The human intestine is usually divided into thick and thin. Each department has its own anatomical features and functions. The large intestine is the final, lower part of the intestine. It got its name for its thicker walls and wider clearance. It consists of several parts, each of which has structural features and plays its own role. You can find out more about the anatomy of the large intestine further.
Features, role and functions of the large intestine
The final part of the intestine is the large intestine.
The large intestine completes the intestines and ends at the anus. Its length in an adult is approximately 2 m. The large intestine, the anatomy of which has its own characteristics, performs important functions in the body:
- Excretory. The main, but not the only function of the intestines is to remove toxins and substances from the body that are unnecessary or harmful to health. This process must be uninterrupted, otherwise the body may be poisoned. A feature of the large intestine is the slow movement of food. The process goes faster after the next meal: food enters the stomach and a signal is sent to the intestinal muscles.
- Digestive. In the large intestine, the process of breaking down food and breaking it down into its components continues. Remains of food, from which all nutrients have already been absorbed into the intestines, are compacted into feces and excreted from the body.
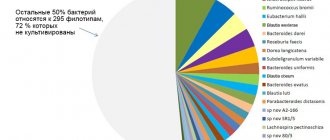
- Protective. As you know, it is in the intestines that the beneficial microflora with bacteria that support the immune system is located. Violation of the microflora leads to a weakening of the body’s protective function and a decrease in its resistance to viruses and pathogenic bacteria.
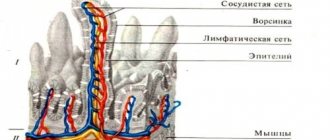
- Suction. The intestinal walls are capable of absorbing water, fatty acids, amino acids, and salts from digested food.
The large intestine is shorter, but also wider than the small intestine. Its length is only 1.5-2 m, while the small part of the intestine is more than twice this size. The diameter of the large intestine is approximately 8 cm. The diameter narrows closer to the anus. The large intestine has a grayer tint and is more heterogeneous than the small intestine. Its uneven muscle layer creates bulges on it; it seems that it consists of cells, swellings with constrictions.
The large intestine also has such features as muscle bands and omental processes. Along its entire length there are thin muscle strips that help peristalsis. On this tape there are accumulations of fat, the so-called omental processes, which protect the intestinal walls from damage. Maintaining colon health is especially valued by yogis, since there are about 500 species of microorganisms here, which significantly exceeds their content in the small intestine.
How long is our intestine?
The small and large intestines are a vital part of the human digestive system.
The length of the small intestine is approximately 274–488 centimeters, while the large intestine is shorter at about 150 centimeters in length. The intestines are located in the stomach and absorb nutrients, vitamins and water. They form part of the gastrointestinal tract (GIT) and are the last section of the digestive system. In general, the intestines run from the end of the stomach to the anus.
Although the intestines can fit inside the abdominal cavity, they are much longer than many people think. The exact length of the intestine may also vary from person to person.
Earlier studies examining intestinal length in people who have donated their bodies to science show that the average total intestinal length is about 8 meters, with a range of 670 to 900 centimeters.
The study authors emphasize that measurements of intestinal length are rare. For this reason, there is no scientific evidence that the size or length of the intestines correlates with health or affects digestive function.
In this article we will discuss what research says about the length of the small and large intestines.
Sections of the large intestine
The sigmoid colon is very important in terms of absorption function.
The large intestine occupies quite a lot of space in the retroperitoneal space. It consists of several departments. They differ in length, width, functions, location:
- Cecum. In appearance it looks like a sac with a small appendage. This part is divided into the cecum itself and the well-known appendix. The cecum is small in size, its diameter rarely exceeds 10 cm. It is difficult to say exactly what role this part of the intestine plays in the digestion process. In ancient times, it was very important for the digestion and assimilation of plant foods, but then this function atrophied. The appendix is associated with the immune system, but when it is removed, intestinal functions are not impaired. There is a sphincter between the intestine and the appendix that acts as a barrier. Thanks to it, food does not get into the appendage.
- Colon. This part of the intestine is the largest section of the large intestine, so it is easily detected by palpation. It is usually divided into 3 parts, and the whole thing resembles a horseshoe or semicircle. It begins with the ascending colon (goes immediately after the cecum), then the transverse and descending colon. In this section, moisture and electrolytes are absorbed, feces become harder due to dehydration and move further.
