The gallbladder performs an important function in the body; disruption of its functioning can lead to very unpleasant consequences. Bile produced by the liver is stored in the gallbladder until the body needs it. This usually happens when food enters the stomach. Bile begins to flow into the duodenum, where, together with pancreatic juice, it helps digest food and facilitates bowel function. What are the symptoms of a kinked gallbladder?
Symptoms of a bent gallbladder
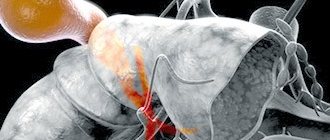
Ultrasound of the gallbladder
If a malfunction occurs in the body, such as a bend in the gallbladder, the symptoms of which will be described below, the outflow of bile is disrupted, and bile, as is known, is quite caustic and can damage any organ, including the gallbladder itself.
- Nausea and vomiting. Nausea and vomiting may occur periodically, especially after a large meal. A dangerous sign is constant nausea and frequent vomiting. In this case, we can talk about a threat to life.
- Constipation. Impaired digestion and insufficient flow of bile into the duodenum lead to the fact that the intestines cannot cope with their work. Constipation when the gallbladder is bent is inevitable.
- Gastric reflux. This is a painful and dangerous syndrome, the essence of which is that the standard chain of food promotion is disrupted. From the intestines, bile with semi-digested food remains enters the stomach, which causes pain, heartburn, nausea, and in some cases even a burn of the gastric mucosa.
- Sweating. Excessive sweating is a manifestation of general weakness of the body. If the pain is severe, cold, sticky sweat may also appear.
- Bloating. The release of bile into the stomach and its contact with the acidic environment prevailing in the stomach contributes to increased gas formation. The patient experiences a feeling of bloating that does not go away even after visiting the toilet.
- Pain in the right side. Abdominal pain is usually aching in nature. When bile enters the stomach, a feeling of pain in the abdomen may occur.
- Bitterness in the mouth. The presence of bile in the stomach and even the esophagus causes a feeling of unpleasant bitterness in the mouth.
Ultrasound diagnostics in questions and answers
— What is the equipment in your clinic in the department of ultrasound and functional diagnostics?
The department of ultrasound and functional diagnostics (USD, FD) is equipped with equipment from leading world companies. There are 3 ultrasound scanners: an expert-class ultrasound system HD11 manufactured by Philips Medical Systems (USA), Panther Ultrasound Scanner Type 2002 ADI and Merlin Ultrasound Scanner Type 1101 from V&K MEDICAL A/S (Denmark) with a full set of multi-frequency sensors for locating internal organs , soft tissues, heart and blood vessels, operating in 2- and 3-D, Color, CPA, PW, CW, TDI, M-mode and THI modes. The functional diagnostics department is equipped with equipment from SCHILLER (Switzerland). Heart rate and blood pressure are monitored using an ambulatory blood pressure recorder BR-102 PLUS and an ambulatory ECG Holter recorder MT-200 from SCHILLER.
— What studies are carried out in the ultrasound department?
In the department related to ultrasound diagnostics, a full range of ultrasound examinations (ultrasound) is carried out: abdominal organs and retroperitoneal space, transabdominal (external) ultrasound of the pelvic organs in men and women, transrectal and transvaginal (internal) ultrasound of the pelvic organs (TRUS, TVUS), ultrasound of the scrotum, thyroid gland, mammary glands, lymph nodes, salivary glands, soft tissues, ultrasound of joints, lungs and pleura. What is important is that an ultrasound is performed with color and energy mapping. This means that by assessing the nature of blood flow, it is possible to distinguish inflammatory or tumor tissue from healthy tissue.
— What organs can be examined with an ultrasound of the abdominal cavity?
When performing an ultrasound of the abdominal cavity, the pancreas and its duct, large vessels (the abdominal aorta is the main vessel of the abdominal cavity), the liver and its vessels, the bile ducts, and the gallbladder are examined. Although the kidneys, adrenal glands and spleen are located in the retroperitoneal space, their ultrasound examination is also included in the standard protocol. We also locate all “suspicious” areas of the abdomen that your doctor identified during the examination. Therefore, it is advisable that a consultation with the attending physician (therapist, surgeon) precede an ultrasound scan.
