Modern approaches to the treatment of gastric and duodenal ulcers
Peptic ulcer of the stomach and duodenum is traditionally one of the most common and widely discussed diseases of the gastrointestinal tract. In recent years, a large amount of information has appeared that has made it possible to radically reconsider the problems of etiology, pathogenesis, standards of diagnosis and treatment of this pathology. From a modern point of view, any gastroduodenal ulcer is considered as a kind of imbalance between the factors of aggression acting on the mucous membrane of the upper gastrointestinal tract and the factors of its protection. Factors of aggression include hypersecretion of hydrochloric acid, which has been known for a long time. Associated with it is the overproduction and hyperactivation of pepsinogen, impaired gastroduodenal motility, smoking, taking a number of medications, primarily nonsteroidal, anti-inflammatory and glucocorticosteroids, and, of course, infection with Helicobacter pyloricus, which is currently considered the most important etiological factor of peptic ulcer disease. All these factors can lead to the development of gastroduodenal ulcers if their effect on the mucous membrane is stronger than the protective factors. The most important protective factors include: secretion of gastric mucus, which is located on the surface of the mucous membrane; production of bicarbonate ions and their reverse diffusion in the mucous membrane, leading to the neutralization of free protons resulting from the dissociation of hydrochloric acid molecules; regenerative potential of epithelial cells; blood flow in the mucous membrane of the stomach or duodenum and the synthesis of cytoprotective prostaglandins.
A little more detail about Helicobacter pylori infection. These are gram-negative, non-spore-forming aerophilic bacteria of a peculiar spiral shape, with the presence of flagella at one of the poles, which are characterized by extremely harsh conditions that ensure their optimal growth. The temperature is about 37 degrees, high humidity, the pH level is from 4 to 6, which practically makes it possible for this microorganism to actively reproduce exclusively in the mucous membrane of the stomach and duodenum. And, despite the fact that the routes of transmission - fecal-oral, oral-oral - are essentially possible only in very narrow social groups with close household contact, the source of this infection is, of course, a sick person. After the discovery and description of Helicobacter pylori, several important, perhaps even radical changes in our ideas about the etiology and pathogenesis of peptic ulcer disease occurred. In 1983, the role of this infection in the development of chronic gastritis was demonstrated for the first time quite convincingly. In 1994, the first national recommendations for the treatment of peptic ulcer disease, aimed at suppressing this infection, were issued in the United States. In 1996, the first Maastricht Agreement appeared with recommendations for the diagnosis and treatment of Helicobacter Pylori infection, 5 years later - the second and, finally, the third Maastricht Agreement, which essentially described the modern standards for the diagnosis and treatment of peptic ulcer disease. A large number of studies were conducted in which the destruction of Helicobacter Pylori was combined with such a pronounced reduction in the frequency of relapses of peptic ulcers, stomach and duodenum, which could not be provided by maintenance therapy with antisecretory drugs carried out in the so-called pre-Helicobacter period. It is also important that in recent years extremely interesting data have been accumulating on the genetic characteristics of peptic ulcer disease associated with both the host genome and the genome of Helicobacter Pylori. In particular, a fairly variable risk of developing peptic ulcer disease in infected people has been described, depending on certain ethnic groups. For example, Japan is characterized by a significantly higher incidence of the disease. A gene has been described that is associated with a fairly high incidence of duodenal ulcer. In addition, a gene has been described that is associated with a high risk of developing atrophy of the gastric mucosa and intestinal metaplasia, morphological signs of chronic gastritis developing in response to Helicobacter Pylori infection. The connection of these genetic changes with certain genetic polymorphisms of the Helicobacter Pylori infection itself has been proven, when combined, the risk of developing peptic ulcer disease, in particular duodenal ulcers, increases enormously.
All this must be taken into account for the diagnosis and treatment of peptic ulcer disease. However, the goals of therapy for peptic ulcer disease have long been well defined. This, of course, is the elimination of pain and dyspeptic syndromes, healing of ulcerative defects within a controlled period, the maximum possible extension of the period of remission and the prevention of exacerbations. From a modern point of view, these goals cannot be achieved without implementing the basic principle of drug therapy for peptic ulcer disease, the principle of eradication, which involves the complete destruction of all vegetative and coccal forms of this bacterium in the mucous membrane. At the same time, the eradication threshold, which is currently recommended by international standards, should be at least 80. What does this mean? This does not mean that the treatment regimen used in a particular patient should provide 80% or more eradication of Helicobacter Pylori, but that in the population in which a particular regimen or treatment method is used, there should be no patients with complete eradication less than 80%. Achieving eradication, significantly reducing the incidence of relapses of peptic ulcer disease, not only improves the quality of life of patients, but also significantly reduces the costs associated with the treatment of peptic ulcer disease.
To carry out anti-Helicobacter therapy, it is necessary to take into account a number of very important features. First of all, there must be a correct diagnosis. Further, it is necessary to overcome the resistance of Helicobacter Pylori to antibacterial drugs, to combat the ineffectiveness of eradication therapy regimens, which gradually appears, with side effects. And, of course, it is necessary to take into account the cost and economy of treatment.
To resolve these issues, international recommendations were developed to regulate the actions of clinicians in the treatment of peptic ulcer disease. We have already talked about the effectiveness of eradication schemes. Of course, these regimens should be well tolerated, fairly easy to use, and cost-effective. Back at the Maastricht-2 meeting in 2000, a range of indications for which eradication should be carried out was determined (the level of evidence is indicated in brackets):
- Gastric ulcer, duodenal ulcer in the stage of exacerbation or remission, including complicated peptic ulcer (1);
- Chronic antral gastritis (2);
- MALT lymphoma (2);
- Atrophic gastritis (2);
- Condition after gastric resection for cancer (3);
- Eradication of H. pylori is indicated for persons who are close relatives of patients with gastric cancer (3).
