Mandatory diagnostic procedures during pregnancy include ultrasound. This examination has no contraindications and is very informative: it helps to identify pathologies of fetal development, assess the condition of amniotic structures, and if complications are detected, make a decision regarding the further course of pregnancy.
Negative effect on fetal development
provide:
- mature age of parents (mothers - from 35 years, fathers - from 40 years);
- burdened heredity;
- constant contact with harmful chemicals;
- unfavorable environmental conditions;
- smoking, drinking alcohol;
- taking a number of medications;
- unstable psycho-emotional background;
- transferred (especially in the first semester) rubella, influenza, hepatitis B, toxoplasmosis, STDs.
Most of these risks can be avoided if you plan your pregnancy in advance. During the preparation, future parents undergo a comprehensive examination, based on the results of which (if necessary) treatment for detected disorders is prescribed.
Causes of congenital fetal pathology
What factors can adversely affect the fetus?
The causes of various pathologies are:
- burdened heredity;
- Mom's age is over 35 years, dad's age is over 40;
- unfavorable environmental conditions;
- working with toxic substances;
- bad habits - alcohol abuse, smoking, drug use;
- viral and bacterial diseases, especially in the first trimester - influenza, rubella, toxoplasmosis, hepatitis B, sexually transmitted diseases;
- taking certain medications;
- excessive psycho-emotional stress.
The more factors are present, the greater the likelihood of fetal pathologies. That is why you need to start planning for the birth of a child in advance, at least six months before conception. This time is enough to undergo a comprehensive examination, identify and cure diseases, and prepare for the conception of a healthy baby. To highlight the impact of bad habits on the fetus, we present some numbers.
With maternal alcoholism, toxicosis is observed in 26% of cases, antenatal death and asphyxia in 12%, miscarriages in 22%, premature birth in 34%, birth injuries in 8%, and intrauterine growth retardation in 19%.
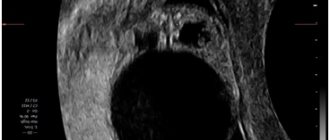
Dilatation of intestinal loops in the fetus
Let's decipher the ultrasound results. With what trepidation every pregnant woman awaits the next ultrasound examination! She wants to see the baby, find out if he is okay in the womb, see his arms and legs, see if his heart is beating. But the expectation of a miracle is often not justified. During the study, the expectant mother sees a screen with black and white dots and sticks, and at the end of the study she sees a conclusion on paper with incomprehensible numbers and phrases. Let's figure out what is written in this conclusion. First, about when and why an expectant mother needs to go for research. Indications for ultrasound examination can be divided into screening and selective. Screening is an examination of all pregnant women without exception at a certain time. These studies are carried out primarily to determine whether there are any malformations in the fetus. During the examination, the fetus is measured, it is determined whether the size of the fetus corresponds to the expected period of pregnancy, and the uterus and placenta are examined. Such screening studies are usually carried out 3-4 times during pregnancy: at 10-14 weeks, at 20-24 weeks, at 30-32 weeks and at the end of pregnancy - at 36-37 weeks. Selective studies are carried out if any problem or complication is suspected. Since the need for such studies is dictated by suspected pathology, their number is not limited. In some cases, ultrasound is performed 2-3 times a week. Condition of the fetus. During the first study, it is determined where the fetus is located, thus excluding the ectopic location of the ovum. Later, the position of the fetus in the uterus is determined - cephalic or pelvic. At the time of the first study, the thickness of the collar zone is determined. Judging by the name, it is clear that this is an area located in the collar area - on the back of the neck. There are certain sizes that must meet certain parameters. An increase in the size of the collar zone is a reason for genetic consultation, as it is a sign of fetal malformations. In the second and third trimesters of pregnancy, ultrasound examinations may reveal signs of fetal infection, including changes in the structure of the brain. In the third trimester, the structures of the fetal lungs are assessed; this is necessary to determine the degree of maturity of the lungs if premature birth is suspected or necessary. The structure of the lungs is also studied to exclude intrauterine pneumonia. All internal organs of the fetus (heart, intestines, liver, etc.) are carefully studied. During the examination, especially carried out in the second trimester of pregnancy, it is possible to examine the fetal facial skull and nose to diagnose defects such as cleft palate and cleft lip. It is also possible to diagnose the pathology of tooth formation. Most expectant parents are interested in the question of whether Down syndrome can be detected using ultrasound. I would like to note that it is very difficult to make this diagnosis based only on ultrasound data. Down syndrome for up to 14 weeks suggests an increase in the nuchal zone (for example, at 7-8 