Read about the diagnosis and treatment of cholelithiasis at the link.
Get help right away if you develop signs and symptoms of a serious complication related to gallstones, such as:
- Abdominal pain is so severe that you cannot sit still or find a comfortable position
- Yellowing of the skin and whites of the eyes (jaundice)
- High temperature with chills
Number to call an ambulance in Moscow – 103
Causes of cholelithiasis
It is not clear what causes gallstones to form. Doctors believe that gallstones can occur in the following cases:
Your bile contains too much cholesterol . Normally, your bile contains enough chemicals to dissolve the cholesterol released by your liver. But if your liver produces more cholesterol than bile can dissolve, the excess cholesterol can turn into crystals and eventually stones.
Your bile contains too much bilirubin . Bilirubin is a chemical that is produced when red blood cells are broken down in the body. Under certain conditions, the liver produces too much bilirubin, including cirrhosis of the liver, bile duct infections, and some blood disorders. Excess bilirubin promotes the formation of gallstones.
Your gallbladder is not emptying properly. If the gallbladder does not empty completely or often enough, the bile can become very concentrated, which contributes to the formation of gallstones.
Types of gallstones
Types of gallstones that can form in the gallbladder include:
Cholesterol stones in the gall bladder. The most common type of gallstones, called cholesterol gallstones, are often yellow in color. These gallstones are composed primarily of undissolved cholesterol, but may contain other components.
Pigment stones in the gall bladder. These dark brown or black stones form when your bile contains too much bilirubin.
Risk factors
Factors that may increase the risk of gallstones include:
- Female
- Age 40 and older
- Overweight or obesity
- Passive lifestyle
- Pregnancy
- High Fat Diet
- High Cholesterol Diet
- Low fiber diet
- Family history of gallstones
- Diabetes
- Having certain blood disorders, such as sickle cell disease or leukemia
- Very fast weight loss
- Taking medications that contain estrogen, such as oral contraceptives or hormone therapy.
- Liver disease
Biliary dyskinesia
Treatment should be comprehensive, including normalization of the diet and nature of nutrition, sanitation of foci of infection, desensitizing, antiparasitic and anthelminthic therapy, elimination of intestinal dysbiosis and hypovitaminosis, and elimination of symptoms of dysfunction. Diet therapy plays an important role: avoiding the intake of extractive products, refractory fats, confectionery products, cold dishes, and foods that cause gas formation in the intestines.
Much attention is paid to correcting the state of the autonomic nervous system. For the hypertensive-hyperkinetic type of dysfunction, sedatives (bromides, valerian, motherwort) are prescribed; for hypotonic-hypokinetic - tonics (extracts of Leuzea, Eleutherococcus, tinctures of ginseng, lemongrass, aralia). In case of giardiasis or helminthic infestation, antiparasitic and anthelmintic therapy is carried out.
Restoring the function of bile formation and bile drainage in different types of dyskinesia is also carried out differently. For hyperkinesia, choleretics (dry bile, cattle pancreas extract, flamin, hydroxymethylnicotinamide, oxafenamide), low-mineralized mineral waters in heated form, antispasmodics (drotaverine, papaverine, platiphylline), herbal infusions (decoctions of chamomile, peppermint, licorice root, dill fruits) are indicated. .
Among non-drug methods, patients with hypertensive-hyperkinetic biliary dyskinesia are recommended courses of psychotherapy, acupuncture, hirudotherapy, ozokerite and paraffin applications, diathermy, inductothermy, microwave therapy, electrophoresis with antispasmodics, acupressure, massage of the collar area.
For the hypotonic variant, cholekinetics (xylitol, magnesium sulfate, sorbitol), highly mineralized water at room temperature, herbal medicine (decoctions of immortelle flowers, nettle leaves, rose hips, oregano, St. John's wort) are prescribed. If there are signs of intrahepatic cholestasis, blind probing (tubage) is indicated. To increase overall tone, exercise therapy, stimulating water procedures, and tonic massage are prescribed.
Physiotherapy methods include diadynamic therapy, electrophoresis with magnesium sulfate on the liver area, low-intensity ultrasound, SMT therapy, and low-frequency pulsed currents. Patients with gastrointestinal dyskinesia are advised to undergo observation by a gastroenterologist and neurologist, and annual health courses in balneological sanatoriums.