What features of the treatment of peptic ulcer disease can we determine today? They proceed largely from the recommendations of the last meeting, which took place in March 2005. The Third Maastricht Agreement defined the necessary conditions for the use of first-line therapy. The first line includes the so-called triple therapy, based on a proton pump inhibitor, clarithramycin and amoxicillin. It was postulated that it is advisable to use this regimen only in those populations where Helicobacter Pylori strains have resistance to clarithramycin of no more than 15-20%, and to metronidazole, if it is used instead of amoxicillin, no more than 40%, otherwise this regimen is ineffective. Separately, it was said about therapy, which was previously classified as second-line therapy, or quadruple therapy. Proton pump inhibitor, tetracycline, bismuth drug and metronidazole. If previously this regimen was used exclusively as an alternative when first-line therapy was ineffective, then at Maastricht-3 it was noted that quadruple therapy can also be used as first-line therapy. This is primarily due to the increasing resistance of Helicobacter Pylori to the antibacterial components of the triple therapy regimen. So-called backup regimens have also been proposed, including drugs such as levofloxacin, furozolidone, and rifampicin. All of these regimens are based on the dual administration of a proton pump inhibitor with two antibacterial drugs. Often this is a combination of amoxicillin with tetracycline, amoxicillin with furozolidone, levofloxacin with furozolidone or rifampicin. Today, these schemes are being actively studied. We do not yet have sufficiently convincing data on the threshold of their effectiveness, but, nevertheless, these schemes may turn out to be very promising.
Duration of treatment. What clinicians have been talking about for a long time, based on their experience and reflection, is reflected in the Maastricht 3 recommendations. It was noted that 14-day eradication therapy is approximately 12% more effective than 7-day treatment regimens. Therefore, today we can recommend prolongation of eradication therapy to at least 12-14 days. It is noteworthy that all regimens use proton pump inhibitors as the cornerstone of treatment. This is due to certain pharmacodynamic characteristics of this group of drugs. In particular, a certain, although not very pronounced, intrinsic activity of proton pump inhibitors, bactericidal against Helicobacter Pylori, has been proven in vitro. It varies among the drugs in this group. Much more important is that all proton pump inhibitors, by raising intragastric pH, create better conditions for the action of the antibacterial components of eradication schemes: amoxicillin, clarithramycin, which turn out to be much more stable in an environment with such pH values and last longer. An increase in pH from 2 to 7 units increases the half-life of amoxicillin by 11 times, clarithramycin by 200 times. Of course, this increases the effectiveness of such a combination. Another important thing is that at such pH values, active reproduction of Helicobacter Pylori begins, and it is the dividing bacteria that are affected by the antibacterial components of the eradication scheme. And therefore, in combination with antibacterial components, proton pump inhibitors are necessary for eradication therapy. They are also necessary in the future, since they neutralize the effect of another important factor of aggression towards the gastroduodenal mucosa, hydrochloric acid. By reducing the level of gastric acidity, proton pump inhibitors help reduce the effect of this damaging factor on the gastroduodenal mucosa. That is why it is necessary to continue monotherapy with proton pump inhibitors after completing the course of eradication therapy to ensure adequate epithelization of the mucous membrane.
The question arises: which proton pump inhibitor to choose from the wide range of drugs in this group available today? I would like to draw your attention to the fact that, according to most large independent international studies, we have several proton pump inhibitors that, compared to others, have a significantly more pronounced and longer-lasting antisecretory effect. The drug with the maximum severity of the antisecretory effect in the dosages in which it is used is considered to be esomeprazole (Nexium), which is an optical isomer of omeprazole. When compared with other proton pump inhibitors, this drug demonstrates a significantly longer and more pronounced antisecretory effect. It is also important that esomeprazole is characterized by a maximum area under the concentration-time curve, which quantitatively characterizes the severity of this antisecretory effect. Does this make any difference? Yes, of course, in a number of cases this matters. In particular, in a study in patients suffering from duodenal ulcers, which compared esomeprazole and omeprazole, it was shown that 1-week triple therapy with esomeprazole provided such a high level of suppression of gastric secretion that it was possible to achieve all goals of treatment of peptic ulcer without subsequent 3-week intake of a proton pump inhibitor as monotherapy. Similar results, which are a direct consequence of the pronounced antisecretory effect of esomeprazole, were obtained in a large number of different clinical studies. Specifically, the PAIR PROTOCOL and ITT studies compared esomeprazole with pantoprazole. According to the results of these studies, the esomeprazole group had a significantly higher eradication rate than the pantoprazole group. According to a meta-analysis that compared the effectiveness of a triple therapy regimen based on esomeprazole and other proton pump inhibitors, a single dose of esomeprazole at a dose of 40 mg was no less effective than a double dose of 20 mg. Although there was a tendency for more pronounced end results with twice the dose, these data were unreliable, and it can be said that a single dose of 40 mg esomeprazole is quite sufficient. And most importantly, side effects with this regimen were significantly less common than with regimens with other proton pump inhibitors.
What are the rules for using antiulcer antibiotic therapy? If, at the end of therapy, there is no complete cure, eradication of Helicobacter Pylori does not occur, it is not recommended to repeat this regimen, since, most likely, we are dealing with an antibiotic-resistant strain of Helicobacter Pylori, and it is necessary to immediately transfer the patient to another regimen. If the use of one and then another treatment regimen does not lead to eradication, the sensitivity of the Helicobacter Pylori strain to the antibiotics included in these regimens should be determined in order to select one of the reserve regimens. The appearance of bacteria in the patient’s body a year after treatment is regarded as a relapse of infection, not reinfection, and requires the appointment of a more effective backup eradication regimen.
Thank you for your attention!
Anti-Helicobacter eradication therapy - a way out of a dead end or a movement deeper into the labyrinth?
The level of development of modern medicine, like any other direction in science, depends on the amount of knowledge and skills accumulated by many dozens of previous generations. At the same time, it should be recognized that we, like the contemporaries of Hippocrates, move forward through trial and error. We can agree that the number of these errors has decreased, but overall it is still very high. It is enough to mention the fact that in our time in every section of medicine, recommendations on the diagnosis and treatment of various diseases are revised with a frequency of 3-5 years. Previously, the revision of established ideas took centuries and even millennia.