weeks of pregnancy, the nuchal zone should be no more than 3 mm), and the absence of the nasal bridge. Indirect signs are an increase in the interorbital distance, an open mouth, a protruding tongue and some other signs. In 1/3 of cases of Down's disease, heart defects are detected, more often in the form of ventricular septal defects. Shortening of the lower leg bones may also be noted. If these signs are detected, placentocentesis is performed - a study during which a piece of the placenta is taken. The chromosomal set of cells is studied in the obtained material. The ultrasound examination report reflects information about the size of the collar zone in the first trimester of pregnancy. If no pathology is found during the examination of internal organs, then this may be noted in a separate phrase or not reflected in any way, however, if certain problems are detected, the data must be entered into the study protocol. In most cases, during an ultrasound examination performed at 12 and 22 weeks, it is possible to determine the sex of the child. These data are not included in the study protocol. Already from the first study, the fetal heartbeat can be determined. The documentation records the presence of a heartbeat (s/b +), heart rate - the number of heart contractions (normal heart rate is 120-160 beats per minute). A deviation in heart rate during the first study - an increase or decrease in the number of heartbeats - may be a sign that the newly born fetus has a heart defect. Later, in the second and third trimesters, it is possible to distinguish and study the heart valves and chambers in detail. A change in the number of heartbeats in the second and third trimester may indicate fetal suffering, lack of oxygen and nutrients. Fruit size. Abbreviations that can be found in ultrasound examination protocols have the following meanings. In the first trimester of pregnancy, the diameter of the ovum (DPR) and the coccygeal-parietal size of the fetus (CTR), that is, the size from the crown to the coccyx, are determined. The size of the uterus is also measured. These measurements make it possible to judge the gestational age quite accurately in the first trimester, since at this time the size of the fetus is most standard. There is a slight nuance regarding determining the gestational age based on the size of the fetus and ovum. In the conclusion, they may record not the obstetric period, calculated from the first day of the last menstruation, according to which the pregnancy lasts 40 weeks, but the gestational period from conception - the embryonic period. The gestational age from conception is 2 weeks less than the obstetric period. However, if the expectant mother compares the results of the ultrasound and the results of the examination, she may be perplexed, since the gestational age according to different sources may differ by 2 weeks. By checking with your doctor what period is indicated in the conclusion of the first ultrasound, you will resolve your doubts. In subsequent studies, in the second and third trimesters of pregnancy, the following indicators of fetal development are determined: * BPR - biparietal size - the size between the temporal bones, * LZR - fronto-occipital size, * OG - head circumference, * OB - abdominal circumference. They also measure the length of the femur, humerus, and it is possible to measure the smaller bones of the forearm and tibia. If the size of the fetus is smaller than expected at this stage of pregnancy, then they speak of IUGR - intrauterine growth restriction of the fetus. There are asymmetric and symmetric forms of VZRP. An asymmetrical shape is said to be when the dimensions of the head and limbs correspond to the period, and the dimensions of the body are less than the expected period of pregnancy. With a symmetrical form of fetal growth retardation, all sizes are reduced equally. With an asymmetric form of IUGR, the prognosis is more favorable than with a symmetric one. In any case, if intrauterine growth restriction is suspected, medications are prescribed to improve the supply of nutrients to the fetus. This treatment is carried out for 7-14 days, after which a repeat ultrasound examination is required. In case of fetal growth retardation, a cardiotocographic study is prescribed - a procedure during which the fetal heartbeat is recorded using a special apparatus, as well as a Doppler study, which is used to determine the blood flow in the vessels of the fetus, umbilical cord, and uterus. Doppler examination is performed at the time of ultrasound. If the degree of fetal growth retardation is large - if the size of the fetus is reduced by more than 2 weeks than the expected period, or malnutrition (fetal growth retardation) is detected early - in the second trimester of pregnancy, then treatment is certainly carried out in a hospital.
At-risk groups
Taking into account the causes of fetal pathologies, scientists have identified risk groups. Women from these groups come under the close attention of doctors due to the high likelihood of developing anomalies.
These include:
- women over 35 years of age;
- patients who already have children with congenital pathology;
- women with a history of miscarriage, premature birth, stillbirth or antenatal fetal death;
- couples with a family history;
- patients exposed to radiation or exposed to toxins at work.