— What can be assessed with an ultrasound of the abdominal organs?
Ultrasound evaluates the size of the organ (there is a norm for each organ and its parts), echostructure, density, the presence of pathological formations (stones, cysts, tumors), and the nature of the blood flow.
— Is it possible to take a piece of tissue or organ to study under a microscope? What organs can be examined in this way? And what is this for?
This is called a biopsy. An aspiration and fine-needle biopsy is performed using a special thin needle under ultrasound guidance. The manipulation is carried out both under local anesthesia and under medicated sleep. In this way, you can examine all soft tissues (skin and subcutaneous tissue formations, muscles), enlarged lymph nodes, salivary glands and, very importantly, internal organs. For example, in our clinic, under ultrasound guidance, puncture of cysts of the kidneys, thyroid gland, prostate gland, soft tissues, and lymph nodes is performed. The purpose of such studies is the early diagnosis of cancer, establishing an accurate diagnosis, which allows for appropriate treatment in the future.
— What liver diseases can be diagnosed with ultrasound?
Most liver diseases have their own characteristic ultrasound picture. These are acute and chronic hepatitis, cirrhosis of the liver, fatty infiltration of the liver (fatty hepatosis or steatosis), liver formations (common benign formations - hemangiomas), fluid cyst formations (congenital, post-traumatic), liver cancer, metastatic liver lesions.
— When and how is an ultrasound of the gallbladder performed?
The gallbladder is an integral part of the biliary system; it also includes the biliary tract. To assess the condition of the biliary system, the patient must properly prepare for an ultrasound. The patient must adhere to a diet for 1.5 -2 days with the exception of vegetables, fruits, black bread, dairy products, carbonated drinks, and vegetable juices that cause bloating. The examination itself should be carried out on an empty stomach - abstaining from food and liquid intake 8-12 hours before the examination. Ultrasound evaluates the location and shape of the bladder and duct system, measures the size, and evaluates the condition of the walls and cavity of the gallbladder. Indications for this study are all unclear pain in the upper abdomen and right hypochondrium, inflammatory process in the abdominal cavity, jaundice.
— What is an S-shaped gallbladder? Is it dangerous?
An S-shaped gallbladder is one of the anomalies of its development, the so-called shape anomaly. This type of anomaly also includes kinks and U-shaped deformation. This is not dangerous, but in some cases it can contribute to the development of biliary dyskinesia.
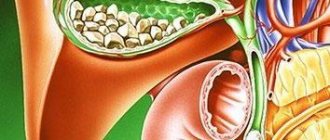
— Can you see stones in the gall bladder?
Gallstone disease is one of the diseases that is successfully diagnosed by ultrasound. The gallbladder is not the only location for stones. Stones can also be located in the bile ducts. This complication of cholelithiasis is called choledocholithiasis, leading to impaired outflow of bile and jaundice. Easily diagnosed using ultrasound.
— How can ultrasound determine the presence of an inflammatory process in the gallbladder? What are the dangers of long-term inflammation in this area?
Acute cholecystitis (inflammation of the gallbladder) is often encountered in the practice of ultrasound diagnostics. This disease has its own characteristic features: an increase in the size of the gallbladder, a sharp thickening of the wall (sometimes a double contour appears), swelling of the surrounding tissues. In this area we will see enlarged lymph nodes, and a study of the blood flow in this area will reveal signs of acute inflammation. Chronic cholecystitis also has its own characteristic ultrasound signs. The danger of a long-term chronic inflammatory process in this area is that it often leads to the development of cancer of the biliary system.
— What are gallbladder polyps? Why are they dangerous?
Polyposis is one of the most common gallbladder lesions. It has characteristic ultrasonic signs - a parietal immobile formation (or formations), which has a close connection with the wall of the bladder in the form of a leg. The danger of these formations lies in their ability to malignize (become malignant). Therefore, one of the methods for monitoring such patients is dynamic monitoring of the size, number and ultrasound characteristics of polyps (for initial detection - monitoring after 1 month, then after 3 months, and then once every 6 months). With the rapid growth of these formations and changes in their ultrasonic properties, surgical treatment is indicated.