The discovery of antibiotics is, without exaggeration, one of the greatest achievements of medicine, since their use has radically reduced mortality from infectious diseases throughout the world. At the end of the twentieth century, gram-negative, non-spore-forming bacteria – Helicobacter pylori – were identified on the mucous membrane of the stomach and duodenum of patients with peptic ulcer disease. The inclusion of antibiotics with anti-Helicobacter activity in the treatment program for gastroduodenal ulcers, in combination with proton pump blockers, made it possible to achieve a maximum reduction in the time of ulcer scarring, which in almost 100% of cases was accompanied by eradication of the bacterium. This fact served as the basis for the conclusion that H. pylori in combination with hyperchlorhydria are the main causes of peptic ulcer disease. Thus, peptic ulcer disease began to be talked about as an infectious disease. However, the treatment of such patients is still carried out not by infectious disease specialists, but by gastroenterologists. Since the recovery of patients in infectious diseases departments is always preceded by the eradication of the infectious agent responsible for the disease, this approach was extended to patients with peptic ulcer disease.
For a long time, there was a strong belief that with the eradication of H. pylori, peptic ulcer disease would also be eliminated. More than 30 years have passed since the discovery of the microorganism, and therefore it became possible to draw some conclusions. Let us refrain for now from our own assessments and turn to the statement of I.V. Maev is one of the zealous adherents of the version about the main role of H. pylori in the pathogenesis of peptic ulcer disease. “Despite many years of active struggle ... against H. pylori infection, the prevalence of peptic ulcer disease both in our country and in most countries of the world is not decreasing. The frequency of its serious complications (perforation, penetration, bleeding, etc.) remains consistently high (at the level of 10%)” [1].
The above phrase is actually an authoritative recognition that the statement about the leading role of H. pylori in the pathogenesis of peptic ulcer disease is erroneous. Indeed, in a significant proportion of cases, peptic ulcer disease develops without any involvement of H. pylori (H. pylori-negative forms of the disease). In the USA, the incidence of peptic ulcer disease not associated with H. pylori varies from 39 to 52%, and in Australia it reaches 45% [2,3]. The data presented clearly demonstrate that the role of H. pylori has been overly demonized without sufficient justification.
Since the principles of treatment of gastroduodenal ulcers are closely linked to the idea of the role of H. pylori, the question arises: has this affected the algorithm for antibacterial therapy of patients? This question can generally be answered in the affirmative. Treatment regimens are indeed adjusted every few years. The latest recommendations are formulated in the Maastricht V-Florence Consensus [4]. A significant part of all five versions of the Maastricht consensus is devoted to consideration of the question: what to do if one or another treatment regimen is ineffective? Accordingly, in the latest version, as in the four previous editions, tactics for overcoming H. pylori resistance to the antibiotics used are mainly discussed. At the same time, the strategic question about the advisability of mandatory achievement of H. pylori eradication does not even arise; it has been automatically, for more than 30 years, transferred from one recommendation to another, although, as already noted, the incidence of peptic ulcer disease on the planet has not decreased over this period. Moreover, the new recommendations, without sufficient evidence, expand the range of diseases and syndromes for which eradication therapy is recommended.
Recently, on the pages of this magazine Y.S. Tsim Merman published a discussion article in which he cited a number of facts casting doubt on the exaggerated role of H. pylori and the adequacy of the strategy of conservative treatment of gastroduodenal ulcers. Taking into account our own experience, we fully share the point of view of Ya.S. Zimmerman that the authors of the “Maastricht Consensus” essentially monopolized the right to determine indications for eradication of H. pylori and methods of eradication therapy, proclaiming a strategy for the total elimination of H. pylori (test and treat strategy: identify and destroy!), which is scientifically unproven and practically impossible [5]. We are firmly convinced that such an approach is one-sided, erroneous and requires taking into account alternative facts. Taking into account what is stated in this article, we will try to dwell in more detail on controversial issues related to the strategy of anti-Helicobacter eradication therapy.
In contrast to the statement about the main role of H. pylori in the pathogenesis of gastroduodenal ulcers, we consider it necessary to recall the well-known fact established by V.Kh. Vasilenko (1970) - “Ulcers heal with treatment, without treatment and despite treatment” [6]. Taking into account the fact that in a significant proportion of patients, the onset of the disease is possible even in the absence of H. py lori, this observation convincingly indicates the existence of causes that play a more important role in the pathogenesis of gastroduodenal ulcers than the presence of the microbe. We believe that in the pathogenesis of gastroduodenal ulcers, among the numerous risk factors, the leading ones are “non-modifiable”: heredity, gender and age of a person. The direct implementation of their role is carried out due to the existing congenital or acquired local vascular hypoplasia in the duodenum or stomach, which also belongs to the category of non-modifiable factors [7]. In addition to non-modifiable factors, a huge number of factors that are considered “modifiable” play an important supporting role in the pathogenesis of gastroduodenal ulcers; these include H. pylori. Taking into account the pronounced positive response to anti-helicobacter therapy, there is reason to conclude that among the modifiable factors, H. pylori plays a major role.
The experience of the last thirty years has shown that eradication of Helicobacter, reducing the time of scarring of ulcers, simultaneously leads to a decrease in the ratio of gastroduodenal ulcers associated and not associated with H. pylori, but at the same time, contrary to expectations, does not lead to the elimination of peptic ulcer disease [8] . Of great interest are the observations of surgeons who have found that the relapse rate after successfully performed organ-saving operations (trunk vagotomy with economical resection of the ulcer) is 0% for more than 25 years after the intervention. At the same time, positive H. pylori status in operated patients is detected with the same frequency as in the population [9,10]. It is important to note the increase in mortality from complications of long-lasting gastroduodenal ulcers, which gives reason to reassess the indications for elective surgical treatment for these conditions. The above examples clearly demonstrate that in a significant number of cases, successful surgical removal of part of the wall of the stomach or duodenum, including an area of local vascular hypoplasia, is a much more effective measure than eradication of H. pylori.
The negative paradox of the problem under discussion is that to date this microbe, without sufficient grounds, is considered as the main cause of a number of other diseases. Indications for their eradication therapy were formulated by the Maastricht II consensus. Subsequent consensus documents additionally indicated a number of new pathological conditions, for which eradication therapy was also recommended. To date, the indications for diagnosis and treatment of H. pylori are the following [4,11]:
- peptic ulcer: in the stage of exacerbation and remission at the time of treatment, in history, in first-degree relatives;
- chronic gastritis;
- functional dyspepsia;
- long-term treatment with proton pump inhibitors (gastroesophageal reflux disease, taking non-steroidal anti-inflammatory drugs, glucocorticosteroids, aspirin, anticoagulants);
- stomach cancer in first-degree relatives;
- early stomach cancer; • the patient's wishes;
- fear of stomach cancer; • first generation emigrant from regions with a high incidence of infection;
- unexplained iron deficiency anemia, idiopathic thrombocytopenic purpura, vitamin B12 deficiency.