- Sigmoid colon. It is located on the left side of the abdomen. Its name comes from the Latin letter S (sigma). It is very important in terms of absorption function: most of the liquid from food is absorbed here, and only then the absorbed moisture is distributed throughout the body. Here the formation of feces continues and their movement further through the intestines. Feces can be retained in the bends of this section, causing inflammation.
- Rectum. This section is the final section for the entire intestine. This is a very short section, the length of which rarely exceeds 15 cm. The inner layer has many mucous cells, whose work is activated during various disorders, hence the mucus in the stool. Despite the name, the intestine is not straight at all, it has bends. Here the process of breaking down food comes to an end. Everything that could be absorbed from food has already been absorbed, feces are formed and excreted from the body.
How long is the small intestine?
It is difficult to measure the length of the small intestine in a healthy person, but researchers estimate it ranges from 3 to 5 meters.
The three sections of the small intestine vary significantly in length:
- The length of the duodenum is about 20–25 centimeters.
- The jejunum is about 240 centimeters in length.
- The length of the ileum is about 300 centimeters.
Earlier studies have shown that total intestinal length correlates with weight, such that heavier people have longer intestines.
The small intestine is long enough that a person can undergo small intestinal resection surgery to remove part of it if an underlying disease or condition causes it to stop functioning.
Colon diseases
Crohn's disease involves inflammation of all organs of the gastrointestinal tract.
All diseases of the large intestine can be combined according to their symptoms. Usually these are stool disorders, diarrhea and constipation that alternate, pain in the side of the abdomen that goes away after defecation for some time, increased gas formation. However, with diseases of this part of the intestine there is no sudden weight loss and hypovitaminosis. Common diseases:
- Crohn's disease. This name hides a number of disorders and diseases. Crohn's disease is characterized by inflammation of not only the colon, but also all organs of the gastrointestinal tract as a whole, even the stomach and esophagus. The lesion is heterogeneous, healthy tissues alternate with inflamed ones. Symptoms may vary depending on the location of the inflammation. Often the disease is complicated by the formation of fistulas, ulcers, and intestinal obstruction.
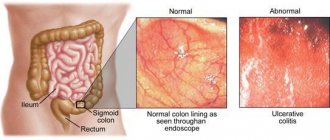
- Colitis (ulcerative, ischemic). Ulcerative colitis usually affects the rectum, but it can also affect other parts of the large intestine. The causes of ulceration are still not fully understood. It is known that heredity plays an important role. Colitis is often accompanied by bleeding and stool disorders. Ischemic colitis is caused by narrowing of the intestinal blood vessels. The blood supply to the intestine becomes difficult, which causes many problems.
- Colon cancer. Malignant colon tumors are more common than benign ones. Colon cancer ranks first in terms of incidence among cancer diseases. Polyps, fistulas and ulcerative colitis, if left untreated, are prerequisites for the development of cancer.
- Irritable bowel syndrome. This disease is also called dyskinesia. Under the influence of various factors, intestinal motility and the release of hormonal substances in it are disrupted. The disease manifests itself in the form of constipation and pain in the abdominal area.
- Megacolon. This is the name for the expansion of individual sections of the colon. The disease is accompanied by severe constipation, despite diet and sufficient fluid intake, abdominal pain, and flatulence. In this case, gases accumulate and are poorly discharged, as a result of which the patient complains of severe bloating, bulging of the abdominal wall, and heaviness.
If the disease becomes complicated and severe, the only treatment option is surgery.
Diagnostics
Diagnosis of the large intestine begins with a digital examination of the anus. Next, laboratory and instrumental studies begin. , endoscopy of the large intestine is diagnostically valuable - sigmoidoscopy and colonoscopy . During sigmoidoscopy, the doctor examines the rectum and sigmoid colon, and during colonoscopy, the entire large intestine.
Irrigoscopy is an X-ray diagnosis of the large intestine after filling through the anus with a contrasting barium suspension. Plain radiography of the abdominal organs without the use of contrast is informative in case of intestinal obstruction. The so-called Kloiber cups, horizontal fluid levels in the intestinal lumen. This is a symptom specific to intestinal obstruction.
Of the laboratory tests, the main place is occupied by the diagnosis of stool. Depending on the tasks assigned, feces are taken for:
- general analysis (coprogram);
- occult blood;
- worm eggs;
- bacterial culture on nutrient media.
A supporting role is played by a general and biochemical blood test, immunodiagnostics and blood culture on nutrient media.
What causes diverticula?
