Risk factors
Gallbladder dyskinesia is a polyetiological condition, so doctors need to take into account all possible forms of predisposition to the disease.
It is believed that gallbladder dysfunction may be associated with the patient's lifestyle, heredity and dietary habits. Key risk factors
- Family history of functional diseases of the gallbladder and its ducts. Hereditary factors are often associated with anatomical abnormalities.
- Infectious processes in the liver and bile ducts. Primarily these are hepatitis A and B.
- Surgical treatment of abdominal organs, abdominal trauma.
- Asthenic physique and psychoneurological disorders, accompanied by anxiety and apathy.
- Poor nutrition: excess fatty foods in the diet, snacks before bed, insufficient fluid intake.
- Chronic stress and insomnia.
- Insufficient physical activity.
- Diabetes.
Many risk factors can be eliminated with the help of a therapeutic diet and timely treatment of primary diseases of the gastrointestinal tract.
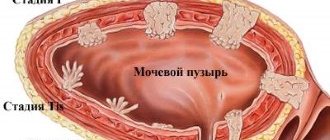
Polyp in the gallbladder - symptoms and treatment
The main tasks of diagnosing a gallbladder polyp are the following:
- Determine whether there are neoplasms in the gallbladder.
- Exclude pathological formations of other origin (cancer and gallstones).
- Distinguish true polyps from pseudopolyps.
- Determine the subtype of the polyp (hyperplastic, adenomatous or cholesterol polyp).
- Determine the number and size of polyps.
- Identify risk factors for malignant polyps:
- polyp size more than 10 mm;
- age over 60 years;
- rapid growth within 1–2 months;
- combination of polyp with gallstones.
The minimum scope of examinations includes:
- clinical blood test;
- general urine analysis;
- blood chemistry;
- Ultrasound of the hepatobiliary zone (HAUS).
A clinical blood test reveals complications, including acute cholecystitis, which is characterized by an increased level of leukocytes. During treatment, a patient with acute cholecystitis donates blood for clinical analysis two or three times. This diagnostic method allows one to evaluate the effectiveness of antibacterial therapy and promptly signal the development of purulent complications.
According to the results of a biochemical blood test, in patients with problems in the gallbladder, the following increases:
- bilirubin level (total and direct) - indicates blockage of the common bile duct;
- creatinine content - helps to assess kidney function and the possibility of using contrast radiography;
- ALT and AST levels indicate liver problems.
Instrumental diagnostics
Transabdominal ultrasound of the abdominal organs - when ultrasound is used to distinguish between different types of tissue, including finding polyps and determining their type. It establishes the number of parietal formations starting from 1 mm in size, determines the thickness of the wall and sometimes shows other disorders: bending of the bladder neck, growth of a polyp into its wall, etc. Since the polyp is closely connected to the wall of the gallbladder, it does not have a shadow on the TAUS image. The polyp is also distinguished by the fact that it does not move when the position of the body changes [9].
Although TAUS can detect 36–90% of gallbladder polyps, this method has its drawbacks [12]. The results of the examination are influenced by many factors such as a “gas echo”, when a section of the intestine filled with gas enters the examination area, a combination of polyps with stones, the modernity of the apparatus and the abilities of the sonographer. TAUS may underestimate the maximum diameter and size of the polyp. Also, ultrasound cannot reliably distinguish non-tumor polyps from tumor polyps [4].
Despite this, TAUS remains the most accessible method for diagnosing gallbladder polyps, which is performed without penetration into the body [2][12].
Computed tomography is rarely used and only with contrast enhancement. It is not very effective for diagnosing polyps smaller than 10 mm, but can reliably detect tumor lesions of the gallbladder [2].
A doctor may suspect cancer due to growth into the liver, focal liver formations, enlarged lymph nodes, the appearance of painless jaundice, unreasonable weight loss of 5–10 kg over the past six months, large polyp size (more than 20 mm) and an unfavorable family history (presence of a similar pathology in close relatives).
Abdominal MRI , like CT, is mainly used to clarify the diagnosis and exclude malignant formation of the gallbladder [2].
Endoscopic ultrasonography allows you to accurately examine tumors and evaluate the functioning of the gallbladder and bile ducts. This method requires careful preparation of the patient [2]. The examination is carried out on an empty stomach. The night before, a light dinner is allowed no later than 18:00. You cannot eat or drink the day before the procedure. For endoscopic ultrasonography, the patient is immersed in a medicated sleep using sedatives.