This ignores the fact that this approach is in conflict with ideas about the pathogenesis, features of the course, treatment and outcomes of classical obligate and opportunistic infections [12]. It is known that the biomass of microbes populating the gastrointestinal tract of an adult is 2.5–3 kg or more and includes up to 450–500 species. About 90% of this microbiocenosis is represented by obligate (obligatory) normal microflora, which performs many vital functions [13]. Without exaggeration, the importance of this microflora is comparable to the role of such an important organ as the liver. The rest of the microbiocenosis is represented by facultative (possible, optional) microflora, which is often found in healthy people and is opportunistic [14]. Microorganisms representing a large group of fungi, bacteria, protozoa and viruses are considered opportunistic pathogens. They are normal inhabitants of the skin and mucous membranes, coexisting peacefully with the human body, which indicates that the host's immune system does not perceive them as a threat and behaves neutrally. At the same time, they are able to exist in the environment for a long time.
H. pylori belongs to the category of opportunistic infections. The peculiarity of microorganisms of this type is that they can remain in the human body for many years and even a lifetime without showing signs of any aggression. These infectious agents exhibit aggressive properties only under conditions of passive penetration into the internal environment in large quantities and (or) a sharp decrease in general and local human immunity (violation of the integrity of the integument, bactericidal activity of secretions, suppression of the phagocytic reaction, reduction in the number of antagonist microbes, etc.) . This is due to the fact that opportunistic microbes, unlike obligate pathogenic microbes, do not have the factors of active penetration into the internal environment, suppression of the body’s defenses, and do not release exotoxins. They exert a pathogenic effect on the body with the help of endotoxin and toxin enzymes [12].
It is important to note that according to Ya.S. Zimmerman et al., in 90.5% of patients with peptic ulcer, along with H. pylori, the periulcerous zone is colonized by 93 types of microorganisms (streptococci, fungi of the genus Candida, enterobacteria, corynebacteria, etc., most often in the form of microbial associations) [15,16] . The term “opportunistic microorganisms” is largely arbitrary, since it is hardly possible to draw a clear line distinguishing these pathogens from obligate pathogens. Nevertheless, we consider it necessary to express the point of view that the category of obligate pathogenic agents should include those infectious agents that comply to the maximum extent with the postulates of Robert Koch (1890). They state that the causative agents of certain infectious diseases are those microorganisms that:
- constantly found in the body of sick people (or animals) and absent from healthy ones;
- the microorganism must be isolated from a sick person (or animal), and its strain must be grown in a pure culture;
- When infected with a pure culture of a microorganism, a healthy person (or animal) becomes ill.
These patients are contagious, so they need to be isolated from others and comply with the requirements of the anti-epidemic regime and should receive treatment in specialized infectious diseases departments. In such cases, the requirement to seek, without fail, the eradication of the infectious agents that caused the disease, seems convincing and quite justified.
Thus, in the occurrence of the listed pathological conditions, H. pylori plays the role of an important modifiable, but not the main risk factor. In this regard, the statement that for all of the listed conditions anti-Helicobacter therapy should be eradicative is highly doubtful. The accumulated world experience allows the empirical use of antibacterial drugs immediately after diagnosis for diseases associated with opportunistic flora (pneumonia, biliary and urinary tract infections, etc.). At the same time, the results of previous epidemiological studies in the region are taken into account; treatment of patients in this category is carried out outside the infectious diseases hospital - in general therapeutic, surgical and other departments. Often, as a result of treatment, it is possible to achieve eradication of the agent involved in the occurrence of pneumonia or another similar disease, but the task of necessarily achieving such a goal is not worth it. Moreover, antibiotics are stopped long before pneumonic infiltration and the main laboratory and clinical manifestations are eliminated. Thus, the main goal of treating diseases associated with opportunistic flora is not the eradication of opportunistic bacteria, but the achievement of clinical recovery in acute illness or remission of a chronic disease. The fundamental fact is that after recovery, the task of monitoring the degree of eradication of the causative agent of the disease is not set; moreover, after successful completion of treatment, the causative agent often remains unknown [17].
The lack of convincing evidence of the feasibility of eradicating H. pylori in gastroduodenal ulcers makes the statement about the need to achieve the same goal in other diseases listed above even less justified. First of all, chronic gastritis and functional dyspepsia associated with H. pylori and gastric cancer deserve discussion. It is believed that during the natural course of H. pylori-associated chronic gastritis, the orderly system of cellular renewal of the gastric mucosa is disrupted in 1-2% of patients. This leads to atrophy and progression of morphological changes in the mucous membrane, which contributes to the formation of gastric cancer (“Correa cascade”) [18].
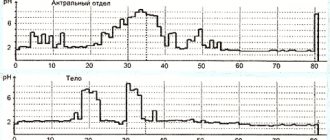
The incidence of gastric cancer varies approximately 10-fold geographically, which may indicate a more important role of ethnic and hereditary predisposition. Gastric cancer is very common in East Asia (Japan and Korea), South America and Eastern Europe and much less common in South Asia, North America, North and East Africa, Australia, and New Zealand [19,20]. Of particular interest is the fact that in the African population, where the prevalence of H. pylori is highest (up to 97%), gastric cancer is minimally common, and in Japan, where the prevalence of H. pylori is about 43%, the incidence of cancer in this localization is high . Taking into account the above, it is difficult to agree with the statement that H. pylori infection is a group 1 carcinogen for humans [21]. Doubt about the validity of this statement increases even more if we look at the statistics on the prevalence of stomach cancer in Russia for the period 2005-2015. (Fig. 1) [22].
Rice. 1. Prevalence of stomach cancer (per 100,000 population) in Russia in 2005-2015. (Kaprin A.D., Starinsky V.V., Petrova G.V., 2016)
The data presented clearly indicate that the introduction of an eradication strategy into practice does not help reduce the prevalence of gastric cancer in Russia. Moreover, there is a statistically unreliable but steady increase over the period 2005-2010, which makes the statement about the advisability of eradication therapy to prevent the occurrence of this type of cancer pathology questionable.