In such cases, ultrasound is performed repeatedly - the doctor needs to examine the fetus in detail, evaluate its development over time in order to exclude congenital anomalies.
Various genetic tests are also carried out for the timely detection of pathologies.
Transverse position of the fetus
At up to 34–35 weeks of gestation, the oblique or transverse position of the fetus is considered unstable, since it can independently change to longitudinal. When diagnosing the transverse position of the fetus, a complete gynecological examination of the pregnant woman is required to identify the causes of the anomaly, choose tactics for further pregnancy management and the method of delivery.
At 30-34 weeks of pregnancy, corrective gymnastics may be prescribed to help turn the fetus into a cephalic presentation. Special sets of exercises are indicated in the absence of signs of a threatened miscarriage, uterine scar, fibroids, bleeding, decompensated heart defects in a pregnant woman, etc. and are carried out under the supervision of an obstetrician-gynecologist observing the woman. Also, if the fetus is in a transverse position, it is recommended that the pregnant woman lie more time on her side, corresponding to the position being determined.
After 35-36 weeks of gestation, the fetus assumes a stable position, therefore, while maintaining the transverse position, the pregnant woman is hospitalized in the maternity hospital to determine delivery tactics.
The method of external rotation to the head - changing the transverse position of the fetus using external techniques is currently practically not used. This is due to the low efficiency of rotation, since if the reasons are not eliminated, the fetus often returns to a transverse position. In some cases, external rotation can result in serious consequences: placental abruption, uterine rupture, fetal hypoxia.
The optimal method of delivery for patients with a transverse fetal position is a planned cesarean section. Absolute indications for surgical delivery are post-term pregnancy, the presence of placenta previa, premature rupture of amniotic fluid, scars on the uterus, and the development of fetal hypoxia. If the fetus is in an advanced transverse position with prolapse of its arm or umbilical cord, it is unacceptable to reposition the prolapsed parts.
In the case of complete dilatation of the cervix, the fetus is determined to be alive and is mobile, it is possible to rotate the fetus onto its stem and then extract it. However, the prognosis for the fetus in this case is less favorable. Rotation and natural childbirth are justified in case of prematurity or twin births, when one fetus occupies a transverse position.
In the situation of a long anhydrous interval, complicated by the development of an infectious process, and the viability of the fetus after a cesarean section, a hysterectomy (removal of the uterus) and drainage of the abdominal cavity are performed. If the fetus is dead, a fetal-destroying embryotomy operation is performed.
Fetal malformations that are visible on ultrasound
Developmental pathologies include:
- abnormalities in the development of the neural tube - absence of the cerebral hemispheres, hydrocephalus, cerebral herniation, microcephaly;
- spinal defects - myelomeningocele, spina bifida, cystic hygroma;
- heart pathologies - abnormal position of the heart, underdevelopment of the organ, ventricular septal defect;
- anomalies of the gastrointestinal tract - atresia of the cardia, duodenum, jejunum;
- malformations of the anterior abdominal wall - omphalocele, gastroschisis, ascites in the fetus;
- congenital kidney anomalies - underdevelopment, urinary tract obstruction, polycystic disease;
- pathologies of the amount of amniotic fluid - oligohydramnios, polyhydramnios;
- intrauterine fetal death.
Neural tube malformations
- Anencephaly is a pathological condition characterized by the congenital absence of the cranial vault and cerebral hemispheres. This is the most common pathology of the central nervous system in the fetus. It is diagnosed at 11-12 weeks. As a rule, the defect is combined with hydramnios and other disorders. The level of alpha-fetoprotein in the mother's blood increases.
- Signs of hydrocephalus in the form of expansion of the anterior and posterior horns of the lateral ventricles will be visible at 18 weeks of pregnancy.
- Microcephaly - a pathological reduction of the fetal head - occurs when the biparietal size decreases by more than three standard deviations. To rule out intrauterine growth retardation, the doctor will compare the size of the head with the size of the body of the unborn child. In isolated form, the defect is rare, and in borderline cases, the diagnosis is quite difficult to make. In this regard, the woman is recommended to undergo an ultrasound again in a few weeks. The data obtained are interpreted quite carefully, especially if the fetus grows and develops normally.
- Encephalomeningocele usually appears as a rounded protrusion in the area of the calvarial bones. Inside the protrusion is fluid or brain matter. Most often, anomalies are localized at the back of the head, but sometimes anterior localization of the defect occurs. To minimize the likelihood of diagnostic error, if an encephalomeningocele is suspected, the woman will be advised to undergo a repeat ultrasound, possibly from a different doctor.