Pathogenesis
Normally, the evacuation of bile is a coordinated process: sequential contraction of the smooth muscles of the body and neck of the bladder leads to the reflux of fluid into the bile ducts. After cholecystokinin stimulates the relaxation of the sphincter of Oddi, the secretion enters the small intestine and participates in digestion. The nervous system provides activation or inhibition of the functions of the gallbladder, depending on external factors. Specialists are rarely able to determine which link of regulation has changed when a pathology occurs.
Dyskinesia of the gallbladder is primarily manifested by uneven contraction of different parts of the organ. Thus, a combination of rapid contraction of the bladder neck with weakened activity of the muscles of the body of the organ is possible. As a result, bile is not completely excreted, and the walls of the bladder are stretched, after which abdominal pain occurs. Additional symptoms are often caused by other autonomic disorders that affect the pain threshold. A long delay in the excretion of bile is complicated by the formation of stones and complete blockage of the ducts.
Classification
Gastroenterologists classify gallbladder dyskinesia according to the clinical manifestations of the disease, etiology and nature of the motility disorder. All these signs help to choose the optimal treatment for the disease.
Main types of dyskinesia
- Hypertensive motility disorder, manifested by rapid uncoordinated contractions of the gallbladder walls. In most cases, this form of dyskinesia is diagnosed in children and young patients. The main symptom is acute paroxysmal pain that lasts for several minutes.
- Hypotonic motility disorder, in which the gallbladder muscles contract too rarely or not strongly enough. Hypomotor dyskinesia is usually found in older patients. The pain is less acute and lasts longer.
Another classification includes secondary and primary forms of the disorder. Dyskinesia can occur independently due to a violation of innervation, an anatomical defect or hormonal imbalance, but more often a secondary form of the disease is diagnosed, which develops against the background of pathologies of other organs.
Symptoms and signs
The clinical picture of the disease depends on the type of gallbladder motility disorder, the patient’s age and concomitant pathological conditions. The pain syndrome may last for several minutes or persist throughout the day. In general, the nature of pain is an important diagnostic marker.
Other signs:
- nausea and vomiting;
- loss of appetite;
- bloating;
- loose stools or constipation;
- bitterness in the mouth;
- yellowing of the mucous membranes and skin;
- insomnia;
- weakness and fatigue;
- dizziness;
- emotional lability.
Almost all symptoms of gallbladder dyskinesia are nonspecific, so accurate diagnosis is carried out only with the help of special examinations.
Clinical signs of exacerbated cholecystitis
Chronic cholecystitis is manifested mainly by painful sensations in the right hypochondrium, bitterness in the mouth, poor appetite, attacks of nausea, often ending in vomiting. Such symptoms are not permanent, but occur occasionally, for example after eating fatty foods.
With exacerbation, the severity of clinical manifestations increases significantly. Patients complain of severe cutting pain in the area of the right hypochondrium, including spreading to the epigastric region. The pain syndrome radiates to the right shoulder blade, shoulder, and is felt in the right half of the neck. It often spreads to the entire abdominal area and gets worse when you try to take a deep breath or lie down on your left side.
Intense pain is often accompanied by constant nausea. When the vomit, which is bitter due to the presence of bile, is expelled, the person does not feel better. During an attack, the skin turns pale and acquires a jaundiced tint. A thick, dry yellow-brown coating forms on the tongue. Upon palpation, it is noted that the upper right part of the abdominal wall is pathologically mobile. It is in this area that the skin is most sensitive and the most severe pain is felt. A valuable diagnostic sign is the symptom of tension in the muscles of the abdominal wall in response to mechanical pressure.
The localization of pain during exacerbation of cholecystitis is nonspecific. Pathologies that are not related to the digestive system manifest themselves in a similar way. For example, paroxysmal sensations of discomfort behind the sternum, radiating throughout the upper right half of the body, are characteristic of coronary heart disease. Therefore, a differential diagnosis is required, the results of which will allow us to exclude other diseases and establish the cause of the pain.
Diagnostics
To conduct an examination, the patient must contact a gastroenterologist. During the appointment, the doctor will ask the patient about complaints, collect anamnestic data and conduct a physical examination. An external examination allows the specialist to detect jaundice, bloating and pain in the right hypochondrium, but these pathological signs are not always present. The final diagnosis is determined after instrumental and laboratory studies.