Of great interest is a study that was conducted over about 7.5 years in a Chinese province where there is a high incidence of stomach cancer. Patients at comparable risk for gastric cancer were randomized to placebo (n=813) or eradication therapy (n=817). In the first 5 years, the cumulative incidence of gastric cancer was higher in the placebo group, but by the end of the study its incidence in the compared groups did not differ significantly [23]. The data presented clearly demonstrate that eradication therapy can slow down the rate of progression of gastric cancer for several years, but is not able to prevent it. The literature provides evidence that eradication therapy is an effective element of cancer prevention only in cases where it is prescribed before the development of preneoplastic conditions. It has been established that stages III and IV of atrophic gastritis according to the OLGA system are associated with an increased risk of developing gastric cancer [24]. Eradication therapy in patients with intestinal metaplasia does not lead to the reverse development of the latter; it can only slow down the progression of metaplasia to neoplasia.
All eradication therapy regimens formulated in the five Maastricht recommendations are not offered as recommendations that can be used, but are imputed in the form of obligations that must be fulfilled. In this regard, it is of interest to observe the prevalence of peptic ulcers among people involved in the production of antibiotics. It was found that the average age of patients with duodenal ulcers (39.8 years) employed in the production of antibiotics corresponded to that of patients with duodenal ulcers in the control group, whose work was not related to this production. At the same time, the average age of patients with gastric ulcers in the main group (38.7 years) was lower than the age characteristic of persons with ulcers of this localization (40-50 years) in the control group. This suggests that prolonged human contact with antibiotics leads to an increase in the resistance of opportunistic flora, which ultimately contributes to the earlier onset of gastric ulcers in people whose work is related to the production of antibiotics [25].
The total prevalence of chronic gastritis and functional dyspepsia is comparable to the prevalence of H. pylori in the population (at least half of the population). It is known that during the natural course of chronic gastritis, 1-2 out of 100 people may die from stomach cancer. At stages III and IV of atrophic gastritis, eradication therapy is useless. The requirement for eradication to be carried out at earlier stages means that at least 50% of the world's population should be included in the treatment program. At the same time, the previously cited examples indicate that, firstly, eradication therapy will not stop the progression of either chronic gastritis or functional dyspepsia. Secondly, in 1-2 out of 100 people with chronic gastritis, the tumor may develop several years later than in the natural course of the disease, but they will die, in any case, from stomach cancer. As for the remaining 98-99 patients, they are, in fact, turning into a “living thermostat-incubator” for growing a huge number of new strains of bacteria resistant to new antibiotics.
Concluding the discussion of the role of H. pylori in the pathogenesis and treatment of H. pylori-associated diseases, a number of conclusions can be drawn that give reason to doubt the sufficient validity and feasibility of the eradication therapy strategy for these diseases. If we focus on the prevalence of H. pylori and associated diseases, the situation as a whole can be considered as a formidable pandemic sweeping the entire planet. However, upon closer examination, it becomes clear that the comparison with the pandemic is purely formal. As you know, a classic example of a pandemic is the “Black Death,” or plague epidemic, which was observed in Europe in the 14th century. It rampaged almost simultaneously across Africa and Eurasia. The consequences of the infection were terrible: Europe was devastated, having lost, according to some estimates, up to 40% of the population; several hundred cities and villages died out in China and India; the number of dead in Africa cannot be counted at all. Thus, one of the main features of the pandemic is not only the high prevalence of infection in the population, but also the extremely high risk of death if infected. At the same time, the absolute majority of people with H. pylori-associated diseases are represented by patients with chronic gastritis, who do not even know that they have either gastritis or H. pylori. Gastritis itself poses a threat to life in only 1-2 out of 100 people. Given the facts presented, the term pandemic is not appropriate for this situation.
The next feature is that the causative agents of pandemic diseases, without exception, belong to the category of obligate pathogens, while H. pylori is opportunistic. It is important to emphasize that in people who have recovered from infectious diseases, the immune system develops a barrier against a specific pathogen: persistent, unstable or lifelong. At the same time, not all those who have recovered from a classic infectious disease caused by an obligate pathogen develop lifelong immunity. For example, diseases that provide lasting immunity for life include rubella, mumps, hepatitis A, diphtheria, measles, polio, and chickenpox. Unstable or short-term immunity is formed after diseases such as whooping cough, hepatitis B, influenza, tuberculosis, typhoid fever, and dysentery. The immune system is neutral towards opportunistic pathogens, so there is no reason to deny that H. pylori, after eradication, can repeatedly return to the same person.
Eradication of an obligate pathogenic pathogen is the same as complete recovery of the infectious patient, while eradication of H. pylori, as time has shown, leads only to a reduction in the time of scarring of the ulcer and to a longer remission, but not to the elimination of the disease itself. The prevalence of stomach cancer, as noted earlier, not only does not decrease, but continues to increase. Taking into account the above, in case of acute occurrence or recurrence of gastroduodenal ulcers, anti-Helicobacter therapy should be considered appropriate. In this case, the main criterion for the effectiveness of treatment should be considered the achievement of remission of the disease (relief of clinical manifestations, scarring of the ulcer). However, since eradication does not guarantee the prevention of recurrence of H. pylori infection and is not accompanied by the elimination of “H. pylori-associated diseases,” a treatment strategy that prescribes mandatory eradication of Helicobacter should be considered erroneous.
By selectively using only those data that indicate a hypothetical benefit of H. pylori eradication and ignoring alternative points of view, the Maastricht recommendations continue to strongly promote the rationale for achieving eradication. However, since the microbe quickly and successfully develops resistance to new classes of antibiotics, in the near future there may be recommendations to include antibiotics in eradication regimens that are currently considered reserve. Ultimately, the attempt to “link” all new diseases to Helicobacter will lead to the fact that at least half of humanity may be involved in eradication therapy. By persisting in the desire to kill the opportunistic microbe without fail, we risk killing the host without ridding him of the disease for which eradication was carried out. Turning to the basic provisions of medical science, we consider it possible to formulate the main debatable question. Do existing approaches to anti-Helicobacter eradication therapy comply with the rule from the Hippocratic Oath – “First, do no harm”?