Often, when visiting a doctor, patients diagnosed with diverticular disease ask the question: “Why did this disease develop?” What are the causes of this disease? A large amount of information on the Internet does not always provide a clear explanation. Let's try to tell you more.
We believe that all the main causes of diverticular disease can be divided into two interrelated groups:
- Increased pressure in the intestinal lumen;
- Weakness of the intestinal wall.
A deficiency of plant fiber in the diet leads to a decrease in the volume and increase in the density of feces, which causes disturbances in the motor activity of the colon: it reacts to even minor irritation with chaotic contractions. Thus, short, closed segments of the intestine appear with increased intraluminal pressure, which leads to bulging of the mucosa through the “weak” areas of the intestinal wall - the places where the blood vessels pass.
To clearly understand the formation of a diverticulum, we offer you an interesting comparison:
“The intestinal wall is similar to the layered structure of a football - the outside is strong and hard skin, and the inside is a soft but elastic rubber chamber.
Now imagine that a hole, a hole, forms in the outer hard shell of this ball. What will happen then? The high pressure inside the ball will push part of the soft and elastic inner rubber chamber outward, creating a pocket that sticks out. This can be compared to a hernia in the abdomen - the contents “bulge out” through a defect in the muscles.
About the same thing happens to the colon with diverticulosis. If the pressure inside the intestinal lumen is high, and there are weak spots in the muscle layer, then the inner lining of the intestine tends outward through these openings, forming protrusions in the form of pouches. They are called diverticula."
Gateway system
In general, normally there are narrowings in the large intestine, which have been described for a long time. Nevertheless, little attention is paid to this in modern literature. What does this lead to? And to the fact that during diagnostic studies, anatomical narrowings are sometimes mistaken for organic pathology. This is very important, especially if after irrigoscopy you are deciding on surgery. During my work I have to communicate a lot with endoscopists, who constantly observe these sphincters during colonoscopy.
So, in order.
3. Muscular lining of the colon wall
- This is the layer of the colon wall located outside the submucosa of its wall.
The purpose of the muscular lining of the colon is to participate in mixing food masses and in their movement through the digestive tract. The terminal intermuscular nerve plexuses are located in the muscular layer of the hollow organs of the gastrointestinal tract. They are the final links in the regulators of the functions of the digestive system. The muscularis propria may consist of smooth muscle tissue or striated muscle tissue. For example, in the initial and middle sections of the colon, the muscular layer consists of smooth muscle tissue, and in the final section (external anal sphincter) the muscular layer consists of striated muscle tissue. Bundles of smooth muscle cells lie in two layers. The direction of muscle cells in these layers is different. Directly adjacent to the submucosa are circular bundles of smooth muscle cells. This layer is called the inner circular layer. Outside the circular layer is a longitudinal layer of smooth muscle cells. The fibers of the outer longitudinal muscular layer of the colon are not only distributed throughout the entire wall, but are also concentrated in three clearly visible longitudinal muscle bands (see Diagram 1). The width of the tapes is ~5 ÷ 8 cm
.
They begin at the base of the appendix and extend along almost the entire colon with the exception of the distal sigmoid colon and rectum. A cross-section of the colon shows that the bands are located approximately 120 degrees in relation to each other. Each tape, in accordance with its position or relationship to other organs, has its own name: free tape
,
mesenteric tape
and
omental tape
.
The circular muscle fibers of the muscle layer lying closer to the colon mucosa also have regular thickenings. These condensations can serve as the basis for external structural regular circular constrictions (see Scheme 1). Muscle fibers concentrated in muscle bands and circular constrictions have greater tone than evenly distributed muscle fibers of the muscle layer. Therefore, along the entire length of the colon wall, in places of the least tone of the muscle fibers, there are external protrusions (internal depressions) - haustra of the colon
.
The haustra are bounded by muscle bands and circular constrictions. The pattern of distribution of protrusions can vary significantly among different people. Haustra are often absent from the proximal cecum, may begin in the ascending colon, and are rarely found in the ascending and proximal transverse colon. Protrusions often occur in the distal transverse colon, descending colon, and sigmoid colon. The rectum has no external protrusions and omental processes. Regular thickening of the muscle layer is the basis for the morphological sphincters
and
functional sphincters
of the colon.
Morphological sphincters have clearly defined anatomical characteristics. Functional sphincters, although they do not have pronounced anatomical differences from the normal wall of the colon, but have all the functions of sphincters. Along with the morphological sphincters, they are the executive apparatus in controlling the movement of the contents of the colon. At the border of the small and large intestines, in front of the entrance to the cecum, the ileocecal (ileocecal) valve
.