Anomalies of the spine
Most often, fetal pathologies in the form of anomalies in the development of the spine are localized in the cervical and lumbar region. Since the spine is clearly visualized from the 15th week of pregnancy, its defects are diagnosed at 18-20 weeks, during the second screening ultrasound.
- Myelomeningocele on ultrasound is visualized as a sac containing fluid and elements of the spinal cord. In rare cases, an open defect is diagnosed, in which only protrusion of soft tissue through the defect is detected. Such anomalies are particularly difficult to detect.
- Spina bifida in the fetus is diagnosed using expert-class, high-resolution ultrasound machines. Normally, the posterior ossification centers of the spine are visualized as two hyperechoic, almost parallel structures. In spina bifida they are displaced laterally.
- Cystic hygroma is a pathology of the development of the lymphatic system. In this case, an ultrasound reveals a cyst with septa located in the cervical spine. Sometimes internal partitions are visible, resembling the spokes of a wheel. The skull, brain and spinal cord, unlike other anomalies, develop normally. Sometimes cystic hygroma is combined with a generalized anomaly of the lymphatic system. In most such cases, the fetus dies.
Congenital heart defects
Diagnosis of congenital heart defects requires special equipment. The doctor should be able to perform Doppler ultrasound. If congenital heart defects are suspected, an expert opinion is required. In difficult cases, clinicians are warned about possible complications so that they are ready to provide specialized care at the birth of the child.
Anomalies of the development of the gastrointestinal tract
The most common pathology of the development of the digestive tract is duodenal atresia. In this case, on an ultrasound, the doctor sees round structures similar to cysts in the upper part of the fetal abdomen. If the cyst is located on the left, it is an enlarged stomach, on the right - the duodenum. This is the so-called “double bubble” sign. Very often the pathology is combined with polyhydramnios, anomalies of the heart, kidneys, and central nervous system.
Diagnosis of small bowel atresia is difficult. In the upper part of the fetal abdomen, the doctor sees cystic structures - overstretched loops of the small intestine. As a rule, fetal pathology is detected in the middle of pregnancy or at a later stage. With high atresia, polyhydramnios is usually diagnosed. Colonic atresia is almost impossible to diagnose using ultrasound.
Pathology of development of the anterior abdominal wall
The most commonly diagnosed defect in this group is an anterior abdominal wall defect - omphalocele. In the hernial sac, formed by the amniotic membrane and the parietal peritoneum, intestinal loops, part of the liver, stomach and spleen are found.
Other pathology is mainly localized in the right periumbilical region (gastroschisis) and is usually isolated. Only intestinal loops that are not covered by the amniotic membrane prolapse through this defect.
Ascites in the fetus
Free fluid is visualized on ultrasound as an anechoic zone surrounding the internal organs of the unborn child. If ascites is suspected, the doctor must carefully examine the fetus and evaluate its anatomy to exclude combined defects. The urinary system must be carefully examined, as ascitic fluid may be urine. If the unborn child has thickened skin or fluid is contained in at least two natural cavities, they speak of hydrops fetalis.
Its reasons are:
- Rhesus conflict;
- congenital heart defects;
- arrhythmias;
- obstruction of blood or lymphatic vessels.
To find out the exact cause of dropsy, the doctor will recommend an additional expert ultrasound to the woman.
Abnormalities of the urinary system
Some congenital defects of the urinary system are incompatible with life. If such a pathology is detected in the early stages, the doctor may advise the woman to terminate the pregnancy. If the anomaly was diagnosed late, the doctor may change the pregnancy management tactics.
Diagnosing agenesis, or absence of kidneys, is difficult due to the significant enlargement of the adrenal glands. In the last weeks of pregnancy, these glands can take on a bean-shaped shape, which makes diagnosis even more difficult. The bladder is small or absent altogether. To make an accurate diagnosis, you need to examine the fetus in several planes. Measuring the kidneys during an ultrasound helps to identify hypoplasia - underdevelopment of the organ.
Obstruction, hydronephrosis is manifested by dilation of the renal pelvis. However, it must be borne in mind that the expansion of the renal pelvis may be transient. Such dilations are most often bilateral and disappear after some time. If hydronephrosis is suspected, an ultrasound scan should be repeated after two to three weeks.
Pathological bilateral obstruction of the urinary system is usually combined with oligohydramnios and has a poor prognosis. If the obstruction is unilateral, the amount of amniotic fluid remains within normal limits.