Yu.V. Vasiliev
TsNIIG, Moscow
Peptic ulcer is one of the most common diseases of the upper gastrointestinal tract. The recurrent course of this disease, the high percentage of patients' disability, the slight tendency to reduce the incidence of severe complications (in the form of bleeding, perforation or penetration of ulcers into neighboring organs), which can lead to the death of patients, force researchers to clarify the etiological and pathogenetic aspects of peptic ulcer disease, to develop new and/or improve already known methods of treating patients.
The main pathogenetic aspects of peptic ulcer disease The pathogenesis of peptic ulcer disease is quite complex and in many ways not entirely clear. According to modern concepts, peptic ulcer of the stomach and duodenum [3, 5] is a heterogeneous, chronic, relapsing disease with varying frequency, with different variants of course and progression, leading to serious complications in some patients. Genetic predisposition, imbalance between aggressive and defensive factors, and the presence of Helicobacter pylori (HP) are the three main factors currently most often considered as the basis for the appearance and recurrence of peptic ulcer disease [1, 3, 5]. It is possible that there are individually different complexes of resistance factors [6], obviously varying in their intensity and duration of action depending on genetic, age-related, hormonal and other factors, including the ability to form antibodies to HP, allowing them to neutralize or reduce The “aggressiveness” of a particular set of risk factors, including those not listed above, largely determines the likelihood of a peptic ulcer and its recurrence, variants of the course of a peptic ulcer, including the frequency and intensity of clinical manifestations, the occurrence of complications, etc. By itself a single risk factor (or even one or another complex of them) cannot lead to the occurrence of peptic ulcer disease or its relapse. A nonspecific additional effect (nervous or psycho-emotional stress, change in quality of life and/or environmental conditions, etc.) is also necessary for the occurrence of peptic ulcer disease or its relapse. However, such additional exposure in itself cannot lead to peptic ulcer disease. Along with many factors that, alone or in some combination, may underlie the onset and progression of peptic ulcer disease, one of the important factors determining its development is periodic imbalances between the factors of aggression and defense. Among the factors of aggression, hydrochloric acid plays a significant role. The following factors particularly predispose to the development of peptic ulcer, especially of the duodenum:
• high level of maximum acid production of the stomach; • increased levels of pepsinogen in the blood serum (inherited in an autosomal dominant manner); • excessive release of gastrin by G cells in response to nutritional stimulation.
Among the protective factors most often identified [2]:
• sufficient secretion of bicarbonates; • muco-epithelial barrier (gastric mucus plus cell integrity), which is capable of neutralizing acid to a greater or lesser extent (depending on the individual characteristics of patients) and inhibiting peptic digestion; • cellular regeneration of the epithelium; • endogenous prostaglandins; • sufficient blood supply to the mucous membrane; • structural resistance of connective tissue glycoproteins to proteolysis; • neutralizing ability of the “mixture”, consisting of the contents secreted by the duodenum, gall bladder and pancreas; • antrumduodenal acid “brake”, i.e. a chain of humoral reflexes that provide inhibition of hydrochloric acid at the end of digestion.
One of the important mechanisms for the development and chronicity of ulcers, especially in gastric ulcers, is tissue hypoxia with subsequent disruption of bioenergetics and oxidative processes. Oxygen-dependent processes express the basis of cell metabolism, determining the intensity of reactions of accumulation and transformation of energy, lipid peroxidation, synthesis of intracellular regulators - cyclic nucleotides, eicosamines, etc. Study of the intravital state of the mucous membrane of the upper gastrointestinal tract, according to endoscopic examination and histological examination of materials targeted biopsies began more than 45 years ago, primarily in the study of peptic ulcer disease. One of the causes of this disease, in particular bacteriological, was established back in 1981 by the Australian pathologist R. Warren. There has been interest in elucidating the role of this bacterium in the pathogenesis of duodenal ulcer [4, 10, 11]. Currently, there are a large number of publications that claim a direct connection between peptic ulcer disease and HP. This microorganism has recently been often considered as the main etiological factor in peptic ulcer disease associated with HP. However, this is still a hypothesis accepted as an axiom and requiring fairly convincing confirmation. The following is often cited in favor of arguing for a connection between peptic ulcer disease and HP:
• the majority of patients with peptic ulcer disease have HP during the period of exacerbation; • carrying out eradication therapy leads to healing of ulcers, reducing the time of treatment for patients; • eradication therapy, leading to the elimination of HP, can reduce the activity of gastritis and even eliminate it in some patients, i.e., achieve a normal state of the gastric mucosa.
It has now become known that HP itself causes minor damage to the epithelium. The main thing in ulcerogenesis is changes in signaling systems caused by NR. Typically, the complex of signaling systems and mechanisms includes cytokines secreted by various epithelial cells of the mucous membrane that come into contact with NR, the greatest importance among which is currently given to interleukin-8, which changes the parameters of chemotaxis, chemokinesis, aggregation and release of lysosomal enzymes from neutrophils. In order to explain the fact of the frequent periodic absence of HP in patients with peptic ulcer disease, a hypothesis was proposed [1, 3], according to which, even in the absence of HP, the changes in signaling systems previously included by it continue to act sluggishly, without generally disturbing a certain biological balance. The activity of signaling systems increases significantly when a significant additional impact appears, which is possible both in the presence and absence of NR during this period. This leads to the occurrence of a peptic ulcer or its relapse.