It is also called the Tulpa 1
(named after its discoverer);
synonyms: Varolius valve 2
, Bauginian
valve
3 Three sphincters are found in the cecum. At the border of the cecum and its appendix there is a sphincter that acts as a valve that blocks the passage from the cavity of the cecum to the appendix. It is called the sphincter (valve) of the appendix
;
synonym: sphincter (valve) of Gerlach 4
.
At the level of the lower edge of the ileocecal valve is the proximal cecal ascending sphincter of the cecum
;
synonym: sphincter Busi 5
.
At the level of the upper edge of the ileocecal valve is the distal cecal ascending sphincter
;
synonym: Hirsch sphincter 6
.
There are three functional sphincters throughout the transverse colon. The right transverse colon sphincter
is located at the proximal part of the transverse colon;
synonym: right sphincter of Cannon 7
-Bam
8
.
In the middle part of the transverse colon is the middle sphincter of the transverse colon
;
synonym: middle sphincter of Cannon 7
.
Closer to the left (splenic) flexure of the colon is the left sphincter of the transverse colon
;
synonym: left sphincter of Cannon 7
.
There are two sphincters in the descending colon. Immediately distal to the left flexure of the colon, is the sphincter of the descending colon
;
synonym: sphincter of Payr 9
-Strauss
10
.
During the transition of the descending colon into the sigmoid colon, the descending sigmoid sphincter
;
synonym: Bally sphincter 11
.
The sigmoid colon has two sphincters. Proximally, approximately in the middle part of the sigmoid colon, the sigmoid colon sphincter
;
synonym: sphincter of Rossi 12
-Muthier
13
.
Distally, at the border of the sigmoid colon and rectum, the sigmoid-rectal sphincter
;
synonym: O'Byrne sphincter 14
-Pirogov
15
-Muthier
12
.
There are three sphincters in the rectum. The third rectal sphincter
is located in the proximal rectum .
In the area of the anal canal of the rectum, a thickening of the muscular lining of the intestine forms the internal (involuntary) anal sphincter
.
the external (voluntary) anal sphincter,
formed by striated muscle fibers .
Meanwhile, the muscle of the external anal sphincter no longer belongs to the muscular lining of the wall of the colon, but to the muscles of the perineum. These three sphincters are the main executive apparatus in controlling the act of defecation. See the diagram in a separate window: Sphincters of the gastrointestinal tract. Notes 1
Tulp, (born Klaus Pietersohn), Tulp, Nicolaes, 1593-1674, Danish surgeon.
2
Varolius, Varolius, Varolio (Varolius) Constanzo, 1543-1575, Italian anatomist.
3
Bauhin, Gaspard, (Caspar Bauhin, Caspar Bauhinius), 1560-1624, Swiss physician, anatomist and botanist.
4
Gerlach, Joseph von Gerlach, 1820-1896, German anatomist.
5
Busse, Otto, 1867-1922, German pathologist.
6
Hirsch, JS, German scientist.
7
Cannon, Cannon Walter Bradford, 1871-1945, physiologist, USA, see photo, second from right.
Cannon W.V. The movements of the intestines stadded by means of the roentgen rays. Am. J. Physiol., 1901-1902, 6, 251-277. 8
Böhme Arthur, 1878-?, German physician.
9
Payr, E. Payr, 1871-1946, German surgeon.
10
Strauss, Strauss N., 1868-1945, German doctor.
11
Balli R., Balli R., Italian radiologist.
Balli R.: The sphincters of the colon. Radiology, 1929, 12, 6, 484-495. The Italian radiologist R. Balli proposed dividing the transverse colon into three sections: proximal, middle and distal (according to the sources of blood supply) and for the first time summarized data on the morphology, radiology and pathology of the sphincters of the colon. Balli R. The sphincters of the colon. Radiology, 1929, 12, 6, 484-495. Balli R. The sphincters of the colon. Radiology, 1939, 33, 3, 372-376. 12
Rossi, K., Italian radiologist.
Quote by: Frolkis A.V. Functional diseases of the gastrointestinal tract, Leningrad, “Medicine”, 1991, 224 p. 13
Moutier, Moutier F., ??
The radiograph revealed a distinct contraction ring in the lower part of the sigmoid colon and a temporary delay in the movement of the contrast mass. 14
O'Bern (O'Bernier), O'Beirne J. ?