— How can you check the functioning of the gallbladder?
For this purpose, dynamic ultrasound cholecystography (test with a choleretic breakfast) is performed - this study allows you to evaluate the function of the biliary tract, determine the type of dyskinesia (impaired motility) of the gallbladder, and, depending on the identified disorders, prescribe appropriate treatment.
— What diseases of the pancreas can be diagnosed using the ultrasound method? How difficult is it?
This organ is the most difficult to visualize due to its location. Therefore, to obtain a high-quality and informative image, it is necessary to prepare the patient well, have high-class equipment and a qualified specialist. Almost all diseases of the pancreas have their own distinctive ultrasound signs. These include acute pancreatitis and its complications, chronic pancreatitis, lipomatosis or steatosis of the pancreas due to impaired fat metabolism, cysts (fluid formations), tumors (both benign and malignant).
— What information does ultrasound examination of the kidneys provide?
Ultrasound of the kidneys makes it possible to evaluate the following important parameters: the location of the kidneys, their number, size, contours and shape of the kidneys, their structure, the ratio of the different layers of the kidney, the condition of the tissues surrounding it (perirenal tissue). Among the anomalies of kidney development, the most common are dystopia (when the kidney is not in its usual place), double kidneys, absence of a kidney, structural abnormalities - polycystic, multicystic, spongy kidney. A fairly clear ultrasound picture is observed with nephroptosis (pathological displacement of the kidney), and kidney cysts (fluid formations) are often found.
— What kidney diseases can be diagnosed using ultrasound?
Most often in urological practice, inflammatory diseases of the kidneys and urinary tract occur. First of all, this is acute pyelonephritis, but in uncomplicated forms, no ultrasound signs of changes in the kidneys are detected. In severe cases of the disease, the size of the kidney increases and the ultrasonic density of the parenchyma decreases. The second most common disease in urologist practice is urolithiasis. Currently, ultrasound is a priority study in the diagnosis of stones in the urinary system. The advantage of this method is the ability to visualize stones of any chemical composition, including X-ray negative stones (invisible during X-ray examination).
— What kidney tumors exist and can a kidney tumor be seen with ultrasound?
There are benign and malignant kidney tumors. The first group includes angiolipomas, leiomyomas, rhabdomyomas, etc. According to ultrasound data, these formations have their own clear signs and require dynamic monitoring. Malignant tumors include renal cell carcinoma and various sarcomas. Their presence can be suspected by ultrasound, but an accurate diagnosis of the nature of the lesion is possible with surgery after additional examination.
— How is ultrasound examination of the prostate gland performed? What can you see? For what diseases and at what age should you undergo regular ultrasound examination of this organ?
Ultrasound of the prostate gland is performed in two ways - transabdominal (external, when the sensor is placed on the anterior abdominal wall) ultrasound and transrectal (using a special sensor - through the rectum) - TRUS. During transabdominal ultrasound, the patient should have a full bladder to improve image quality. The location of the prostate, its shape, structure, size, relationship with surrounding organs and tissues, the presence of nodules are assessed, growths of gland tissue (hyperplasia), as well as tumors are identified. The quality of the image, and, accordingly, the accuracy of diagnosis is significantly improved with TRUS, since in this case the sensor is closely adjacent to the organ. Also, with the help of TRUS, the seminal vesicles are clearly visible. Using ultrasound, inflammatory diseases (chronic or acute prostatitis, gland abscesses), cysts, benign prostatic hyperplasia (“adenoma”), as well as prostate cancer are diagnosed. Based on the above, prostate ultrasound should be performed regularly in persons over 40 years of age, once a year (in the absence of complaints). If there are complaints, the examination is carried out at a younger age and more often.
— Who is indicated for an ultrasound of the bladder? What diseases can be detected using ultrasound?