With a multicystic kidney, ultrasound will reveal several cysts of varying diameters. They are located diffusely, less often in one part of the organ. Renal parenchyma can be detected between the cysts, although it is not clearly visualized. Autosomal recessive polycystic kidney disease is diagnosed in the third trimester of pregnancy. In such situations, there is a family history and oligohydramnios. On ultrasound, the kidneys are enlarged in size and their echogenicity is sharply increased.
Amniotic fluid
The most common causes of polyhydramnios are:
- high obstruction of the digestive tract;
- neural tube pathology;
- hydrops fetalis;
- defects of the anterior abdominal wall;
- skeletal dysplasia of the chest;
- development of several embryos simultaneously;
- diabetes mellitus in the mother.
The causes of oligohydramnios are:
- bilateral renal anomaly;
- damage to the amniotic membranes with leakage of water;
- intrauterine growth retardation;
- post-term pregnancy;
- antenatal fetal death;
- intrauterine developmental delay;
- post-term pregnancy;
- intrauterine embryonic death.
Oligohydramnios with bilateral renal anomalies is a poor prognostic sign.
fetal intestinal loops are dilated
Let's decipher the ultrasound results. With what trepidation every pregnant woman awaits the next ultrasound examination! She wants to see the baby, find out if he is okay in the womb, see his arms and legs, see if his heart is beating. But the expectation of a miracle is often not justified. During the study, the expectant mother sees a screen with black and white dots and sticks, and at the end of the study, a conclusion on paper with incomprehensible numbers and phrases. Let's figure out what is written in this conclusion. First, about when and why an expectant mother needs to go for research. Indications for ultrasound examination can be divided into screening and selective. Screening is an examination of all pregnant women without exception at a certain time. These studies are carried out primarily to determine whether there are any malformations in the fetus. During the examination, the fetus is measured, it is determined whether the size of the fetus corresponds to the expected period of pregnancy, and the uterus and placenta are examined. Such screening studies are usually carried out 3-4 times during pregnancy: at 10-14 weeks, at 20-24 weeks, at 30-32 weeks and at the end of pregnancy - at 36-37 weeks. Selective studies are carried out if any problem or complication is suspected. Since the need for such studies is dictated by suspected pathology, their number is not limited. In some cases, ultrasound is performed 2-3 times a week. Condition of the fetus. During the first study, it is determined where the fetus is located, thus excluding the ectopic location of the ovum. Later, the position of the fetus in the uterus is determined - cephalic or pelvic. At the time of the first study, the thickness of the collar zone is determined. Judging by the name, it is clear that this is an area located in the collar area - on the back of the neck. There are certain sizes that must meet certain parameters. An increase in the size of the collar zone is a reason for genetic consultation, as it is a sign of fetal malformations. In the second and third trimesters of pregnancy, ultrasound examinations may reveal signs of fetal infection, including changes in the structure of the brain. In the third trimester, the structures of the fetal lungs are assessed; this is necessary to determine the degree of maturity of the lungs if premature birth is suspected or necessary. The structure of the lungs is also studied to exclude intrauterine pneumonia. All internal organs of the fetus (heart, intestines, liver, etc.) are carefully studied. During the study, especially carried out in the second trimester of pregnancy, it is possible to examine the fetal facial skull and nose to diagnose defects such as cleft palate and cleft lip. It is also possible to diagnose the pathology of tooth formation. Most expectant parents are interested in the question of whether Down syndrome can be detected using ultrasound. I would like to note that it is very difficult to make this diagnosis based only on ultrasound data. Down syndrome for up to 14 weeks suggests an increase in the nuchal zone (for example, at 7-8 weeks of pregnancy, the nuchal zone should be no more than 3 mm), and the absence of the nasal bridge. Indirect signs are an increase in the interorbital distance, an open mouth, a protruding tongue and some other signs. In 1/3 of cases of Down's disease, heart