Complications
Complications of gallstones may include:
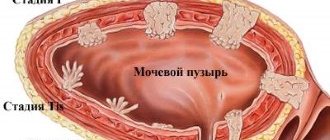
Inflammation of the gallbladder . A gallstone stuck in the neck of the gallbladder can cause inflammation of the gallbladder (cholecystitis). Cholecystitis can cause severe pain and peritonitis.
Blockage of the common bile duct . Gallstones can block the channels (ducts) that carry bile from the gallbladder or liver to the small intestine. This can lead to severe pain, jaundice, and bile duct infection.
Blockage of the pancreatic duct . The pancreatic duct is a tube that comes from the pancreas and joins the common bile duct just before it enters the duodenum. Pancreatic juices, which aid digestion, pass through the pancreatic duct.
A gallstone can cause a blockage of the pancreatic duct, which can lead to inflammation of the pancreas (pancreatitis). Pancreatitis causes severe, persistent abdominal pain and usually requires hospitalization. Severe forms of pancreatitis often result in the death of the patient.
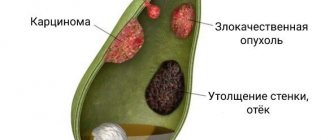
Gallbladder cancer . People with gallstones have an increased risk of developing gallbladder cancer.
One of the main functions of the liver is bile production. The liver has two unequal lobes - right and left. The anatomical and functional (ultrasound) division of the liver into the right and left lobes differs. According to Couinaud’s classification (C. Couinaud, 1957) [1], segments I and IV are anatomically located in the right lobe, and functionally belong to the left lobe [2, 3]. Bile is collected from all segments and both lobes into lobar ducts.
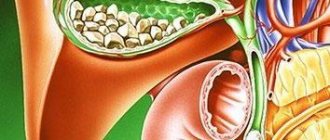
In a healthy person, the intrahepatic ducts ductus hepaticus dexter (right hepatic duct) and ductus hepaticus sinister (left hepatic duct) (Fig. 1) are not visible on ultrasound; only the ductus hepaticus communis (common hepatic duct) is visible with good visualization. It connects with the ductus cysticus (cystic duct) and forms the ductus choledochus (common bile duct), which normally has a length of 5-7 cm [4].
Rice. 1. Gall bladder and bile ducts.
The common bile duct opens into the descending part of the duodenum and has sections designated according to its position relative to the duodenum and pancreas after it leaves the liver: CH1 - supraduodenal section, CH2 - retroduodenal section, CH3 - pancreatic section (located deep in the head of the pancreas). The portal of the liver is located deep in the parenchyma - this zone is projected during ultrasound examination inside the liver; this part of the common bile duct does not have a classification name (CH0, portal section) [5].
The pancreatic duct (ductus pancreaticus, Wirsung's duct) and the common bile duct at the level of the lower third of the descending duodenum are connected on the medial side. After fusion, a 2-3 mm long section is located inside the papilla duodeni major (major papilla of the descending duodenum, papilla of Vater), this is CH4 - the intramural section of the common bile duct.
Gallbladder: ultrasound approaches. The term "approach" in ultrasound refers to the position of the ultrasound transducer on the patient's body for optimal visualization of the organ.
1. Subcostal access (Fig. 2, a) . The position of the sensor is oblique below the costal arch, parallel to it. The gallbladder is most often projected along the midclavicular line. With the correct placement of the sensor, the gallbladder in this section is recessed into the liver parenchyma. By tilting the sensor in a direction closer to the spine or closer to the costal arch, you can see the lobar branches of the portal vein (right and left) and the inferior vena cava (see Fig. 2, a); these are additional landmarks for finding the gallbladder [6].
Rice . 2. Gallbladder: subcostal access (a; according to [5]); intercostal access (b) and biometry (c; according to [5]).
2. Intercostal access. The sensor is located parallel to the ribs in the intercostal space, approximately outward from the midclavicular line. With this position of the sensor (Fig. 2, b), the right lobe of the liver is mainly visible, the gallbladder is visible from below the liver, adjacent to it, adjacent to the corner of the edge of the liver. Additional landmarks are the trunk of the portal vein, which deep in the liver is divided into right and left lobar branches, and laterally to the right, the inferior vena cava.
Biometric parameters of the gallbladder and biliary tract. The size of the gallbladder is very variable (in patients of different constitutional types, depending on the filling, characteristics of smooth muscle, how it reacts to contraction).
