Intestinal obstruction in children is a common disorder that occurs among various age groups. The disease is an abnormal functioning of the gastrointestinal tract and is characterized by a violation of the movement of food particles or other intestinal contents through the rectum. Among reported cases, the disease is more often diagnosed in boys than in girls. The main age for the development of this pathology is the first year of life.
- Etiology
- Classification
- Symptoms
- Diagnostics
- Treatment
The disease can be either congenital or acquired. There may be several factors contributing to the formation - premature initiation of complementary feeding for infants, poor nutrition and lack of diet, individual structural features of this organ and the occurrence of inflammatory processes of various natures.
Clinical manifestations can occur in a seemingly completely healthy child. Symptoms are paroxysmal in nature and are expressed in significant pain, inability to defecate, attacks of vomiting and nausea. An increase in temperature is often observed.
Diagnostic measures consist of a whole range of tools and include a physical examination, laboratory and instrumental examinations. Treatment of such a disease in a child is carried out through the use of medications and surgical intervention.
Etiology
The predisposing causes of the disease depend on the age group of children. Intestinal obstruction in newborns is caused by:
- improper and early feeding of infants, before four months;
- lack of a normal diet in children of the first year of life;
- delayed introduction of complementary foods, as well as prolonged feeding with breast milk only;
- insufficient formation of the gastrointestinal tract;
- structural features of the gastrointestinal tract, in particular the intestines;
- congenital elongation of this organ, as well as a wide range of disorders during the period of intrauterine formation;
- the presence of intestinal diseases of an inflammatory nature.
In children over 2 years of age, among the sources of intestinal obstruction are:
- the formation of benign or malignant neoplasms;
- the presence of fecal stones - the masses harden due to a disturbance in the digestive process or a diet inappropriate for the age group;
- formation of polyps on the membrane;
- entry of a foreign body into the intestine, which leads to blockage of the lumen of this organ;
- the occurrence of adhesive or scar disease, as well as ailments of the genitourinary system;
- volvulus;
- complications after medical intervention;
- immobilization of the large or small intestine;
- intussusception is a condition during which the penetration of one part of the intestine into the lumen of another occurs.
Development of intestinal obstruction in children
In some cases, the cause of the formation of the disease may be the pathological effect of worms or other parasites.
Classification
Modern pediatric gastroenterology knows several types of intestinal obstruction in children. According to the nature of origin, the disease is divided into:
- congenital obstruction - occurs as a result of intrauterine pathologies in the development of the gastrointestinal tract in a child, which is why the baby experiences symptoms of the disease from the first days of life. To prevent the recurrence of the disorder, patients are advised to lead an active lifestyle and follow a healthy diet;
- acquired obstruction - the main source of its appearance is intussusception. This form, in turn, is divided into several types. It is diagnosed mainly in infants from the fourth month to one year of life. It differs in that the appearance of symptoms is abrupt and unexpected. In children over 2 years of age, the disease can occur, but is rare.
Acquired intestinal obstruction in children is divided into several types:
- mechanical - occurs due to tumors and fecal stones. In this case, there is a manifestation of severe, cramping pain and disruption of the circulatory process. This may lead to tissue death and peritonitis;
- dynamic - this type of disease develops against the background of previous injuries or operations;
- adhesive - based on the name, the pathology is provoked by the presence of adhesions and inflammation in the abdominal cavity. This is the most common form of this disease in children;
- obstructive;
- strangulation - the main reasons for its appearance are considered to be improper diet, increased intra-abdominal pressure, prolonged fasting, followed by congestion of the stomach.
According to the nature of the spread of the pathogenic process, the disease is divided into several forms:
- complete obstruction - often this type is formed as a result of congenital intestinal obstruction and operations designed to eliminate it;
- partial obstruction - differs in that the intestinal lumen is not completely closed. This type can be quite difficult to detect, which is why therapy begins at a later stage.