15
Pirogov Nikolai Ivanovich, 1810-1881, Russian surgeon, naturalist, teacher and public figure.
I was unable to find all the information about some of the scientists who were the discoverers of the structures described. If anyone can fill this gap, please write to me or to the guest book (see menu at the bottom of each page).
| Scheme. Enteric nervous system . | |
| The enteric nervous system is a section of the visceral part of the nervous system, which is a neural network located in the walls of the gastrointestinal tract. The network consists of interacting afferent neurons, interneurons and efferent neurons. It is located between the layers of the walls of the gastrointestinal tract. Nerve fibers of the autonomic nerve plexus innervating the gastrointestinal tract approach and depart from this network. The enteric nervous system is the final executive element in the hierarchy of regulators that control all functions of the gastrointestinal tract. It functions as an effector, the control center of the digestive system. The enteric nervous system has relative independence and other properties of local regulators. At the same time, the enteric nervous system is modulated by signals arriving through postganglionic sympathetic nerve fibers and preganglionic parasympathetic nerve fibers from the autonomic nerve plexuses. | |
4 . The outside of the large intestine is covered with a serous membrane
(peritoneum).
The cecum, transverse colon, sigmoid colon and proximal third of the rectum are covered on all sides by the peritoneum, that is, they are located intraperitoneally, intraperitoneally. The ascending colon, descending colon, and the middle part of the rectum are not completely covered with peritoneum, but only on three sides, that is, they are located mesoperitoneally. The distal third of the rectum is not covered by the peritoneum and is located extraperitoneally, extraperitoneally. The outer layer of this part of the intestine is the adventitia. The peritoneum covering the large intestine, when moving to the walls of the abdominal cavity or to neighboring organs, forms mesenteries, numerous folds called colic ligaments
. These folds (ligaments) fix the large intestine, prevent its displacement and prolapse, and serve as pathways for the blood vessels of the intestine. The number of such ligaments varies significantly.
Literature. Illustrations. References. Illustrations
Click here to access the site's library! Click here and receive access to the reference library!
- Aksenenko A.V. Human sigmarectal sphincter: clinical and morphological parallels. In the book: Baitinger V.F., ed. Sphincters of the digestive tract, Siberian State Medical University, Tomsk, 1994, 207 p. A unique collection of scientific works.
The quality of the book is evidence of the miserable situation of talented people in Russia . Access to this source = Access to the reference. URL: https://www.ssmu.ru/office/f1/operative/interview.shtml quotation - Baitinger V.F. Upper esophageal sphincter: structural, functional and clinical aspects. In the book: Sphincters of the digestive tract, Siberian State Medical University, Tomsk, 1994, pp. 46-67. Fundamental, carefully conducted research, excellent report on the work.
The quality of the book is evidence of the miserable situation of talented people in Russia . Access to this source = Access to the reference. URL: https://www.ssmu.ru/office/f1/operative/interview.shtml quotation - Baitinger V.F., ed. Sphincters of the digestive tract, Siberian State Medical University, Tomsk, 1994, 207 p. A unique collection of scientific works.
The quality of the book is evidence of the miserable situation of talented people in Russia . Access to this source = Access to the reference. URL: https://www.ssmu.ru/office/f1/operative/interview.shtml quotation - Baitinger V.F., Aksenenko A.V. Sphincters of the human sigmoid colon. In the book: Sphincters of the digestive tract, Siberian State Medical University, Tomsk, 1994, pp. 174-181. Fundamental, carefully conducted research, excellent report on the work.
The quality of the book is evidence of the miserable situation of talented people in Russia . Access to this source = Access to the reference. URL: https://www.ssmu.ru/office/f1/operative/interview.shtml quotation - Kolesnikov L.L. Moscow State Medical and Dental University, Department of Human Anatomy, Human sphincter apparatus, St. Petersburg, Special Literature, 2000, 183 p. A guide for clinicians, a textbook for university students.
Unique work! The quality of the book is evidence of the miserable situation of talented people in Russia . Access to this source = Access to the reference. URL: https://www.anatom-mgmsu.ru/personalii/ quotation - Andersen IS, Michelsen HB, Krogh K, Buntzen S, and Laurberg S. Impedance Planimetric Description of Normal Rectoanal Motility in Humans using impedance planimetry. Diseases of the Colon & Rectum, 2007, 50, 11, 1840-1848. Review
. . Access to this source = Access to the reference. URL: https://www.tryfonov.ru/tryfonov/serv_r.htm#0 quotation - Dahl J., Greenson JK Colon = Large intestine. In: Mills SE Histology for Pathologists = Histology for Pathologists, 3rd ed., Lippincott Williams & Wilkins, 2006, 1280 p. Illustrated study guide and guide.