Diagnosis and therapy of peptic ulcer For the first time, indications for eradication therapy of peptic ulcer were discussed at the World Congress of Gastroenterologists in Australia (Sydney) in 1990 [15]. At the same time, the feasibility of carrying out eradication therapy for HP in the treatment of patients with peptic ulcer disease, in whom ulcers were identified that were not “amenable” to conventional therapy and often recurrent, was recognized. At that time, therapy with H2 receptor antagonists was considered the most effective (recognized) method of treating patients with peptic ulcer disease (there were no effective alternative therapy options for HP eradication). For example, in Japan, a popular question at that time was discussed: what is more effective – inhibition of acid formation in the stomach or eradication of HP? Later, at a Joint Meeting in the USA [12], it was decided that the combined use of antisecretory drugs and antibiotics is necessary in the treatment of patients with peptic ulcer disease, regardless of whether the ulcer was detected for the first time or a relapse of the disease was just detected. Somewhat later in Holland (Maastricht) in 1996, at the first Maastricht consensus, which was held in the form of a meeting of general practitioners from different European countries, representatives of gastroenterological societies, specialists and experts from different countries of the world, criteria for the presence of HP, methods for its identification and possible treatment of patients who have diseases (exacerbation and remission of peptic ulcer disease, chronic atrophic gastritis, functional dyspepsia, gastric MALT lymphoma), in which it is advisable to eradicate HP [14], although sufficiently reliable scientific evidence of the need for eradication of HP is not yet available were obtained [13]. At the same time, it was emphasized that the Maastricht agreements were proposed only for the countries of the European Union (perhaps other options for treating patients are needed in other, economically less developed countries). It was also noted that these agreements are intended only for general practitioners, and if there is insufficient effect in the treatment of patients (primarily with peptic ulcer disease), it is necessary to contact a specialist, i.e., a gastroenterologist. Later, at the second Maastricht consensus in 2000, it was decided to reduce the number of possible anti-Helicobacter therapy regimens and proposed (for European Union countries) in practical work to use (for at least 7 days) only two treatment regimens as first-line therapy patients with peptic ulcer disease (as a base drug - one of the proton pump inhibitors (PPI) or ranitidine bismuth citrate in standard dosages twice a day in combination with two antibiotics (clarithromycin 500 mg + amoxicillin 1000 mg, respectively, twice a day or instead of amoxicillin – metronidazole 500 mg twice a day)). Further development and improvement of ideas for the diagnosis and treatment of acid-related diseases, including those associated with HP, based on the results of studies conducted in Russia, was reflected in the first, second and third Moscow agreements [7-9]. In 2006, publications appeared in the accessible press about the results of the third Maastricht Agreement.
Basic principles of therapy for peptic ulcers Improving the quality of life and eliminating risk factors are some of the important factors in improving the condition of patients and preventing relapses of peptic ulcers. Unfortunately, it is not yet possible to influence the genetic characteristics of people in order to prevent the occurrence of peptic ulcer disease. Therefore, the following should obviously be considered the main principles of drug treatment of patients with peptic ulcer disease [1]:
• impact on factors of aggression and/or defense; • in case of peptic ulcer associated with HP – its eradication; • in necessary cases, the use of medications in the treatment of patients that eliminate dyspeptic and/or “psycho-emotional” symptoms; • correction of drug treatment of patients taking into account concomitant diseases; • taking into account the individual characteristics of patients (age and body weight, tolerance of certain medications by specific patients, their activity, i.e. ability to take care of themselves, etc.); • taking into account the financial capabilities of the hospital and especially specific patients if their treatment is carried out in an outpatient setting.
To carry out standardization, increase the efficiency of diagnosis and treatment of patients, the standards “Diagnostics and therapy of acid-related diseases, including those associated with Helicobacter pylori” were adopted at the V Scientific Society of Gastroenterologists of Russia, combined with the XXXI session of the Central Research Institute of Gastroenterology, in February 2006 [9] . Accepted standards allow doctors to have at their disposal alternative options for diagnosing and treating patients with peptic ulcer disease associated with HP. As our own experience shows, the choice of treatment option for peptic ulcer disease may depend on various factors:
• on the size and location of ulcers, the duration of the disease; • individual resistance of patients to certain drugs; • tolerability of certain drugs by some patients; • the presence or absence of certain drugs in pharmacies of specific hospitals or at the place of residence of patients; • financial capabilities of patients when treating them outside the hospital.
The need to introduce alternative treatment options for patients into practice is also due to the following fact: in practical work (in inpatient or outpatient settings), treatment is often carried out based on available capabilities, which depend on various reasons. According to accepted standards, options for anti-Helicobacter therapy for peptic ulcer disease associated with HP have been identified.
Options for first-line anti-Helicobacter therapy for peptic ulcer disease associated with HP
First option One of PPI (omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole) in a standard dosage and clarithromycin 500 mg in combination with amoxicillin 1000 mg or metronidazole 400-500 mg, respectively. All drugs are prescribed to patients twice a day for at least 7 days (in the absence of ulcer healing - up to 10 days, followed by three-week PPI therapy).
The second option for first-line therapy is Bismuth tripotassium dicitrate (de-nol) 240 mg in combination with amoxicillin 1000 mg and clarithromycin 250 mg, respectively, all drugs are used twice a day for 10 days. If the ulcer does not heal, according to the results of the control endoscopy on days 11-12, continue treatment of patients for another 2.5 weeks with de-nol 240 mg twice a day. If (before treatment) patients have severe pain in the epigastric and/or pyloroduodenal region, it is advisable to add ranitidine or famotidine, respectively, 300 mg or 40 mg at night, to this therapy for the first 10 days. For large ulcers of the stomach and duodenum (1.5-2 cm or more), the above-mentioned anti-Helicobacter therapy (in one option, one of the PPIs is proposed as a basic drug, in the other, tripotassium bismuth dicitrate in combination with two antibiotics) is carried out in for 10 days, followed by therapy with one of the basic drugs for three weeks. After this, it is advisable to conduct the first control EGDS; If the ulcer does not heal, treatment of patients should be continued with the basic drug for another 4 weeks.
Third first-line treatment option One of the PPIs at a standard dose in combination with amoxicillin 1000 mg bismuth tripotassium dicitrate 240 mg respectively twice a day for 10 days. If the ulcer does not heal, according to endoscopy, continue treatment with one of the PPIs or bismuth tripotassium dicitrate for another three weeks.
The fourth option for first-line therapy When treating patients with large ulcers (2 cm or more), as well as with so-called long-term non-healing ulcers and/or penetrating ulcers of the stomach and duodenum (regardless of size) associated with HP (if patients refuse surgical treatment or due to the presence of contraindications), it is advisable to immediately use “quad therapy” (see below) for 10 days, followed by treatment for another three weeks with tripotassium bismuth dicitrate 240 mg twice a day and ranitidine or famotidine (respectively 300 mg or 40 mg at night); if the ulcer does not heal, according to endoscopy, treatment should be continued for another 4 weeks.