Since the bladder is an integral part of the genitourinary system, ultrasound examination of this organ is indicated in all cases of diseases of other parts of the genitourinary system (kidneys, prostate gland, seminal vesicles, uterus and ovaries), as well as in cases of changes in urine tests. An ultrasound is performed with a full bladder. In this case, it is possible to identify abnormalities in the development of the bladder and the final sections of the ureter - diverticula (these are cavities containing urine and connected to the bladder cavity through a narrow neck). Ureterocele is a saccular “sagging” of the wall of the final section of the ureter into the bladder cavity (congenital or acquired). In a full bladder, small (1-2 mm in diameter) and large concretions (stones) are clearly visible. In inflammatory diseases of the bladder (cystitis), a thickened, compacted wall of the organ is sometimes visible, and an inflammatory suspension appears in the lumen. The most valuable information from ultrasound can be obtained for bladder tumors. Most bladder tumors have a papillary structure and without treatment always become malignant, so early diagnosis in these cases is very important. Ultrasound can accurately determine the location of the tumor, its size, extent, and also assess the presence and extent of damage to the bladder wall, paravesical (surrounding the bladder) tissue, nearby organs, lymph nodes, etc.
— What diseases can be diagnosed using ultrasound of the scrotum? How is this study carried out, is special preparation of the patient required?
Ultrasound of the scrotal organs is performed using a contact method and does not require special preparation of the patient. This reveals abnormalities in the development of the testicle, hydrocele of the testicular membranes (hydrocele), cysts of the testicle and its epididymis (spermatocele), and varicose veins of the spermatic cord (varicocele). Epididymitis (inflammation of the epididymis) is one of the most common diseases of the genital organs in men; it can be acute or chronic. In most cases, it is infectious in nature. Tuberculosis of the epididymis accounts for about 20% of all diseases of the genital organs in men. Orchitis - inflammation of the testicle - is also often encountered in the practice of a urologist; it can complicate the course of an infectious disease or occur after an injury. All these diseases have a characteristic ultrasound picture.
— Is it possible to suspect a testicular tumor based on ultrasound data?
Testicular tumors (seminoma, teratoma, androblastoma) are rare, but are one of the most common causes of death from cancer in young men 20-35 years old. Therefore, early diagnosis is so important in those patients when the tumor does not yet have obvious clinical manifestations, is not detected, but is only suspected by the doctor. According to ultrasound data, a characteristic picture of organ damage is determined. At risk are patients with cryptorchidism (undescended testicle) after testicular trauma.
— What are the possibilities of ultrasound in diagnosing thyroid diseases?
Using ultrasound scanning, diseases such as diffuse toxic and non-toxic goiter, various thyroiditis (inflammatory diseases of the thyroid gland), nodular goiter, toxic adenomas, cancer, etc. are diagnosed. Each of these diseases has its own characteristic ultrasound picture. Ultrasound morphometry is performed to assess the size and volume of the gland. The final stage of ultrasound in patients with nodular formations is a targeted biopsy of the thyroid gland under ultrasound guidance.
— In what cases is ultrasound of the mammary glands performed?
Ultrasound of the mammary glands is an informative method for identifying various diseases of this organ. It should be remembered that at different age periods the echostructure of the glands differs from each other. What is normal for a woman of reproductive age will be pathological for a woman of menopause. Ultrasound of the mammary glands is performed in children and adolescents, in healthy young women, starting from 25-30 years old, in pregnant and lactating women, when areas of compaction are identified during mammography or palpation, in the acute period of injury or inflammation, to assess the condition of the mammary glands after prosthetics , in premenopausal women and taking hormonal medications. In addition, ultrasound of the mammary glands is performed during examination in men, especially if there are lumps in the gland or discharge from the nipple.
— What diseases of the mammary glands can be detected using ultrasound?
