Abdominal ultrasound (from abdominous - belly, belly) is a method of ultrasound diagnostics of the abdominal and pelvic organs, carried out through the abdominal wall using a special sensor with a transducer inside. The device recognizes the impulse reflected from the organ and converts it into an electrical signal.
Ultrasound of the pelvis - 1000 rubles. Consultation on diagnostic results (optional) - 500 rubles.
SIGN UP FOR AN ULTRASOUND
The sensor is not inserted internally (into the rectum or vagina). Due to its high efficiency and lack of discomfort for the patient, abdominal examination is used as a method of primary diagnosis of diseases and pathologies of the liver, gallbladder, pancreas, spleen, less often the stomach and duodenum, as well as all organs of the genitourinary system in men and women.
How does an abdominal examination differ from a regular ultrasound?
The content of the article
The difference between the examination procedure with an abdominal sensor and a conventional ultrasound device lies in the design of the sensors.
In a conventional ultrasound, it is piezoelectric, that is, it works on the principle of distortion of crystals under the influence of electrical voltage. The sensor emits and receives ultrasonic pulses, and the device converts them into a picture on the screen. For abdominal examination, convex sensors are used. They differ from conventional linear sensors in their curved shape. The radius of curvature varies depending on the area of the body being examined.
Why is the examination carried out with different sensors?
Modern devices have sets of sensors with different power, curvature and other parameters. The correct choice of sensor is very important and affects the effectiveness of ultrasound.
- Dimensions
. Sensors for abdominal examination are: 40 mm; 50 mm; 60 mm; 70 mm. - Scan angle
. Also, the sensors have different scanning angles: 500; 600; 700; 800. - Frequency
. The frequency ranges of the sensors differ as follows:
- 2-6 MHz (used when studying very obese people with a thick layer of fat on the abdomen (fat tissue interferes with the examination) or for studying deeply located organs up to 25 cm);
- 3-8 MHz (used for examining pregnant women and children 1-8 years old);
- 5-10 MHz (used in neonatal studies (infants up to 28 days of age) or for studying superficial organs).
There are microconvex abdominal sensors that are used for more detailed examination of organs in young children and in gynecology and urology.
Sensors with a surface curvature of 10-14 mm are suitable for vaginal examinations, and with a curvature diameter of 8-10 mm - rectal ones. Such details are important for a clear image of small areas of the organ (when considering fibroids, prostate adenoma, fetus at short term). In pediatrics, when studying small organs, sensors with a curvature of 20-40 mm are used (for example, to study the brain through the fontanel).
Microconvex sensors have a handle for ease of insertion, and can rotate around its axis to view the organ in different projections. Convex sensors may change during the examination. They are selected depending on the tasks assigned to the doctor, the characteristics of the patient (overweight, age) and other factors.
What does an abdominal ultrasound show?
Abdominal ultrasound examination is used in the diagnosis and treatment of various diseases, to monitor the progress of pregnancy, etc. In particular, abdominal ultrasound helps identify the following problems.
Abdominal organs
With an abdominal ultrasound of the abdominal cavity, the following are clearly visible: gallbladder, liver, spleen, pancreas, kidneys.
Ultrasound reveals:
- liver cyst;
- hepatitis (liver inflammation caused by a viral infection);
- kidney abscess;
- malignant and benign tumors;
- stones in the gall bladder, pancreas and bile ducts;
- cholecystitis (inflammation of the gallbladder due to the presence of a large number of stones in it);
- cholestasis - accumulation of bile;
- empyema (accumulation of pus inside an organ due to impaired bile outflow);
- pancreatic necrosis;
- abdominal aortic aneurysm (pathological expansion of the aortic lumen as a result of injury);
- hemorrhages in the spleen, enlargement or reduction of the spleen.
urinary system
The doctor sees: kidneys, adrenal glands, bladder.
Detects diseases:
- hydronephrosis (enlargement of the renal pelvis);
- pyelonephritis (inflammation of the kidney tubules);
- kidney cyst, kidney tumor;
- diverticula (inflammation of the intestines);
- urolithiasis disease;
- kidney abscess (proliferation of a purulent cavity).