According to the nature of its course, intestinal obstruction in newborns and children under 2 years of age is divided into:
- acute - is a consequence of various gastrointestinal disorders, hernias and intestinal tumors. Develops to the terminal stage within 24 hours, which is why medical care should be provided as soon as possible after the onset of symptoms;
- chronic – characterized by a milder course. Children suffer from pain in the lower abdomen and constant constipation. The body gradually becomes exhausted.
Depending on the intussusception, acquired or congenital intestinal obstruction occurs:
- small intestinal;
- colonic;
- small-colic – in which part of the small intestine is introduced into the large intestine.
Intestinal obstruction in newborns
The occurrence of the syndrome in infants is associated either with impaired intestinal motility, or with the presence of some kind of mechanical obstacle. This condition can be fatal to infants.
Causes
The congenital process usually occurs due to abnormal size of the sigmoid colon or stenosis at its border. This condition causes delay and difficult passage of breast milk. As a result, about a week after the start of feeding, heavy regurgitation of undigested milk appears.
There may be other causes of intestinal obstruction:
- increased viscosity of feces. Usually this phenomenon occurs due to an incorrectly selected mixture or the characteristics of mother's milk. This is why during lactation it is extremely important for a woman to monitor her diet;
- a tumor that serves as a mechanical obstacle to the passage of chyme;
- worms and roundworms;
- adhesions;
- volvulus, hernia.
Symptoms
Difficulties in diagnosis are due to the fact that the child cannot describe his complaints. However, parents may be wary of the following signs:
- incessant crying that turns into screaming;
- refusal to feed;
- pulling the legs bent at the knees towards the tummy;
- colic;
- absence of feces for several days;
- lethargy;
- vomit;
- pallor;
- heavy sweating.
The first symptom of intestinal obstruction in newborns is an attack of abdominal pain. The mechanism for the development of this symptom is due to the fact that the intestines are trying to push through feces, but this is impossible due to a mechanical obstruction. Feces begin to accumulate and put pressure on the walls of the organ, thereby causing a painful outbreak.
The pain usually occurs in bursts of about ten minutes. If the pain syndrome has completely gone away, this is not a good sign, indicating the development of life-threatening complications. Another characteristic manifestation of CI is stool retention. If meconium is not passed within a few hours after birth, a pathology may be suspected.
With partial obstruction, thick and hard stool mixed with mucus and blood is observed. Foul-smelling diarrhea indicates the development of a bacterial infection. The accumulation of feces and gases in the intestinal lumen provokes bloating. Visually, you can pay attention to asymmetrical areas. This is due to the fact that the abdomen swells only in those areas where there is no patency.
It is also worth noting another sign of pathology – vomiting. It occurs some time after feeding. Typical regurgitation is “fountain”. Ileus in newborns is divided into four main forms: duodenal, intestinal, ileal, and large intestinal obstruction.
Attentive parents can pay attention to the incessant crying of the baby, which eventually turns into screaming
When diagnosing pathology in infants, treatment should be carried out immediately. The long course of the pathology makes the baby’s condition fatal. If you consult a doctor at the first signs of illness, surgery can be avoided. Now let's talk about the processes that can cause ileus in newborns.
Meconium ileus
Pathology occurs due to excessively dense meconium. Original feces have a fibrous and dense structure, which makes it difficult to pass. The causes of this disorder can be several reasons:
- enlarged lymph node;
- infectious processes;
- cystic fibrosis;
- deficiency of digestive enzymes.
Ileus manifests itself in the form of vomiting and bloating. The main task of the treatment process is to remove dense chyme. A gastric tube is inserted into the baby through the mouth and infusion support is provided. For prevention purposes, antibacterial drugs are prescribed. When pathology is diagnosed early, intestinal lavages are performed. In difficult cases and when conservative therapy is ineffective, surgical intervention is indicated.
Hirschsprung's disease
It manifests itself as a violation of motor function, the cause of which is the absence of nerve cells in the intestinal wall. Because of this, the intestinal section is essentially not involved in the digestion process. Hirschsprung's disease primarily affects boys. Hereditary predisposition plays a major role in the occurrence of the disease. Mutations in genes can trigger the development of the disease.