First of all, these are cysts (fluid formations) - the most common diseases of the mammary glands in women of reproductive age. They have a typical picture according to ultrasound, so the accuracy of ultrasound diagnosis of cysts is 98-100%. The size of cysts can range from a few millimeters to 5-6 cm in diameter, they can be single or multiple, they can have septations and be multi-chambered. If the image of a cyst is atypical (has dense internal contents, parietal calcifications), it is necessary to perform a puncture biopsy of such a cyst under ultrasound control to clarify the diagnosis. Dilation of the milk ducts (ductectasia) can be physiological: during lactation and during pregnancy, in the 2nd phase of the menstrual cycle. Therefore, routinely, an ultrasound of this organ should be performed in the 1st phase of the menstrual cycle (that is, on the 5-7th day from the start of menstruation). Often there are inflammatory diseases of the mammary glands - mastitis, mammary abscess. These diseases have their own characteristic ultrasound signs and are easily diagnosed using ultrasound. Gynecomastia is fatty hypertrophy of the mammary glands in men, develops against the background of various diseases or as a result of the influence of certain medications, and also has its own characteristic ultrasound features. Dysplasias are characterized by a violation of symmetry. size, configuration of the mammary glands. These include hypertrophy of the mammary glands (an increase in the volume of the gland by more than 50%), hypotrophy (a decrease in the size of the mammary glands). Dishormonal hyperplasia (proliferation of gland tissue (adenosis, adenomatosis)) are diseases that need to be differentiated from the early stages of breast cancer, and therefore require special attention from both the ultrasound diagnostician and the clinician.
— What types of mammary gland formations exist? How are they diagnosed using ultrasound?
Fibroadenoma is the most common benign tumor of the mammary glands in women aged 15 to 45 years. As a rule, fibroadenoma is a single formation, but multiple and one- and two-sided lesions occur. Echographic signs are varied; the formation can mask a malignant tumor. Requires dynamic observation and histological verification (i.e., a biopsy with analysis of the nature of the tissue). Breast cancer is the disease with which all benign processes in the mammary gland are differentiated. There are various ultrasound symptoms characteristic of cancer of this organ. Most often, breast lesions are detected in the upper-outer quadrant. The process can be diffuse or nodular in nature, one- or two-sided. Metastases to the mammary gland account for 1 to 6% of all malignant processes in it. Unlike primary tumors, metastases are usually located in the subcutaneous zone. An aspiration biopsy is also performed to clarify the diagnosis.
— What information does ultrasound provide after plastic surgery on the mammary glands?
The need for a visual assessment of the condition of the mammary gland and surrounding tissues arises after plastic surgery and other types of correction of the mammary glands. Breast augmentation can be performed for cosmetic reasons and after a mastectomy (removal of the breast). In both cases, the condition of the endoprosthesis and breast tissue is assessed to exclude tumor recurrence (after mastectomy). Possible complications after gland replacement are also assessed. These are complications associated with violation of the surgical technique and complications associated with the reaction of breast tissue to the endoprosthesis as a foreign body. Ultrasound can reveal: changes in the position of the endoprosthesis, compaction of the prosthesis capsule, inflammation, hemorrhage, rupture of the implant wall with silicone leaking beyond the capsule.
Causes
A bend in the gall bladder can occur in any part of the organ.
A bend can occur in various parts of the gallbladder for a variety of reasons. The most dangerous thing is the bending of the body of the gallbladder, in which bile is released in fairly large quantities. Let's look at the main causes of gallbladder bending:
- Great physical activity. With physical exertion and regular lifting of weights, prolapse of internal organs can occur, which leads to kinking of the gallbladder with all the consequences.
- Obesity. Obesity has a detrimental effect on many internal organs. They become covered with fat, become deformed, and shift. The gallbladder is no exception. A kink in the gallbladder is not the worst thing that can happen with severe obesity, but its consequences are noticeable.
- Congenital pathology. This is perhaps the most common cause of a bent gallbladder. During the formation of the internal organs of the embryo, a disturbance in the proportion of growth and size of the organs may occur. In this case, the liver and gall bladder are subject to deformation. Such changes can last a lifetime.
- Pregnancy. During pregnancy, the uterus grows and puts pressure on the internal organs. The liver and gallbladder may also suffer from this. Then a temporary bend of the gallbladder is formed, which is subject to restoration after childbirth. However, this is rare. Most often, the bend is congenital, but makes itself felt only during pregnancy.