defects are detected, more often in the form of ventricular septal defects. Shortening of the lower leg bones may also be noted. If these signs are detected, placentocentesis is performed - a study during which a piece of the placenta is taken. The chromosomal set of cells is studied in the obtained material. The ultrasound examination report reflects information about the size of the collar zone in the first trimester of pregnancy. If no pathology is found during the examination of internal organs, then this may be noted in a separate phrase or not reflected in any way, however, if certain problems are detected, the data must be entered into the study protocol. In most cases, during an ultrasound examination performed at 12 and 22 weeks, it is possible to determine the sex of the child. These data are not included in the study protocol. Already from the first study, the fetal heartbeat can be determined. The documentation records the presence of a heartbeat (s/b +), heart rate - the number of heart contractions (normal heart rate is 120-160 beats per minute). A deviation in heart rate during the first study - an increase or decrease in the number of heartbeats - may be a sign that the newly born fetus has a heart defect. Later, in the second and third trimesters, it is possible to distinguish and study the heart valves and chambers in detail. A change in the number of heartbeats in the second and third trimester may indicate fetal suffering, lack of oxygen and nutrients. Fruit size. Abbreviations that can be found in ultrasound examination protocols have the following meanings. In the first trimester of pregnancy, the diameter of the ovum (DPR) and the coccygeal-parietal size of the fetus (CTR), that is, the size from the crown to the coccyx, are determined. The size of the uterus is also measured. These measurements make it possible to judge the gestational age quite accurately in the first trimester, since at this time the size of the fetus is most standard. There is a slight nuance regarding determining the gestational age based on the size of the fetus and ovum. In the conclusion, they may record not the obstetric period, calculated from the first day of the last menstruation, according to which the pregnancy lasts 40 weeks, but the gestational period from conception - the embryonic period. The gestational age from conception is 2 weeks less than the obstetric period. However, if the expectant mother compares the results of the ultrasound and the results of the examination, she may be perplexed, since the gestational age according to different sources may differ by 2 weeks. By checking with your doctor what period is indicated in the conclusion of the first ultrasound, you will resolve your doubts. In subsequent studies, in the second and third trimesters of pregnancy, the following indicators of fetal development are determined: * BPR - biparietal size - the size between the temporal bones, * LZR - fronto-occipital size, * OG - head circumference, * OB - abdominal circumference. They also measure the length of the femur, humerus, and it is possible to measure the smaller bones of the forearm and tibia. If the size of the fetus is smaller than expected at this stage of pregnancy, then they speak of IUGR - intrauterine growth retardation. There are asymmetric and symmetric forms of VZRP. An asymmetrical shape is said to be when the dimensions of the head and limbs correspond to the period, and the dimensions of the body are less than the expected period of pregnancy. With a symmetrical form of fetal growth retardation, all sizes are reduced equally. With an asymmetric form of IUGR, the prognosis is more favorable than with a symmetric one. In any case, if intrauterine growth restriction is suspected, medications are prescribed to improve the supply of nutrients to the fetus. This treatment is carried out for 7-14 days, after which a repeat ultrasound examination is required. In case of fetal growth retardation, a cardiotocographic study is prescribed - a procedure during which the fetal heartbeat is recorded using a special apparatus, as well as a Doppler study, which is used to determine the blood flow in the vessels of the fetus, umbilical cord, and uterus. Doppler examination is performed at the time of ultrasound. If the degree of fetal growth retardation is large - if the size of the fetus is reduced by more than 2 weeks than the expected period, or malnutrition (fetal growth retardation) is detected early - in the second trimester of pregnancy, then treatment is certainly carried out in a hospital.