Normal: length <120 mm in adults, can be measured both in subcostal (somewhat shorter, since it is more difficult to bring out the entire length) and in intercostal approaches. The transverse diameter is normally <40 mm and is measured strictly at right angles to the length. Fasting wall thickness <2 mm, contracted bladder wall thickness <4 mm (if the patient ate food on the day of examination) [7, 8].
The gallbladder wall should be measured at the site closest to the transducer, as the dorsal reinforcement effect may result in the appearance of greater thickness. If this is an intercostal approach (Fig. 2, c) , then the dorsal (anterior) wall of the gallbladder should be measured - adjacent to the visceral surface of the liver, and not the ventral (posterior).
Bile ducts. In Fig. 3, the right and left hepatic ducts and the ducts flowing into them are clearly visible, since they are dilated as a result of obstruction of the bile ducts distally beyond the liver (normally not detected) [9, 10].
Rice . 3. Intrahepatic bile ducts (identified against the background of obstruction of the common bile duct).
The walls of large and small ducts in Fig . 5 are uneven, this is detected only in the case of obstruction. The common bile duct is located outside the liver, in Fig. 4 it is curved, adjacent to the visceral surface of the liver, its right section is embedded in the head of the pancreas [7].
Rice. 4. Common bile duct.
In Fig. 4, additional landmarks are also visible: a large venous vessel - the inferior vena cava, posterior to which are located the right renal artery, the right branch of the hepatic artery and the portal vein. The normal diameter of the common bile duct is <6 mm. After cholecystectomy <9 mm (according to B. Blok) is compensation for the possibility of bile accumulation in the gallbladder.
In Fig. 5 areas in the yellow circle on the echograms correspond to the area in the yellow circle in the diagram [11]. The most superficial structure is the common hepatic duct; the right hepatic artery crosses it deeper at a right angle, and the portal vein is located even deeper. Normally, the portal vein (about 6 mm) is thicker than the common hepatic duct (about 4 mm). In the diagram and on the echogram in the red circle, the area in which the cystic duct connects with the common hepatic duct is the place of formation of the common bile duct.
Rice. 5. Common hepatic and common bile ducts (according to [11]).
On the echogram in Fig. 5 the gallbladder and the so-called Mickey Mouse are visible, whose ears are sections of the cystic and common bile ducts, the head is a section of the common bile duct, and the body is a section of the portal vein.
Parasagittal approach (see Fig. 5) : the common bile duct and the gastroduodenal artery are directed at an acute angle to each other (the common bile duct is green, the gastroduodenal artery is red).
In Fig. 6 on echogram 1 the head of “Mickey Mouse” is visible: at the gate of the liver there are ears (the right one is the common bile duct or in some cases the common hepatic duct, the left one is the proper hepatic artery), the head is the portal vein, the torso is the inferior vena cava. The supraduodenal part of the common bile duct is shown in yellow on the echogram and diagram [12].
Rice . 6. Sections of the common bile duct (according to [12]).
On echogram 2 (see Fig. 6) , the portal vein is identified, parallel to it is the common bile duct (the supraduodenal and retroduodenal parts are visible), the upper part of the duodenum, the pylorus, and the pancreas.
Echogram 3 (see Fig. 6) shows a transverse scan - the pancreas is well recognizable due to the splenic vein, two anechoic points are visible at the level of the head of the pancreas: the lower one is the pancreatic section of the common bile duct, the upper one is the gastroduodenal artery. The inferior vena cava, aorta and superior mesenteric artery are also identified. The pancreatic part of the common bile duct is shown in red on the echogram and diagram.
The intramural part of the common bile duct is located in the wall of the descending duodenum and is normally not visible (Fig. 7) .
Rice . 7. Examples of echograms of the common bile duct.
Sphincter apparatus of the biliary tract. In Fig. Figure 8 shows small folds of the mucous membrane of the gallbladder, spiral folds inside the cystic duct (Heister valves).
If you dissect the mucous membrane of the duodenum, you can see sphincters - smooth muscle fibers covering the ducts: the sphincter of the common bile duct (Aschof), the sphincter of the pancreatic duct and, after their fusion, the sphincter of the hepatic-pancreatic ampulla, or the sphincter of Oddi (see Fig. 8; Fig. . 9) . In Fig. 8 also indicates Lütkens' sphincter - between the neck of the gallbladder and the cystic duct.
Rice . 8. Sphincter apparatus of the biliary tract.
Rice . 9. Anatomy of the major duodenal papilla (papilla of Vater) [4].
Normally, these structures are not visible during ultrasound examination [6].
The authors declare no conflict of interest.