- Poor nutrition. Alternating fasting with overeating leads to increased production of pancreatic juice and stagnation of bile.
- Age-related changes. With age, internal organs prolapse, which leads to kinking of the gallbladder, age-related constipation and other diseases.
- Atypical location of the gallbladder. In addition to congenital deformation of the gallbladder, it may also have an atypical location relative to the liver. In this case, the gallbladder becomes more mobile and prone to kinks and stagnation of bile.
Ultrasound of gallbladder polyps. Part one
Authors: G. Cocco, R. Basilico, A. Delli Pizzi, N. Cocco, A. Boccatonda, D. D'Ardes, S. Fabiani, N. Anzoletti, P. D'Alessandro, G. Vallone, F. Cipollone , C. Schiavone
Gallbladder polyps are raised areas of the gallbladder wall that protrude into the lumen. They are discovered incidentally during abdominal ultrasound or after cholecystectomy, with an estimated prevalence of up to 9.5% of patients. Gallbladder polyps are motionless and do not have a posterior acoustic shadow. They can be sessile or on legs.
A systematic review by Elmasry et al. classified gallbladder polyps into pseudopolyps and true polyps. Pseudopolyps are benign and include cholesterosis, cholesterol polyps, inflammatory polyps, and localized adenomyomatosis.
True gallbladder polyps can be benign or malignant. Benign polyps are most often adenomas, and malignant polyps are adenocarcinomas and metastases. In addition, there are rare types of benign and malignant gallbladder polyps, such as mesenchymal tumors and lymphomas.
In this graphical review, we briefly recall the normal anatomy and function of the gallbladder, describe the normal ultrasound anatomy, and point out the wide range of pathologic abnormalities of the gallbladder wall. This review is based on the cumulative experience of our centers with a thorough review of the literature over the past 18 years (2001–2019). A systematic literature search was conducted in PubMed and included original studies and review articles focusing on sonographic descriptions of gallbladder polyps and associated diseases.
The gallbladder is a hollow, pear-shaped internal organ, ~7-10 cm long and ~2.5-3.5 cm wide, with thin and regular walls. It is located in the fossa of the gallbladder between the IV and V segments of the liver, which is an area devoid of visceral peritoneum.
The gallbladder consists of three parts: infundibulum, body and fundus (Fig. 1). Its function is to store bile volume (bile), usually 30–50 ml. When food enters the small intestine, a hormone called cholecystokinin is released, which signals the gallbladder to contract and release bile into the small intestine through the common bile duct. The gallbladder acts as a reservoir that stores bile during fasting, releasing it into the initial tract of the small intestine after eating to aid the digestive process, especially by breaking down fats.
According to some authors, the upper limit of normality for the thickness of the gallbladder wall is 4 mm. The thickness of the parietal surface of the gallbladder may exceed this limit if the patient is not fasting due to contraction of the smooth muscles of the organ or for certain pathological reasons, including inflammatory, neoplastic and systemic pathologies. These pathologies can be differentiated using a combined assessment of clinical findings and imaging findings.
Figure 1 : Sonographic image shows an image of the gallbladder: infundibulum, body and fundus (white arrows).
Ultrasound provides optimal imaging of the entire gallbladder (infundibulum, body and fundus). Conventional transabdominal ultrasound imaging using low-frequency transducers shows one or two layers of the gallbladder wall (Fig. 2a, b).
High-resolution sonography (HRUS), using high-frequency transducers, shows the three layers of the gallbladder wall, including the innermost hyperechoic layer, the middle thin hypoechoic layer, and the outermost hyperechoic layer. The innermost layer corresponds to the mucosa, is linear, echogenic and has a regular surface; the middle layer corresponds to the muscle layer, thin and slightly hypoechoic; and the outermost layer corresponds to the serosa of the organ and is linear, echogenic and regular (Fig. 3).