Pathologies will also be identified: aplasia (one kidney instead of two), kidney duplication (three instead of two), nephroptosis (prolapse of the kidney), dystopia (improper position of the kidneys in the pelvis), changes in parenchymal tissue (dystrophy or swelling of the kidney), glomerulonephritis (immune damage to the glomeruli of the kidney).
Anechoic (lack of ultrasound reflection) indicates cavitary formations (cysts and abscesses), hyperechoic (increased ultrasound reflection) indicates sclerotic changes in the kidneys, as well as the presence of stones and sand inside the organ.
Pelvic organs (women)
Visible on ultrasound:
uterus, cervix, fallopian tubes, bladder.
Detects diseases:
- inflammation of the appendages;
- uterine fibroids (benign tumor in the muscle layer of the uterus);
- endometriosis (growth of the inner layer of the uterine wall);
- ovarian cyst;
- early pregnancy (from the second week of delay).
Pelvic organs (men)
Visualized: prostate, bladder.
Diseases are defined:
- prostate adenoma (benign growth of glandular tissue of the prostate);
- prostate tumor;
- prostatitis (inflammation of the prostate gland).
Treatment methods for abdominal oncology
The goal of surgical treatment of oncological diseases is to perform the most radical amount of surgical intervention while maintaining the most comfortable quality of life for the patient after surgery.
Laparoscopic operations involve significantly less trauma than conventional open surgery and allow the patient to recover faster. Along with laparoscopic operations performed through 3 punctures, operations through a single puncture in the navel area are practiced - the so-called SILS technique.
Like any type of surgery, abdominal surgery has a number of side effects. Surgeries are performed on vital organs that perform an important function in the body. After the operation, unpleasant consequences may occur:
- blood residues on the operated area can provoke the formation of acute purulent peritonitis;
- during intervention, adhesions of different sizes may form on the intestines;
- internal bleeding in the abdominal cavity;
- prolapse of an organ outside the abdominal cavity – eventration.
It is impossible to predict possible complications in advance. Symptoms appear after surgery after a certain time.
After the operation, the recovery period begins, requiring special care; you must follow a list of doctor’s recommendations. The duration of rehabilitation takes from 7 days to several months, depending on the type of surgery performed and the severity of the disease.
Antitumor drug therapy is also prescribed, which includes:
- application of modern methods of chemotherapy, immunotherapy and endocrine therapy;
- advanced cytotoxic and targeted antitumor drugs;
- use of current chemotherapy protocols in accordance with the recommendations of the European Society of Oncologists and the Russian Society of Chemotherapists-Oncologists;
- conducting molecular genetic testing when choosing drugs for antitumor therapy.
The choice of treatment tactics depends on the location, size, stage of the malignant tumor, and the number of nodes. The doctor must also take into account the general condition of the patient, his age, and the presence of concomitant diseases.
Abdominal examination modes
There are 4 modes of abdominal examination.
- A-mode (amplitude)
is the simplest mode, it allows you to determine the distance to the organ and its parameters; - B-mode or 2D
makes it possible to see an image of an organ in 2D format; - M-mode
creates a video recording of an image with clear boundaries; - Doppler mode
. It shows blood flow in color or black and white modes; - The harmonic mode
allows deep penetration of ultrasonic beams, creating a high-resolution image.
Malignant tumor of the abdominal cavity
Many malignant tumors spread metastases to the peritoneum, a thin “shell” that covers the internal organs and walls of the abdominal cavity. This phenomenon is called (from the Latin peritoneum - peritoneum) peritoneal carcinomatosis (carcinomatosis is not recognized by everyone, but is a generally accepted synonym that we also use). Millet-like (small, like millet) metastases are scattered over the entire surface of the peritoneum.
This happens in 50% of cases in abdominal oncology (tumors of the gastrointestinal tract or reproductive organs). Let us remind you that colorectal cancer (colon and rectum) and stomach cancer are in 2nd and 3rd place in the number of deaths among all cancers.