Placenta. The placenta is finally formed by 16 weeks of pregnancy. Before this period, they talk about the chorion - the predecessor of the placenta. The chorion is the outer shell of the embryo, which performs protective and nutritional functions. During an ultrasound examination, the placenta is attached - on which wall of the uterus the chorion or placenta is located, how far the placenta is from the internal os of the cervix - the place of exit from the uterine cavity. In the third trimester of pregnancy, the distance from the placenta to the internal os of the cervix should be more than 6 cm, otherwise they speak of low placental attachment, and if the placenta covers the internal os, placenta previa. This condition is fraught with complications - bleeding during childbirth. Low attachment of the placenta is also noted during ultrasound examinations performed in the first and second trimesters, but until the third trimester the placenta can migrate, that is, rise up the wall of the uterus. During ultrasound examinations, the structure of the placenta is also assessed. There are four degrees of its maturity. Each degree corresponds to certain stages of pregnancy: the 2nd degree of maturity should last up to 32 weeks, the 3rd degree - up to 36 weeks. If the placenta changes structure ahead of schedule, they speak of premature aging of the placenta. This condition may be associated with impaired blood flow in the placenta caused by gestosis (a complication of pregnancy, manifested by increased blood pressure, the appearance of protein in the urine, edema), anemia (decreased hemoglobin amount), or may be an individual feature of the body of a given pregnant woman. Premature aging of the placenta is a reason for conducting Doppler ultrasound and cardiac monitoring studies. During an ultrasound examination, the thickness of the placenta is determined. Normally, up to 36 weeks of pregnancy, the thickness of the placenta is equal to the gestational age +/- 2 mm. From 36-37 weeks, the thickness of the placenta ranges from 26 to 45 mm, depending on individual characteristics. When the thickness and structure of the placenta changes, an assumption is made about placentitis - inflammation of the placenta. Conclusion Ultrasound “placentitis” is not an indication for hospitalization. If changes in the placenta are suspected, it is necessary to conduct a Doppler study, which confirms or refutes the assumption. Additional laboratory tests are also prescribed, in particular screening for sexually transmitted infections. According to an ultrasound examination, it is possible to confirm the assumption of placental abruption, the cause of which is bloody discharge from the genital tract at any stage of pregnancy. Areas of detachment are visible on the screen. All this information is reflected in the ultrasound protocol. Umbilical cord. The umbilical cord connects the placenta to the fetus. At the time of ultrasound examination, the number of vessels in the umbilical cord is determined (normally there are three). In 80% of pregnant women, the umbilical cord loops are located in the neck or pelvic end - that part of the fetus that is about to exit the uterus. The umbilical cord loops “fall” there under gravity. Umbilical cord entanglement in the fetal neck can only be diagnosed using Doppler ultrasound. And although umbilical cord entanglement is not the topic of this conversation, I would like to note that even the fact that the umbilical cord is entwined around the neck is not an indication for a cesarean section. Amniotic fluid. An ultrasound examination measures the amniotic index, which indicates the amount of water. The amniotic index (AI) is determined by dividing the uterus into quadrants by two perpendicular lines (transverse - at the level of the pregnant woman's navel, longitudinal - along the midline of the abdomen) and summing up the indicators obtained by measuring the largest vertical column of amniotic fluid in each quadrant. At 28 weeks, normal AI values are 12-20 cm, at 33 weeks – 10-20 cm. An increase in AI indicates polyhydramnios, a decrease indicates oligohydramnios. Significant polyhydramnios or oligohydramnios may indicate fetoplacental insufficiency - a violation of the blood supply to the placenta. An increase and decrease in water levels can also occur with other pathologies, but it also occurs in isolation. During the study, the absence or presence of foreign impurities - suspensions in the amniotic fluid - is also assessed. The presence of a suspension may be evidence of infection or post-term pregnancy, but the suspension may contain only vernix lubrication, which is normal. Uterus. During an ultrasound examination, the size of the uterus is measured, the walls of the uterus are examined for the presence or absence of myomatous nodes, and for increased tone of the muscle wall. The thickness of the uterine walls is also measured. It should be noted that the diagnosis of “threatened miscarriage” cannot be made only in accordance with ultrasound data; such a diagnosis is made only when clinical signs - pain in the lower abdomen, in the lower back - are combined with ultrasound, which include a decrease in the thickness of the lower uterine uterus. segment (muscles in the lower part of the uterus) less than 6 mm, spindle-shaped contractions of the muscles of the uterus (increase in the thickness of the uterine wall in one area or another), which indicate a contraction of one or another area of the muscles of the uterus. Mechanical pressure with a sensor increases the tone of the uterine wall. This can be detected at the time of the study, but in the absence of clinical manifestations (pain in the lower abdomen, lower back), the diagnosis of “threatened miscarriage” is not made, talking only about increased tone. During all studies, especially when there is a threat of miscarriage, the length of the cervix, the diameter of the cervix at the level of the internal os, and the condition of the cervical canal (open, closed) are