Figure 2 : Conventional transabdominal ultrasound image using a convex probe (1–5 MHz) shows a single layer (white arrow). b Conventional transabdominal ultrasound image using a convex probe (1–5 MHz) shows two layers of the gallbladder wall (white arrows)
Figure 3 : A linear transducer using high frequency transducers can better visualize the layers of the gallbladder wall. The image shows the three layers of the gallbladder wall, including the innermost hyperechoic layer (white arrow), the middle thin hypoechoic layer (red arrow), and the outermost hyperechoic layer (yellow arrow).
Optimal sonography of the gallbladder should be performed with the patient fasting (about 6–8 hours) using convex (2–8 MHz) and linear (3–13 MHz) transducers. The examination should be optimized to obtain appropriate B-mode images and be performed using systematic scanning using subcostal and intercostal approaches, as well as longitudinal and transverse images of the organ. The anatomy (shape, size, wall thickness, regularity and structure of the gallbladder walls) and contents should be assessed.
Fine deposits of bile sludge can mimic gallbladder wall polyps (Fig. 4a). It is useful to perform dynamic ultrasound of the gallbladder, changing the position of the patient. The polyps will remain fixed as the bile sludge breaks away from the wall (Fig. 4b).
Gallbladder sonography should be combined with color and power Doppler. When using color Doppler mode, the clinician should set the device to low PRF values and optimize color gain to evaluate the flow of small vessels in the gallbladder wall, which is characterized by low velocities. Currently, ultrasound machines are equipped with special settings for slow vascular flows. For example, ultrasound machine CHISON QBIT 5.
Figure 4 :a Ultrasound images show fine deposits of bile sludge that may mimic gallbladder wall polyps (white arrows). b It is useful to perform dynamic ultrasound of the gallbladder by changing the position of the patient (green arrow)
High-resolution ultrasound (HRUS) uses low- and high-frequency transducers to evaluate the gallbladder. Because high frequency has better resolution, HRUS can better evaluate the layers of the gallbladder wall and more accurately analyze changes in the internal echo of polyps compared with traditional transabdominal sonography. Although data in the literature are still limited, HRUS appears to provide successful performance in the evaluation of gallbladder cancer and in differentiating gallbladder cancer from adenomyomatosis.
3D ultrasound is a progressive method for diagnosing the gallbladder. A study conducted on 80 patients with gallbladder polyps showed that diagnosis agreement was achieved in 89% of cases when 2D and 3D ultrasound were used. However, 3D ultrasound showed poorer diagnostic performance when detecting polyps smaller than 4 mm.
Contrast-enhanced ultrasound (CEUS) is a promising tool for improving diagnostic accuracy in the detection and evaluation of gallbladder diseases. Numata et al. used galactose and palmitic acid contrast injection to evaluate polyps by analyzing criteria for tumor enlargement and tortuous tumor vessels; this method demonstrated 91% accuracy in diagnosing malignant neoplasms. Other studies have shown a limitation associated with lesion size, as diagnostic accuracy was higher for polyps larger than 10 mm.
Cholesterolosis is the most common pseudopolyp. It is asymptomatic and may be isolated or associated with gallstones. Cholesterolosis is usually diagnosed incidentally during sonography. This condition results from abnormal deposition of lipids (triglycerides, cholesterol precursors and cholesterol esters) in the lining of the gallbladder.
DO YOU CARE CORRECTLY FOR YOUR ULTRASOUND DEVICE?
Download your care guide now
Download PDF
During sonography, cholesterolosis appears as parietal hyperechoic single or multiple lesions on the gallbladder wall, generating comet-tail artifacts on B-mode and flickering artifacts on color Doppler.
The comet tail artifact is a form of reverberation (Fig. 5a). In this artifact, two reflective interfaces and serial echoes are located close to each other. The result is an artifact caused by the reverberation principle, but with a triangular, tapering shape. Flicker artifacts on color Doppler ultrasound arise from the interaction of the ultrasound beam with a rough acoustic boundary consisting of randomly arranged highly reflective media such as cholesterol crystals or calcification (Fig. 5b).