The prognosis for primary peritoneal cancer directly depends on whether all tumor foci were removed during surgery. Unfortunately, the disease is often diagnosed at a late stage, so relapses often occur after treatment. Patients usually require more than one surgical intervention or course of chemotherapy.
Peritoneal carcinomatosis with metastases of other types of cancer sharply worsens the prognosis. Typically, the life expectancy of such patients is measured in months. But HIPEC can significantly extend it, up to several years - if such treatment is possible for a particular patient. The technique gives excellent results: it increases the 5-year survival rate to 40-50%, and sometimes provides a complete cure.
How is an abdominal ultrasound examination of various organs performed: preparation, advantages, disadvantages
Let's consider each organ separately, since both a comprehensive examination of the body and individual diagnostics of organs can be carried out abdominally.
Prostate
Ultrasound of the pelvic organs in men begins with the preparatory stage. An hour or two before the procedure, the man should drink several glasses of water to ensure that the bladder is well filled. Naturally, you cannot go to the toilet, otherwise the ultrasound readings will be distorted.
The man lies down on the couch. Inspection is carried out with sensors in any projection and plane. Transverse scanning determines the thickness (1.6-2.5 cm) and width (2.7-4.2 cm) of the prostate gland. Longitudinal scanning shows the length of the prostate, which should not exceed 4.1 cm.
Based on the thickness, length and width readings, the doctor calculates the volume of the organ, which should not exceed 28 cm3. After the ultrasound, the patient empties the bladder. The doctor takes measurements of residual urine, which is an important indicator when diagnosing prostate adenoma.
The disadvantage of the abdominal method of examining the prostate gland is the inability to determine the structure of the prostate. The sensor is not sensitive enough to “see” small lumps and tumors. Ultrasound sees the shape, size and outline of an organ. If they differ from normal standards, the patient is sent for further examination.
Bladder
Examination of the bladder using the transabdominal method is the only possible examination in children. The transvaginal method is excluded for girls, and the transrectal method causes such discomfort and panic in children that it is rare that a child will agree to such an examination. An abdominal ultrasound of the bladder is done according to the same principle as an examination of the prostate gland.
Shortly before visiting the office, the patient drinks liquid to keep the bladder full. If it turns out to be empty, it will not be able to transmit ultrasound, and nothing will be visible on the monitor. Ultrasound does not see organs filled with air. It is also undesirable to indulge in starchy and floury foods, fruits and vegetables, so as not to cause excessive gas formation in the intestines. If there is a predisposition to flatulence or bloating, the patient takes Espumisan or other gas-neutralizing drugs the day before.
The patient lies down on the couch, and the doctor applies a special gel to the abdomen that eliminates air pockets between the sensor and the surface of the abdominal cavity. Then the doctor examines the bladder in different planes and projections. If the parameters (diameter, wall thickness) do not correspond to the norm, the patient is sent for a more detailed examination.
Liver
Abdominal examination of the liver gives excellent results, revealing the true picture of structural changes. Ultrasound of the liver allows you to see obstruction of the bile ducts, cirrhosis at all stages, abnormal fibrous formations, changes in renal blood flow, fatty liver disease and much more. When diagnosing an organ, no other type of examination will provide such a complete picture.
The patient is also placed on a couch and a special gel is applied to his stomach. The doctor then moves the transducer, and the result of the ultrasound radiation interpreted by the transducer is displayed on the screen. The liver lies close to the surface, and this greatly facilitates ultrasound examination.
Spleen
Sometimes liver diseases are combined with spleen pathologies. The organ increases in size and its structure changes. An abdominal examination shows inflammation or damage due to trauma (accident, heavy physical activity). An enlarged spleen indicates a blood disorder. Ultrasound will help diagnose infection and various tumors.
Kidneys
The kidneys are a rather traumatic organ. Performing the most important function in the body, the kidneys are susceptible to stone formation. Stones block urination by blocking the tubules. The morphology of the kidneys changes, and renal failure develops. An abdominal examination will look for organ obstructions, stones, and duct problems.