Necessary diagnostic procedures
- Laboratory research. First, a blood test is performed to assess the number of white blood cells, determine liver function, and rule out infectious diseases. It is also recommended to test for Helicobacter.
- Ultrasound visualization of the gallbladder. This study does not always detect dyskinesia, but in some cases doctors detect an increase in organ volume and other anomalies. It is also possible to carry out imaging after eating and choleretic drugs: in patients suffering from dyskinesia, the volume of the gallbladder decreases by only 35-40%.
- Radionuclide diagnostics. The introduction of a special chemical marker into the patient’s body gives the specialist the opportunity to assess the functions of the liver and gallbladder.
- Retrograde cholangiopancreatography is a visual examination of the bile ducts and mucous membrane of the gastrointestinal tract.
- Computed tomography or magnetic resonance imaging of the abdominal organs. Obtaining three-dimensional images of these anatomical structures allows the doctor to more accurately determine the cause of the disease.
A gastroenterologist may order a limited number of tests to make a diagnosis after requesting a medical history and reviewing symptoms.
Therapeutic treatment
If impaired motility of the gallbladder is not complicated by severe structural pathologies, doctors prescribe only drug therapy. The main task is to normalize the functioning of the gallbladder and facilitate the evacuation of bile into the duodenum. Before prescribing specific medications, it is necessary to determine the type of disease.
Possible destinations:
- Myotropic antispasmodics that relax the smooth muscles of the gallbladder. These drugs are necessary for the hypertensive form of the disorder.
- Choleretic agents are substances that stimulate the functions of the liver and gallbladder. If the patient has too active muscle contractions, cholespasmolytics are needed to slow down the motility of the organ and eliminate spastic phenomena.
- Cholekinetics and prokinetics for weakened gallbladder motility. These drugs simultaneously improve the contraction of the organ and facilitate the release of bile into the intestines.
- Additional medications: anti-inflammatory drugs and antidepressants to eliminate complications of the disease.
In addition to drug therapy, patients are required to be prescribed a therapeutic diet. The recommended diet depends on the form of the motor disorder, but most often patients are prohibited from consuming too fatty foods and alcoholic beverages.
Diagnosis of dyskinesias of the gallbladder and biliary tract
It is carried out using duodenal intubation. In the hypertensive form of dyskinesia, the administration of a bile secretion stimulator (magnesium sulfate) often causes a painful attack and the gallbladder bile fraction is released quickly or intermittently, the contraction phase of the gallbladder can be shortened. With hypokinetic dyskinesia, bile flows out of the gallbladder after a long period of time after stimulation, and the release of bile occurs slowly. Cholecystography and intravenous cholegraphy, radiocholecystography are also performed. These tests detect changes in the filling and emptying of the gallbladder and help rule out other diseases of the biliary tract and gallbladder.
Surgery
An indication for surgical intervention may be complicated dyskinesia, which cannot be eliminated with drug therapy. Surgery is also prescribed for severe pain and severe digestive disorders. Before surgical treatment, it is important to exclude other pathologies of the gallbladder, such as cholelithiasis or the growth of a malignant tumor. According to modern research, radical treatment is more effective in relieving the symptoms of the disorder.
Depending on the indications and condition of the patient, the doctor may perform an open or laparoscopic cholecystectomy. The operation involves removing the gallbladder. After the intervention, the functions of the digestive system are normalized, but some complications may develop, such as dyslipoproteinemia or dysfunction of the sphincter of Oddi.
What precedes the exacerbation of diseases?
Since exacerbation of chronic cholecystitis is usually caused by violation of a gentle therapeutic diet or alcohol abuse, the doctor analyzes the medical history data. Leading questions about other provoking factors preceding an attack help determine the diagnosis. For example, about possible stressful situations, nervous strain, mental trauma. Unlike cholecystitis, cholelithiasis and pericholecystitis usually worsen after excessive physical exertion, driving on rough roads, or horse riding.
Prognosis and complications
Prognostic data depend on the form of pathology, concomitant diseases and the age of the patient. If gallbladder dyskinesia is not complicated by other disorders, the prognosis is favorable. In most cases, drug therapy can achieve significant improvements.
Possible complications:
- hepatic encephalopathy with prolonged bile retention;
- inflammation of the gallbladder and its ducts;
- the occurrence of secondary infection;
- insufficient supply of nutrients to the body.
To prevent the development of complications, it is necessary to follow a therapeutic diet.