Figure 5 : Ultrasound image shows multiple parietal hyperechoic lesions on the gallbladder body and infundibulum wall generating comet-tail artifacts in B-mode (white arrows). b Ultrasound image shows multiple parietal hyperechoic lesions on the body of the gallbladder, producing flickering artifacts on color Doppler (yellow arrows).
Cholesterol polyps are a polypoid variant of cholesterolosis in which deposits result in the formation of single or multiple cholesterol polyps that are attached to the underlying mucosa by a fragile epithelial stalk composed of lipid-filled macrophages. These polyps can break off, leading to complications similar to those that occur with small gallstones.
On sonography, cholesterol polyps usually appear as multiple lesions, homogeneous, pedunculated, and smaller than 1 cm; polyps are usually more hyperechoic than liver parenchyma (Fig. 6 a, b).
Figure 6 : a Ultrasound image shows single cholesterol polyps, homogeneous, pedunculated, without posterior acoustic shadow, less than 1 cm in size, more hyperechoic than the liver parenchyma (white arrow). b Sonographic image shows two cholesterol polyps, homogeneous, pedunculated, without posterior acoustic shadow, less than 1 cm in size, more hyperechoic than the liver parenchyma (white arrows)
Inflammatory polyps are the least common type of pseudopolyp, accounting for about 10% of gallbladder polyps. They represent local epithelial proliferations of inflammatory reactions with infiltration of inflammatory cells and are often associated with chronic cholecystitis.
On ultrasound examination, inflammatory polyps are often characterized by higher echogenicity than liver parenchyma and are homogeneous, sessile or pedunculated (Fig. 7), difficult to distinguish from cholesterol polyps. Although inflammatory polyps larger than 1 cm have been described, they are usually less than 10 mm in diameter. It is noteworthy that large inflammatory polyps can be confused with true gallbladder polyps.
Figure 7 : Sonographic image shows an inflammatory polyp (white arrow) that has a higher echogenicity than the liver parenchyma, is homogeneous, pedunculated, and less than 10 mm in diameter.
Typically, the differential diagnosis of cholesterol and inflammatory polyps is made histologically, and for this reason CEUS is not usually used. These lesions usually appear homogeneous, slightly hyperechoic in the arterial phase, and are surrounded by normal tissue.
Source
Treatment of gallbladder inflection
Gallbladder: schematic representation of organ placement
Treatment is prescribed individually and only by the attending physician. Self-medication is not recommended. Before this, it is necessary to undergo diagnostics, identify the causes of the bend in the gallbladder, specify the location of the bend, only after an ultrasound and tests the doctor will prescribe treatment:
- Choleretic drugs. If the gallbladder is bent, choleretic drugs are prescribed to improve the flow of bile into the intestinal lumen. Similar drugs include Hofitol, Allohol. A drug called Aristochol contains medicinal herbs and acts in several directions at once: improves intestinal function, increases the flow of bile and relieves spasms.
- Painkillers and antispasmodics. For pain, the doctor prescribes painkillers and antispasmodics, such as Drotaverine, No-Shpa, Baralgin. For nausea and vomiting, intramuscular injections are possible.
- Antibiotics. The doctor may prescribe antibiotics for cholecystitis, if the gallbladder is bent due to an infection that provokes inflammation of the gallbladder mucosa. Ampiox is often prescribed.
- Physical procedures. Physiotherapy is most often aimed at warming up: ozokerite therapy, paraffin therapy.
- Breathing exercises. The abdominal type of breathing is useful, when with each inhalation the diaphragm and abdominal organs develop. This will help avoid bile stagnation.
- Vitamin therapy. Vitamins will help strengthen the general condition of the body, increase immunity, which is especially important when there is an excess caused by infection.
- Traditional medicine. Choleretic herbs include milk thistle, tansy, and immortelle. Tansy decoction also has an analgesic effect. It is also recommended to take a decoction of rose hips, valerian, chamomile with mint, and hop cones. For gallbladder diseases, it is sometimes recommended to eat mustard, horseradish and garlic with other foods. However, you need to be careful with this, since such products are contraindicated for other diseases of the digestive system.