The patient lies on his stomach, and the doctor looks at the kidneys from the back. They are located close to the surface, so they are clearly visible both in size and structure.
Pancreas
Pancreatitis, or inflammation of the pancreas, is a deadly disease. An abdominal ultrasound will show the abnormal amount of fluid surrounding the gland and will also help differentiate a normal fluid-filled cyst from a malignant tumor.
Sometimes the cause of problems in the functioning of the organ is stones, and they can only be seen using an abdominal ultrasound. The cause of sharp pain in the right hypochondrium is a narrowing of the bile ducts. In case of acute pain, the patient is immediately sent for an abdominal ultrasound.
Gallbladder
Intolerance to fatty foods, large meals or movement of stones causes unbearable pain in the gallbladder area. In these cases, the patient is sent for an abdominal ultrasound. The study will help identify inflammation of the organ, stones in the bile ducts. The patient will be quickly prescribed the necessary treatment and relieved of severe pain.
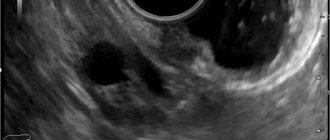
Gynecology
An abdominal pelvic ultrasound will help to see uterine fibroids, endometriosis, ovarian cysts, and inflammatory processes in the appendages. However, ultrasound will not detect cervical pathology; for this it is necessary to use a transvaginal sensor.
Abdominal aorta
In emergency cases (road accident, fall from a height), the abdominal aorta is damaged and blood stops flowing from the heart to the abdominal and pelvic organs. An abdominal ultrasound examination will help identify a life-threatening aneurysm.
What else is revealed with the help of an abdominal examination?
The doctor will definitely give a referral for an ultrasound in the following cases:
- diagnosis of appendicitis;
- drainage of fluid from the cyst;
- performing a biopsy;
- pregnancy at different stages;
- diagnosis of abscesses and hematomas in blunt abdominal trauma;
- location of the renal pelvis.
Abdominal pain and intestinal pathology. Diagnostic issues, treatment approaches
Vladimir Trofimovich Ivashkin , academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences:
– Message from Marina Fedorovna Osipenko, professor from Novosibirsk.
Marina Fedorovna Osipenko , professor:
– Good afternoon, dear colleagues, dear Vladimir Trofimovich! The problem that I would like to discuss and touch on today concerns abdominal pain and intestinal pathology, issues related to diagnosis and treatment approaches. It seems to me that the fact that we began to discuss not only the nosological approach to patient management, but also the syndromic one, is actually very important, because especially for primary care doctors - and not only for primary care doctors, and for specialized specialists – patients do not come with a ready-made diagnosis, patients come with symptoms, syndromes, and, of course, our task is to verify the cause of these symptoms and syndromes, to build a nosological diagnosis. But on the other hand, our task is to ensure a certain quality of life for our patients even at the time of examination, and on the other hand, of course, to provide assistance in relieving symptoms and syndromes.
So, dear colleagues, you and I know very well that chronic pain - and in the vast majority of cases and most often we still encounter just such pain - affects 19-20% of the adult population. That is, almost every fifth person suffers from various manifestations or various causes, so to speak, underlying the occurrence of pain, and, of course, abdominal pain is one of the very serious symptoms for which our patients suffer greatly. Of course, we must remember very seemingly simple points, but they are very important so that you and I, in addition to identifying the abdominal pain itself, can also identify the causes of its occurrence. We all know very well from our student days that the mucous membrane does not have pain receptors, and accordingly, even severe lesions of the mucous membrane are often not accompanied by any pain. On the other hand, we understand that changes in pressure in the lumen of a hollow organ, which undoubtedly includes the entire intestine, lead to the activation of nociceptive receptors and the appearance of various pain sensations, just like the parietal peritoneum and mesentery , and in the end this is very, I emphasize once again, important, and you and I understand this, in order to verify the cause of pain.
