymes and drugs to restore gastric microflora;
- Elimination of physical activity;
- Medical examinations and monitoring of the condition of the gastric mucosa.
Unfortunately, any operation does not protect against recurrence of gastric cardia polyps.
In almost 2% of all cases, relapse occurs after a few years.
Complications
Complications after removal of polyps of the gastric cardia rosette occur quite rarely and are characterized by the following changes or conditions:
- bleeding (lack of coagulation, intense manipulation of currents);
- perforation of the walls of the esophagus, stomach (incorrect choice of current power, too wide wound bed);
- burn and necrosis of mucous membranes.
Complications after abdominal surgery are more common, up to 25% of cases. Typically, final healing occurs several months after the procedure.
What it is?
Polyps in the stomach are benign tumor-like formations that form from the glandular structure of the mucous membrane of the organ. These tumors appear on the inner wall of the stomach and grow into its lumen. They can have a wide base - sessile tumors and an oblong stalk - lancet tumors. The latter are found at the tops of the mucous membrane, becoming a continuation of its folds.
The shape of the tumor is most often round or oval, although mushroom-shaped and papillary polyps are sometimes found. Their color varies from gray to deep red. The more glandular cells a tumor contains, the softer its consistency will be. The average size of the tumor is 15 mm, although sometimes large tumors reaching 60 mm are found.