Prevention
Many diseases of the digestive system are long-term consequences of an unhealthy lifestyle, so preventive measures help prevent dysfunction of the gallbladder and its ducts. First of all, doctors recommend paying attention to primary pathologies and nutritional habits.
Basic recommendations
- Improving your diet: avoiding too fatty foods, fried foods, alcohol and excess spices. Adequate fluid intake.
- Normalization of body weight and regular physical activity.
- Avoiding stress, treating anxiety.
- Timely detection and treatment of inflammatory processes in the gallbladder and intestines.
- Regular examinations by a gastroenterologist in the presence of chronic diseases of the digestive system.
- Refusal of hormonal contraceptives and somatostatin drugs.
Thus, gallbladder dyskinesia is a common disease manifested by impaired motility of the organ. Insufficient bile secretion can lead to serious complications, so this disorder must be treated when the first symptoms appear. Most often, taking medications and lifestyle changes is enough.
Diseases of the bile and hepatic ducts and their manifestations
Causes of diseases of the bile ducts:
- parasites;
- tumors of the mucous membrane and submucosal layer;
- heterogeneous consistency of bile;
- damage to the duct by calcifications.
The main risk group is women, because they are more likely than men to experience hormonal problems and suffer from excess weight.
Blocked ducts
Most often, the ducts become blocked due to cholelithiasis. Obstruction can also be caused by a tumor, inflammation of the walls of the ducts, a cyst, helminthic infestation, or a bacterial infection. Narrowing of the ducts (strictures)
The main reason for this pathology is a previous operation to remove the gallbladder or tumor, cyst in the duct. Inflammation persists for a long time after surgery, which leads to narrowing. The patient loses appetite, experiences pain in the right side, and his body temperature rises.
Screeds and scars
The walls of the duct are replaced by scar tissue due to inflammation caused by sclerosing cholangitis. As a result, the outflow of bile is disrupted, it is absorbed into the blood and stagnates in the gallbladder. There are no symptoms, but as the disease progresses, liver cells die.
Swelling
The walls of the bile ducts become denser due to catarrhal inflammation. In this case, overcrowding of the blood vessels occurs, the mucous membrane of the duct swells, leukocytes accumulate on the walls, and the epithelium exfoliates. Often this disease becomes chronic. At the same time, he constantly experiences discomfort in the right side, he is tormented by nausea, and vomiting occurs.
Cholelithiasis
Stones in the biliary system are formed due to stagnation of bile in the gallbladder and disruption of cholesterol metabolism. For treatment, medications are prescribed, under the influence of which the stones leave the gallbladder through the ducts. The patient feels a stabbing, cutting pain in the right side. A large stone may partially or completely block the duct. This is called gallbladder spasm. Its symptoms are pain, nausea, vomiting.
Tumors and metastases in cancer
Klatskin tumor is often found in older patients with biliary problems. In 50% of cases, a malignant tumor forms in the common bile duct. If left untreated, metastases appear, affecting regional lymph nodes, pancreas, and liver. The disease can be detected at an early stage if the symptoms are not ignored: pain in the right hypochondrium, which radiates to the neck and shoulder blade.
Parasites
Trematodes, Giardia, and flukes may appear in the gallbladder and ducts. They cause chronic inflammation of the walls of the gallbladder and disrupt the contractile function of the ducts.
Free or paid treatment?
Dyskinesia
With this disease, the consistency of contraction of the walls of the gallbladder and its ducts is disrupted. As a result, bile enters the duodenum in deficiency or excess, which disrupts the process of digestion and absorption of nutrients.
Cholangitis
Inflammation of the bile ducts occurs when they become blocked or liver secretions become infected with bacteria. There are three types of inflammation:
- acute, occurring unexpectedly - a person has a headache, the skin turns yellow, a stabbing pain appears in the right hypochondrium, which radiates to the shoulder and neck;
- chronic – mild pain on the right side, increased body temperature, bloating of the upper abdomen;
- sclerosing - there are no symptoms, and if left untreated, liver failure develops, which cannot be cured.
Extension
Most often it occurs due to increased contractility of the walls of the gallbladder. There are other reasons - blockage of the common duct with a tumor or stone, improper functioning of the sphincters. As a result, the pressure in the biliary system increases and the ducts expand.
Biliary atresia
This is a blockage or absence of the bile ducts. The disease is found in newborns. The child's skin becomes yellow-green, the urine darkens, and the feces become white-gray. If the pathology is not treated, the child will not live more than one and a half years.