On the first day of life, pathology manifests itself in the form of a lack of stool. During the first years of a baby’s life, constant constipation, lack of appetite, poor weight gain, distended abdomen, vomiting, and developmental delays are troubling. Treatment involves removing the affected area of the large intestine. The operation is recommended to be performed at an early age. Infants are prescribed conservative therapy, which is a preparatory stage for surgical intervention.
Pyloric stenosis
The pathology is characterized by thickening of the muscle, which is located at the transition of the stomach to the duodenum. Pyloric stenosis becomes an obstacle to the entry of food into the small intestine. Immediately after feeding, the baby vomits the contents of the stomach. It turns out that the baby simply regurgitates everything he eats. Because of this, the child does not gain weight. The only solution to this problem is surgery.
Intussusception
There is an insertion of one segment of the intestine along with blood vessels into the adjacent part. Usually during sleep the baby wakes up from severe pain. The attack lasts about ten seconds. Then the child falls asleep safely, but not for a long time, since after about fifteen minutes the pain attack returns.
Children become pale and sweat excessively. Feces take on the appearance of raspberry jelly, as they contain blood and mucus. If the course is favorable, a special enema of the damaged area is performed under general anesthesia. If there is no improvement, surgery is performed.
Symptoms
Acute intestinal obstruction in children manifests itself abruptly and unexpectedly. Each type of disease has a characteristic manifestation, but there is a group of symptoms that accompanies any course of the disease. Symptoms of the disease are:
- pain syndrome is cramping in nature. During an attack, the pain is so intense that children often experience pain shock;
- attacks of nausea with frequent vomiting. Excessive vomiting does not provide relief to the baby's condition. If the large intestine is affected, vomiting may be absent altogether;
- disruption of the process of defecation, or rather, complete retention of stool. Children suffer from constipation, which can only be relieved with an enema;
- increase in abdominal size;
- increase in body temperature;
- increased gas formation;
- decreased appetite;
- the stomach ceases to be soft and elastic, which is why it takes on an irregular shape;
- signs of dehydration.
Intestinal obstruction
If help is not provided to the child in a timely manner, the above symptoms become more intense.
Volvulus of the small intestine
Under normal conditions, the intestinal loops make significant movements and often make turns of up to 90° without causing any pathological disorders. When the intestine is rotated more than 180°, its lumen is blocked and the mesenteric vessels are compressed. Volvulus is promoted by intestinal overflow, increased peristalsis, and adhesions. Volvulus may involve several loops, and sometimes the entire intestine.
Clinical picture and diagnosis . Volvulus of the small intestine begins acutely. The disease occurs with severe general and local clinical symptoms characteristic of acute high strangulation obstruction.
In the first hours of the disease, against the background of constant pain, cramping pain periodically occurs, the intensity of which increases synchronously with peristalsis, reaching the character of unbearable. Often patients become restless, scream in pain, and take a forced position with their legs brought to their stomach. From the very beginning of the disease, repeated vomiting occurs, which does not bring relief, initially with unchanged gastric contents and bile, and then it becomes fecaloid. Retention of stool and gases is an unstable symptom of the disease: often at first there is a single stool due to emptying of the lower intestines, which does not bring relief.
The general condition of the patient is serious. Disorders of water-salt, protein and carbohydrate metabolism, microcirculatory and hemodynamic disorders, intoxication, and decreased diuresis quickly appear and increase. The abdomen is moderately swollen, sometimes the swelling is manifested only by smoothness of the subcostal areas.
A positive sign of Will is often detected - a balloon-shaped loop of jejunum stretched and fixed in the abdomen, over which a high tympanitis and splashing noise are detected.
During a survey fluoroscopy of the abdomen, Kloiber's cups are detected, which appear 1-2 hours after the onset of the disease and are localized in the left half of the epigastric region and in the mesogastric region.
Treatment is surgical. It involves detorsion or “untying” the nodule, removing intestinal contents through a long nasointestinal tube. If the viability of the intestines is beyond doubt, detorsion is limited. In case of intestinal necrosis, the non-viable loop is resected with end-to-end anastomosis. The line of intersection of the intestine should be 40-60 cm above the obstacle and 10-15 cm below it.