Actually, it has long been clear that the level and threshold of pain perception is very different for everyone, and now a large amount of research in the world is devoted specifically to the genetics of pain, and more and more research concerns the enzymes involved in the metabolism of catecholamines and enkephalins, and features in the structure of the metabolism of opioid receptors, and genes that transfer afferent neurons, just like the genes that determine the transport of potassium, calcium, sodium ions, and so on. It is absolutely clear that in many respects the subjective perception of pain (and you and I perfectly understand that pain is a subjective manifestation of one or another degree of ill-health on the part of different systems and organs), it is determined precisely by a number of complex genetic factors, because one and the same In fact, a stimulus, if assessed even from some strict physical parameters, evokes completely different sensations in the patient. And we must, despite seemingly very banal things, clearly understand that in order to move from the syndrome to the actual nosological form, we must verify abdominal pain well enough and understand the possible mechanism of its occurrence.
We must find out the duration of the pain, we must find out its nature, we must find out its localization, we must try to determine whether its genesis is functional or organic, we must try to determine the mechanism of its formation, while taking into account and taking into account that in origin, despite localized in the abdominal area, this may not only be a pathology of the gastrointestinal tract itself, but it may also be manifestations from other systems and organs. Therefore, purely propaedeutic things were, are and remain very important in order for us to get out or move on, strictly speaking, to a diagnostic search. This is a necessary option for a normal diagnostic search. Of course, in most cases, we, gastroenterologists, and therapists in general, most often encounter subacute or chronic pain, that is, pain that lasts more than two days, let’s say. Acute pain in most cases is still the destiny of surgery, although any pain that later becomes chronic, it certainly begins at some point.
Of course, such moments as colic, which is still more associated with an increase in intraluminal pressure, or pain of an inflammatory nature, is more well localized, of a constant nature, more acute in the subjectivity of sensations, or ischemic in nature, with increasing intensity, aching , constant, around the clock - all this also helps us to verify the diagnosis in the same way as the localization of pain. If we are now focusing, or I am emphasizing in my message, on intestinal diseases that are manifested by abdominal pain, then we also know very well the places of localization of pain associated with the intestines - these are the lower abdomen or the right upper quadrant of the abdomen. The same important point is the attempt to determine the leading mechanism of the formation of abdominal pain, because we know very well that parietal pain is always the involvement of the peritoneal cover. It is clearly localized, it is accompanied by varying degrees of muscle tension, and the example that Vladimir Trofimovich gave at the very beginning of our round table once again emphasizes that the presence of parietal pain in the patient was not accompanied by the classic manifestations of this disease, but for all that in Ultimately, this situation turned out to be so. It intensifies with a change in body position, coughing, and, of course, if there is a suspicion that the pain is of a parietal nature, without a doubt, consultation with a surgeon and the surgeon’s participation in the management of patients must be mandatory.
Visceral pain - this is what we mostly encounter - this is precisely a change in pressure, stretching, tension, perhaps a circulatory disorder, this is the involvement of nosoceptive factors, and so on. In most cases, we are faced with precisely this genesis of pain. Referred, referred pain also gives us a lot of problems, since we often deal with it, and, of course, not arising in the place where the organ is projected, it gives us a lot of problems. Well, and, finally, psychogenic, which, essentially, we can diagnose only by the method of exclusion and with the help of completely different, very weak, let’s say, inherently tests. Of course, parietal pain is always an organic disease, without a doubt. As for organic diseases, in the initial stages, or rather, not even in the initial stages, but in the absence of complications, they can be accompanied by visceral pain. As soon as a reaction from the peritoneum occurs, it is, without a doubt, parietal pain.
Functional diseases are always visceral pain plus psychogenic pain, plus there may be components of radiating pain. The scope of examinations is different for all patients, and this, in fact, is a big task, because if all patients with abdominal pain are examined in depth using everything that is available in the world today, then, in general, not in any of the most developed civilized The country will not have enough such opportunities. Therefore, our task as doctors is, first of all, to outline for each patient, in each specific clinical situation, our own reasonable algorithm of actions and our own reasonable list of those examinations that will help us diagnose pathology. Of course, even such a method - I say “even”, because there was a time when a lot of people put their faith in laparoscopy and believed that this was a method that allowed practically, well, almost in 100 percent of cases, to reach the nosological form - in fact in fact, without a doubt, it has justified itself in this sense quite relatively, because a very specific list of nosological forms or pathological situations allows us to identify, and laparoscopy does not always allow us to get out, as I already said, and as you and I know very well , to a specific nosological form.