In .chm format . Access to this source = Access to the reference. URL: https://www.tryfonov.ru/tryfonov/serv_r.htm#0 quotation - Koch TR Colonic Diseases = Diseases of the colon. Humana Press, 2003, 572 p. Illustrated textbook.
Physiology, pathophysiology, medicine . . Access to this source = Access to the reference. URL: https://www.tryfonov.ru/tryfonov/serv_r.htm#0 quotation - MedPics. An Image Library for Medical Education = An Image Library for Medical Education. Digestive System, UCSD School of Medicine, Office of Educational Computing, 2008, University of California, San Diego. Illustrated textbook
. . Access to this source = Access to the reference. URL: https://medpics.ucsd.edu quotation - Messmann H., Ed. Atlas of Colonoscopy: Techniques, Diagnosis, Interventional Procedures = Atlas of Colonoscopy: technique, diagnosis, treatment procedures, Thieme Medical Publishers, 2005, 236 p. A beautifully illustrated guide
. . Access to this source = Access to the reference. URL: https://www.tryfonov.ru/tryfonov/serv_r.htm#0 quotation
See: Gastroenterology: dictionary, Gastroenterology: Literature. Illustrations,
| LIBRARY = LIBRARY Human Physiology = Human Physiology, Human Anatomy = Human Anatomy, Human Biochemistry = Human Biochemistry, Human Psychology = Human Psychology, Medicine = Medicine, Mathematics = Mathematics, Chemistry = Chemistry, Physics = Physics, General Scientific Literature = General Science Lexis. Click here to access any source in the site's library! Click here and receive access to the any reference of the library! “I AM LEARNED. . . N E D O U C H A ?” T E S T V A S H E G O I N T E L L E C T A Premise : The effectiveness of the development of any branch of knowledge is determined by the degree of compliance with the methodology of knowledge - the knowable entity. |
Error? Click here and fix it! Search on the site E-mail of the author (author)
Introduction
Over the past 20 years, the number of patients with diverticular disease has increased significantly, which is primarily due to changes in the nature of nutrition, a decrease in fiber and dietary fiber in the diet and, as a consequence, the development of constipation. For patients suffering from diverticular disease, as well as their relatives, it is important to understand all stages of development, methods of diagnosis and treatment of this disease. To fully understand the pathological process, it is necessary to begin studying the issue from the basics - the anatomical features of the organ.
How to treat diverticular disease, diverticulosis and diverticulitis?
Drug treatment
When treated promptly, diverticulitis responds very well to drug treatment. Inflammatory changes can be completely cured with antibacterial and anti-inflammatory therapy.
If complications develop in patients, the treatment method must be selected as least traumatic and minimally invasive as possible. The infiltrate can be completely cured with medication. The abscess can be punctured under ultrasound or CT control.
Surgery
In case of peritonitis and the need for surgery in the early stages of the disease, intervention can be performed laparoscopically - through small punctures.
Unfortunately, the development of fecal peritonitis, as a rule, requires laparotomy - a “large incision” for thorough washing and examination of the abdominal cavity.
Surgical treatment of diverticular disease outside periods of exacerbation is especially important for active travelers, as well as patients living far from regional centers. If an exacerbation of the disease occurs far from centers where you can get quality medical care, the consequences can be very unpleasant. If there are three or more attacks of diverticulitis in a year, the patient should contact the coloproctology department to determine the optimal treatment tactics outside the period of exacerbation. If surgical treatment is necessary, the operation of choice in this case is laparoscopic removal of the affected area of the colon and rectosigmoid junction as one of the causes of increased pressure in the intestinal lumen. In this case, removal of the stoma (even temporarily) is not required.
Comparisons
For anyone who has difficulty imagining their own intestinal length, the following comparisons may help:
- The colon, when stretched, is the height of a short adult. The smallest parts of the colon are about the size of your thumb.
- The small intestine is on average longer than a van and about as long as a pickup truck. The length of the small intestine varies from person to person by about the height of a very tall person.
- Research shows that the total surface area of the intestines is about half the size of a badminton court.