Diagnostics
- The most informative endoscopy is esophagogastroscopy, which allows you to immediately take at least 6 pieces of damaged tissue for examination.
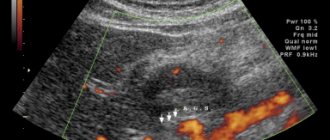
- Supplementing gastroscopy with ultrasound examination - endosonography will quite clearly determine the depth of penetration of the cancer process into the gastric wall.
- The extent of damage to the walls of the organ is determined by polypositional X-ray contrast examination.
- An abdominal CT scan will reveal metastases in the lymphatic system and clarify the involvement of surrounding tissues and organs in the malignant process.
- A mandatory examination before surgery is laparoscopy, which detects peritoneal carcinomatosis.
Prevention
Prevention is possible only if the causes leading to carcinoma are clear. Today, oncologists know a list of diseases in which the likelihood of developing a neoplasm in the mucous membrane is increased, but the root cause of malignant degeneration itself is unknown.
Prevention is limited to the treatment of underlying gastric diseases and regular monitoring of the course of benign processes. The leading screening method is gastroscopy, which allows you to assess the condition of the mucous membrane and take it for analysis.
For patients who have undergone primary treatment for gastric carcinoma, prevention is regular screening for early detection of tumor recurrence and metastases.
Stages of development of gastric carcinoma
Typically, cancer is graded according to TNM stages - from first to fourth. Each stage is characterized by a certain size of the primary lesion, which is designated by the letter “T”, and the degree of involvement of the abdominal lymph nodes – by the letter “N”. From stages I to III inclusive, metastases to other organs are excluded, that is, “M” is always only 0.
Schematically and simplified stages are interpreted as follows:
- The initial stages of development, when cancer cells have not penetrated further than the mucous membrane, are referred to as early gastric cancer, that is, stage one carcinoma or less - in situ.
- Metastasis to the lymph nodes, even with a tiny tumor, is at least the second stage.
- The exit of carcinoma through the gastric wall into the abdominal cavity is the third stage.
- Cancer metastases to other organs are the fourth.
Symptoms of gastric carcinoma
Early stages of cancer cause the same symptoms as any benign or inflammatory pathology of the gastrointestinal tract, without forcing the person experiencing discomfort to see a doctor.
Often there is not a single sign of illness at all, which is why it is so important to regularly perform endoscopic examination of the gastrointestinal tract during background processes.
The stomach stretches, masking the decrease in its capacity with a growing tumor, and the symptoms do not differ from a banal exacerbation of chronic gastritis; only the progressive loss of body weight with an increase in the volume of the abdomen can be alarming - evidence of carcinomatous contamination of the abdominal cavity with the formation of ascites.
The pain is typical for an ulcer; with stomach cancer, pain occurs when the nerve trunks of the abdominal cavity are sealed into the tumor conglomerate or neighboring organs are involved. More than half of patients notice signs of a common malignant process:
- weight loss,
- increase in belly size,
- vomiting after eating
- the appearance of lymph nodes above the collarbone or palpating a lump in the epigastric region.
Classification and varieties
In terms of cellular structure, the overwhelming majority of gastric neoplasms are represented by adenocarcinoma, which is typical for the entire gastrointestinal tract. Morphological variants are possible in the form of papillary or tubular, mucinous or signet ring cell adenocarcinoma.
The choice of the optimal treatment method is based not so much on the cell variety as on the degree of its aggressiveness, that is, differentiation, where the minimum is designated as “highly differentiated.” High malignancy is inherent in the poorly differentiated form.
Invasive gastric carcinoma is not a separate disease, it is a natural process of tumor development, when it is no longer an isolated colony of cancer cells in a separate area of the mucous membrane, but penetrates into the surrounding tissues, destroying everything that interferes with its advancement in depth and breadth, and has acquired the ability to metastasize.