And now a review, in general, ten years ago, but quite correctly, let’s say, carried out, showed that from 10 to 15% of patients who underwent laparoscopy, essentially, were left, let’s say, without a definite diagnosis, because Laparoscopy was not helpful in diagnosing the cause of abdominal pain in these patients. Of course, today, gastroenterology especially is still a field of medicine in which the scope of the examination is largely determined by whether the patient has symptoms of anxiety or does not have these symptoms of anxiety. And you and I, understanding, on the one hand, the seemingly banality of these symptoms of anxiety and, it would seem, their obviousness, on the other hand, we must clearly understand that such moments as the nocturnal nature of pain, as the onset of the disease after 50 years , such as the presence of oncological or organic diseases in the family, if we are now talking about intestinal diseases, this is inflammatory bowel disease celiac disease, this is fever and loss of body weight, these are changes in direct examination of the patient, changes in the size of organs, these are changes in laboratory parameters - and routine ones, and the results of instrumental research methods, they force us, of course, to examine patients in more depth, because these are signals and markers of organic pathology. If we talk about intestinal diseases in general, then, of course, the most common cause of chronic abdominal pain is irritable bowel syndrome.
We all know the criteria very well, since they have practically not changed since 2006, and we understand that the leading one here is precisely recurrent abdominal pain, which is associated either with the fact of defecation, or with a change in frequency, or with a change in the shape of stool. And we perfectly understand that in order to diagnose irritable bowel syndrome, these are all the criteria that are listed and which are recommended to us by the Rome recommendations, all these criteria must be very strictly observed. Then, indeed, with a clear history and consistency of these symptoms, the likelihood of irritable bowel syndrome is high. This is visceral pain, and chronic, with a complete absence of anxiety symptoms. Moreover, it is chronic, that is, they arose, these pain sensations and these disorders, within six months. At the same time, we understand that despite the fact that this nosological form is called a syndrome, it is, in general, an independent nosological form, and issues related to the pathogenesis of its occurrence, the pathophysiology of its occurrence, are repeatedly discussed and very actively studied.
In doing so, we understand that if we clearly meet the criteria, the likelihood of irritable bowel syndrome—this is data relevant to previous irritable bowel syndrome recommendations—is 93%. However, irritable bowel syndrome can be masked, so to speak, or combined with some other diseases. These include enteropathies, inflammatory bowel diseases, parasitic colitis, lymphocytic/allergic colitis, bacterial overgrowth syndrome, diverticular disease, and endometriosis. Moreover, we must understand that there may be several options here. On the one hand, these may be similar syndromes of irritable bowel syndrome and intestinal diseases, and the second very important point is that there may be an overlap, that is, the presence of both intestinal diseases of an organic nature and at the same time irritable bowel syndrome. That is, when we encounter symptoms that are included in the criteria for the diagnosis of irritable bowel syndrome, we must understand that symptoms of another disease may be hidden behind them, or this may be the intersection of organic pathology and purely functional pathology.
If we consider approaches to the treatment of irritable bowel syndrome, there are a lot of guidelines. One that is fairly widely cited and not the most recent is the American College of Gastroenterology. Antispasmodics occupy a significant place there, they have a fairly good, let’s say, level of evidence, and it is m-anticholinergics that are predominantly discussed, and selective m-anticholinergics, when they talk about evidence-based therapy for IBS. But, however, if we are talking about what we must first differentiate irritable bowel syndrome from, then according to the recommendations of the World Gastroenterological Organization, celiac disease and parasitic diseases are most similar to IBS. Therefore, in patients with classic IBS manifestations, without symptoms of anxiety, we must exclude celiac disease, we must also exclude parasitic diseases. And then the most alarming from the point of view of other organic diseases are patients who have persistent diarrhea. Now, if we look at celiac enteropathy, today there are quite clear diagnostic recommendations in the world. They are based on determining, first of all, antibodies to transglutaminase, in addition, on determining the level of endomysial antibodies and the characteristics of the HLA system.