measured. The length of the cervix normally during pregnancy should be 4-4.5 cm. Shortening of the cervix - in a primigravida up to 3 cm, and in a multigravida - up to 2 cm, the opening of the uterine pharynx allows a diagnosis of isthmic-cervical insufficiency, in which the cervix begins to open already at 16-18 weeks, unable to hold the developing pregnancy. So, we have listed many, but not all of the signs that are determined during an ultrasound examination. Often, one sign can indicate completely different pathological or physiological conditions, so only a specialist can evaluate the full ultrasound picture, and the treating doctor will compare the ultrasound data with the results of observations, complaints, tests, and other studies. This is the only way to draw the right conclusions. I would especially like to note that if there is a suspicion of an unfavorable course of pregnancy, for those women who previously, during previous pregnancies, experienced certain complications (fetal malformations, etc.), it is necessary to conduct an expert study - using progressive technology, and most importantly, a highly qualified specialist. Ultrasound placentography. It is necessary to evaluate: localization, size of the placenta, structure, presence of pathological changes. Determining the location of the placenta allows you to choose the optimal tactics for managing pregnancy and childbirth and predict some obstetric complications. A final idea of the location of the placenta can only be obtained in the third trimester of pregnancy. Establishment of placenta previa or low attachment of the placenta is possible with a moderately full bladder using standard longitudinal and a series of oblique sections. Placenta previa is characterized by the presence of placental tissue in the area of the internal os: complete - covers the internal os, moving from one wall to another, incomplete - the lower edge of the placenta reaches the internal os without blocking it. Low attachment of the placenta: the lower edge is less than 5 cm from the internal os in the second trimester of pregnancy and less than 7 cm in the third trimester Placenta dimensions. The area and volume of the placenta are the most objective indicators, but they are difficult to assess. In practice, the thickness of the placenta is measured. The thickness of the placenta is measured at the level of the umbilical cord. There are standard tables for placental thickness and gestational age. Criterion for thickening of the placenta: thickness more than 4.5 cm, with fetal hydrops, Rh conflict, diabetes mellitus, infectious process. Criterion for placental thinning: placental thickness up to 2 cm or less. Stages of placenta maturity: 0 tbsp. - up to 30 weeks. 1 tbsp. — 27 — 36 weeks. 2 tbsp. - 34 - 39 weeks. 3 tbsp. - after 37 weeks. Premature ripening of the placenta, criteria: 2 tbsp. up to 32 weeks and 3 tbsp up to 36 weeks. Delayed placental maturation: 0 - 1 tbsp. during full-term pregnancy. Premature abruption of a normally located placenta, ultrasound criteria: the presence of an echo-negative space between the wall of the uterus and the placenta (retroplacental hematoma). Visualization of the hematoma is possible only in 25% of cases. In the second half of pregnancy, small hematomas are detected only when they are localized on the anterior wall. Fresh hematoma is a liquid formation with a fine suspension, clear boundaries, increased sound conductivity. From the second - third day - an echogenic formation without clear contours with increased sound conductivity. Thus, it is definitely impossible to either make or remove the diagnosis of placental abruption. Placental infarctions are defined as irregularly shaped formations with clear hyperechoic outer contours and homogeneous hypoechoic contents in the placental parenchyma. Deposition of calcium and fibrin salts and intervillous thrombosis are visualized as formations of increased echogenicity with uneven contours. Placental cysts appear as single-chamber fluid formations. Tumors of the placenta: chorioangiomas are identified echographically as nodular formations of reduced echogenicity with a heterogeneous structure, the outer contours have clear boundaries, polyhydramnios in 25-30% of cases. Placental edema: detected with maternal Rh immunization, ABO conflict, diabetes mellitus, infection, fetal hydrops. Ultrasound signs include an increase in the thickness of the placenta by 30-100% or more, an increase in the echogenicity of the placenta tissue and increased sound conductivity. Anomalies in the development of the placenta occur in the form of: accessory lobe, ring-shaped placenta, fenestrated placenta. The umbilical cord in cross section contains 2 arteries and 1 vein. During ultrasound it is necessary to evaluate: * the place of attachment of the umbilical cord to the placenta, * the place of attachment of the umbilical cord to the anterior abdominal wall of the fetus, * the number of umbilical cord vessels. Attachment of the umbilical cord can be marginal, shell, or split. An anomaly of attachment of the umbilical cord to the fetus - omphalocele: the umbilical ring and the fetal part of the umbilical cord are expanded due to the internal organs, the free part of the umbilical cord extends from the top of the hernial sac. Syndrome of a single umbilical cord artery. In 20% it is combined with congenital malformation and chromosomal aberrations. Entanglement of the umbilical cord around the fetal neck: Ultrasound criteria - one or more loops of the umbilical cord on the near and far surface of the neck. Umbilical cord cysts: Ultrasound signs: anechoic formations that do not disrupt the flow of blood vessels. Amniotic fluid. Oligohydramnios, ultrasound signs: presence of 1 pocket of water with two perpendicular dimensions less than 1 cm (for full-term pregnancy); Polyhydramnios, ultrasound signs: the presence of more than 2 pockets of water with two perpendicular dimensions of more than 5 cm (for full-term pregnancy).