Diagnostics
To establish the correct diagnosis, a small patient will need to undergo a whole range of laboratory and instrumental diagnostic techniques. But before prescribing them, the doctor needs to independently perform some activities:
- study the medical history, analyze the life history of the child and immediate relatives - this will help determine some of the causes of the disease, as well as distinguish congenital intestinal obstruction from acquired one;
- conduct a thorough examination of the child, with obligatory palpation of the abdomen, and interview the parents regarding the first time of appearance, as well as the degree of intensity of symptoms.
After this comes the stage of laboratory research, which includes:
- assessment of feces - with such a disorder, it acquires a reddish tint and contains blood impurities;
- general and biochemical study of blood - a way to detect changes in its composition and associated disorders;
- analysis of stool for occult blood - if internal hemorrhages are suspected;
- general urine analysis.
But the basis of diagnosis is instrumental examinations, which involve performing:
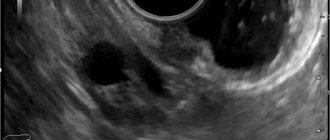
- Ultrasound will make it possible to detect intussusception and other internal causes of the disease;
- X-rays with contrast - procedures to identify specific signs of intestinal obstruction.
Cecal volvulus
Volvulus of the cecum is possible in cases where it has its own mesentery or a common mesentery with the small intestine. With cecal volvulus, the symptoms are as acute as with small intestinal volvulus. Pain (both constant and cramping) is localized in the right half of the abdomen and in the umbilical region. Vomiting is usually observed. Most patients have stool and gas retention.
Upon examination, asymmetry of the abdomen is revealed due to swelling in the umbilical region. At the same time, retraction of the right iliac region occurs. Palpation of the abdomen often reveals a positive Schimans-Dans sign (a feeling of “emptiness” on palpation in the right iliac region) and rigidity of the abdominal wall muscles.
When auscultating the abdomen, characteristic ringing peristaltic noises with a metallic tint are noted. Subsequently, as peritonitis develops, peristaltic sounds weaken.
A plain X-ray of the abdomen reveals a spherically swollen cecum, which is localized in the right half of the abdomen or is displaced inward and upward. In the intestinal projection area, a large (up to 20 cm long) horizontal fluid level is visible.
Treatment
After receiving and studying all the examination results, the specialist prescribes the most effective method of treatment. There are two of them - conservative and surgical.
Before performing drug therapy, the small patient is advised to ensure complete rest, therapeutic fasting, after which dietary nutrition is applied. In addition, conservative therapy includes:
- probing – necessary to free the digestive tract from food accumulation. This can relieve the baby from gagging;
- injections of solutions to restore water-salt balance;
- use of enemas;
- introduction of air into the rectum - which helps to straighten the intussusception;
- taking painkillers, antispasmodics and antiemetics;
- subcutaneous administration of substances to stimulate intestinal function.
In cases of ineffectiveness of previous treatment methods or in severe cases of the disease, medical intervention is prescribed. This method of treatment is carried out by specialists from the field of pediatric surgery. The operation is aimed at removing mechanical blockage, excision of dead intestinal tissue and preventing relapse of the disease.
In addition, complex therapy includes adherence to dietary nutrition. In cases where the disease is eliminated surgically, the patient is prohibited from eating and drinking for twelve hours. After which, gentle nutrition will consist of principles such as:
- complete exclusion from the baby’s diet of foods that contribute to increased gas formation;
- refusal of confectionery products, pickles, fatty meats and fish. It is not recommended to give boiled pasta and raw vegetables;
- all dishes should be boiled or steamed, preferably in a puree state;
- You can drink warm green tea. It is forbidden to give your child cold and carbonated drinks.
There is no specific prevention of acquired or congenital intestinal obstruction in newborns and children in the first year of life. It is only necessary to introduce complementary foods in a timely manner and, if the first symptoms occur, immediately seek help from specialists.