But in any case, when we talk about enteropathy, this is, of course, visceral pain, this is persistent diarrhea syndrome, this is the presence of varying degrees of melaabsorption, although melaabsorption may be absent, and extraintestinal symptoms that are characteristic of celiac enteropathy. Approaches to the treatment of celiac enteropathy in general are quite clear, although in some cases, in the presence of abdominal syndrome, we also always think whether this is an overlap with IBS or whether abdominal syndrome is somehow associated with the actual course of enteropathy, although in general this is not the most characteristic of this pathology symptom. If we talk about inflammatory bowel diseases, here, in fact, there may also be two classic situations, and mainly when we are faced with Crohn's disease due to obstruction or deep inflammation affecting the mucous membrane, submucosal layer, reaching the muscle layer, there may be a reaction with side of nociceptive receptors, so pain may occur, and the second option is, of course, crossover, the coexistence of these two nosological units. Here is the coexistence of two nosological units - studies have shown that in the population 30% of patients with ulcerative colitis suffer from IBS-like syndromes, with Crohn's disease this situation is more common.
And in one of Drossman’s latest reviews on inflammatory bowel diseases, IBS-like syndrome, in addition to the fact that we are trying to relieve pain by prescribing specific therapy for the treatment of inflammatory bowel diseases, we also use a different approach to treat pain, namely - inclusion of antidepressant drugs, antispasmodics and drugs that affect motor skills. The next nosological form that we include in the range of differential diagnosis is the syndrome of bacterial overgrowth in the small intestine. If we look and remember once again the symptoms that are associated with this pathology, we see many similar symptoms to irritable bowel syndrome. This is the same visceral pain, in most cases chronic, and symptoms of anxiety are not always present in these patients. In any case, a lot is now being said and written about the intersection of IBS with bacterial overgrowth syndrome, and it occurs in a large percentage of cases, and the important point is that, of course, there is specific treatment directly aimed at this bacterial overgrowth, but in a number of cases, we must also stop the manifestation of an IBS-like symptom complex in these patients.
The next situation, which is by no means rare, is diverticular disease, and at the same time, of course, in a number of patients it can be asymptomatic, in some cases we may encounter diverticulitis or other complications of diverticular disease, and finally, there is the term “symptomatic diverticular disease.” disease" is the presence of chronic abdominal pain, a violation of intestinal passage, which is very similar to the manifestation of irritable bowel syndrome. If we talk about the features of abdominal pain with diverticulitis, then we understand that this pain is visceral, with the addition of a parietal component, if we are talking about significant thinning of the walls of this diverticulum. As a rule, there are symptoms of anxiety - these are such as fever, such as accelerated ESR, such as increased levels of C-reactive protein. The pain, as a rule, is local, intensifies with movement, which indicates that the parietal component of this pain is attached, and, of course, age, without a doubt, is very important.
If we talk about symptomatic diverticular disease, the question is debated - whether it is segmental colitis, or whether it is simply concomitant irritable bowel syndrome. There are a lot of ideas expressed, but, indeed, it is very similar to irritable bowel syndrome in its manifestations, except, of course, for age. Since we understand that diverticular disease is the lot of people in older age groups, here, of course, age plays a very significant role in order for us to suspect this particular pathology in our patients. If we talk about approaches to treatment, then in uncomplicated acute diverticulitis, pain relief is an important section, and it is discussed in the guidelines that exist in individual countries. It should be understood that non-steroidal anti-inflammatory drugs worsen the course of acute diverticulitis, therefore the emphasis in treatment was placed on predominantly selective anticholinergic drugs - they reduce the pressure in the intestinal lumen - and drugs of the 5-aminosalicylic series.
As for the symptomatic form of management of diverticular disease, management is essentially no different from the management of patients with irritable bowel syndrome. And then there is a large list of various other inflammatory, allergic diseases of the intestines, both the small and large intestines. This group of diseases can never be discounted, and we have repeatedly encountered colitis, making a differential diagnosis of inflammatory bowel diseases, and there, for example, it turned out to be yersiniosis, and it, too, may not have a subacute, but a chronic relapsing course, and, of course, ischemic colitis , and, of course, associated with drugs, which we often forget about, and microscopic colitis. Despite the fact that, in general, I have not made many of these diagnoses in my life, it is certainly impossible to completely discount them. I demonstrate here some points, without focusing on particulars, that for each of the forms of colitis there are its own diagnostic features, and in many ways they are associated with features, including morphological histological conclusions. But as for, for example, some forms of microscopic colitis, here is a review from ten years ago, which suggests that distinguishing it from irritable bowel syndrome is not always really easy.
Well, and finally, new nosological forms appear, such as intestinal syndrome of drug addicts. Today, this form claims to be an independent nosological form, it occurs in people dependent on drugs, and this is associated with a change in the threshold of pain sensitivity, and, of course, we understand perfectly well that if it does not, then in the near future it will give us very There are many problems from the point of view of both managing these patients and making a diagnosis, among other things. Thus, in general, if we talk about approaches to the treatment of abdominal pain in intestinal diseases, of course, we should, in those cases in which we can, try to eliminate the cause. Although, alas, we cannot always do this. Next, of course, we must eliminate abdominal pain. It reduces the quality of life and makes it difficult to examine patients. There are a number of different approaches to this, and in general, if you arrange them in stages, then these are non-steroidal anti-inflammatory drugs, analgesics, antispasmodics, then more intense, let’s say, more complex opioid drugs and surgical interventions, these are, of course, antidepressants , and speaking here about antispasmodic therapy, we must understand: on the one hand, the combined prescription of drugs is indeed considered as one of the ways to relieve pain, but in this regard, hyoscine butyl bromide has its strengths, since it has a tropism for the enteric nervous system, and besides, here is a study that is good because for abdominal pain, the effect of paracetamol, the No. 1 drug in the world for pain relief, specifically for providing symptomatic assistance, showed almost completely similar results, and therefore we consider this drug as a drug for relief abdominal pain.
Moreover, taking into account that the frequency of side effects practically does not exceed the frequency of side effects when taking a placebo, and bearing in mind that pain of any origin is alleviated or stopped when using this drug, plus quickly, plus a small number of side effects, and that’s all , of course, we must take into account. Of course, we can use anticonvulsants, but it must be said that more research on this matter has been carried out specifically in chronic pancreatitis. In some cases, we can resort to laparoscopic treatment in situations where we suspect the presence of adhesions as the cause of pain, but we understand that these are not adhesions as such, but are either a reaction from the mesentery or changes in motility from the intestines. But if we look at the studies that are more or less rigorous today, then in no more than 60-70% of cases we have any lasting effect from this manipulation.
Thus, today we must clearly understand, and we know this with you, that abdominal pain is one of the most important symptoms of intestinal pathology, certainly not the only one, but very important. One of its causes, if we talk about statistics, the most common, is irritable bowel syndrome, and it can either be an independent nosological form, or it can hide an organic disease, or it can simultaneously coexist with an organic pathology. The mechanisms of pain are different, therefore they use different drugs, different combinations in pain relief, but it seems to me that we must clearly understand that pain relief in the 21st century is an independent clinical task, and we must do everything so that our patients, Living in this world, one should not experience this pain, including those suffering from serious illnesses. A large number of drugs are used, and various other approaches, including surgical, endoscopic, and one of the well-studied group of drugs that can relieve pain both in monotherapy and in complex therapy is a group of antispasmodics, and among them, of course, the important hyoscine butyl bromide takes its place due to its safety, fairly good study and thanks to those studies that have shown the safety of its use over long periods of time, up to 3 months. Thank you very much for your attention.