Second-line anti-Helicobacter therapy (quadruple therapy) Therapy is carried out in the absence of eradication of HP after treatment with one of the first-line triple therapy options presented above, as well as as first-line therapy in the treatment of patients with “long-term non-healing” ulcers and/or with penetrating ulcers (see. higher). The quadruple therapy regimen is one of the PPIs at a standard dose twice a day, tripotassium bismuth dicitrate 120 mg 4 times a day, metronidazole 400-500 mg three times a day, tetracycline 50 mg 4 times a day for 7 days.
Third-line anti-Helicobacter therapy Therapy is carried out in the absence of HP eradication after second-line therapy according to the following regimen: one of the PPIs in a standard dose, tripotassium bismuth dicitrate 240 mg, furazolidone 200 mg (accordingly, all drugs are taken twice a day for 7 days ). When choosing the above procedure for the use of drug treatment regimens for patients with peptic ulcer disease associated with HP, we proceeded from the following:
• in the majority of patients, triple anti-Helicobacter therapy makes it possible to achieve eradication of HP (hence, reduce the number of drugs, which reduces the likelihood of complications and side effects in a larger number of patients, as well as reduce the financial component of treatment); • furazolidone produces more side effects and complications than metronidazole (the Maastricht Agreements confirmed the effectiveness and feasibility of using metronidazole in HP eradication therapy for peptic ulcer disease).
Conclusion In itself, the prescription of various medications in the treatment of peptic ulcer has two main goals - ensuring the greatest effect and minimizing the likelihood of possible side effects and complications, including during anti-Helicobacter therapy for peptic ulcer associated with HP. The following factors are of particular importance when choosing drug treatment options for patients with peptic ulcer disease:
• tolerance by specific patients to certain medications (not just antibiotics); • presence of concomitant diseases; • individual resistance of specific patients to certain drugs; • availability of drugs in the hospital pharmacy network or in the areas where patients live, if their treatment is carried out in an outpatient setting, as well as their financial condition.
In connection with the above, in some cases it is advisable to use alternative treatment options for peptic ulcer disease. The results of ulcer healing and HP eradication given in the literature, to a certain extent, as is known, depend on the selection of patients, the duration of one or another option of anti-Helicobacter therapy, the regularity of taking prescribed medications, etc. Therefore, it is necessary to pay attention to working with patients sufficient attention. Taking into account the individual characteristics of specific patients, it is advisable to make timely adjustments to their treatment regimens.
Literature 1. Vasiliev Yu.V. Peptic ulcer and Helicobacter pylori // Russian Journal of Gastroenterology, Hepatology and Coloproctology 2001. T. XI. No. 5. P. 19. 2. Vasiliev Yu.V. Pharmacotherapy of peptic ulcer in elderly and senile patients // Materials of the 1st Russian Scientific Forum “Gerontology of the 21st Century”. M., 2001. P. 47-50. 3. Vasiliev Yu.V. Diseases of the digestive system. Histamine H2 receptor blockers. M.: “Double Freig”, 2002. 93 p. 4. Vasiliev Yu.V. Peptic ulcer disease and Helicobacter pylori (questions for discussion) // Provincial medical news. 2002. No. 2. P. 8-9. 5. Vasiliev Yu.V. Peptic ulcer // Selected chapters of clinical gastroenterology / ed. L.B. Lazebnik. M.: Anaharsis, 2005. P. 82-112. 6. Vasiliev Yu.V., Yashina N.V. Etiopathogenesis of peptic ulcer (main aspects) // Current issues of clinical medicine. M., 2001. P. 82-87. 7. Lazebnik L.B., Vasiliev Yu.V., Grigoriev P.Ya. and others. Diagnosis and therapy of acid-dependent diseases, including those associated with Helocobacter pylori infection. Draft Standards Program. First Moscow Agreement, 5 February. 2003 // Experimental and clinical gastroenterology. 2003. No. 3. P. 3-18. 8. Lazebnik L.B., Vasiliev Yu.V. Standards for diagnosis and treatment of acid-related diseases, including those associated with Helicobacter pylori. Program draft. Second Moscow Agreement, February 6. 2004 // Experimental and clinical gastroenterology. 2004. No. 2. P. 5-12. 9. Standards for diagnosis and treatment of acid-related diseases, including those associated with Helicobacter pylori. (Third Moscow Agreement, February 4, 2003) / ed. L.B. Lazebnik and Yu.V. Vasilyeva // Experimental and clinical gastroenterology. 2005. No. 3. P. 1-4. 10. Marshall BJ The Campylobacter pylori story // Scand. J. Gastroenterol. Suppl. 1986. Vol. 146. P. 58-68. 11. McGowan CC, Cover TI, Blaser MJ Helicobacter pylori and gastric acid biological and therapeutic implications // Gastroewnterology. 1996. Vol. 110. P. 926-928. 12. NIH consensus development panel on Helicobacter pylori in peptic disease. Helicobacter pylori in peptic ulcer disease // JAMA. 1994. Vol. 272. P. 65-69. 13. The European Helicobacter pylori Study Group (EHPSG). Current European concepts in the management of Helicobacter pylori infection. The Maastricht consensus report // Gut. 1997. Vol. 41. P. 8-13. 14. Treiber G. Treatment of Helicobacter pylori infection // Praxis. 2000. Vol. 89. P. 958-962. 15. Tytgat GNJ, Axon ATR, Dixon MF et al. Helicobacter pylori: causal agent in peptic ulcer disease, Working Party Reports of the World Con-gresses of Gastroenterology, Melbourne, Australia: Blackwell Scientic Publications, 1990:36-45.
Sequential therapy for eradication of Helicobacter pylori infection
Results of a systematic review and meta-analysis
H. pylori infection is the cause of the development of gastric and duodenal ulcers, gastric MALT lymphomas and gastric cancer. Currently, a large number of eradication therapy regimens have been proposed: standard triple therapy with amoxicillin, clarithromycin and a proton pump inhibitor (PPI); quadruple therapy based on bismuth preparations, sequential and concomitant therapy. One of the global problems at the moment is the growing resistance to clarithromycin and metronidazole. To overcome this problem, sequential therapy has increasingly begun to be used in clinical practice, including the prescription of a PPI and amoxicillin at a dose of 1 g 2 times a day for the first five days and for the next five days - a PPI, clarithromycin 500 mg 2 times a day and a drug from nitromidazoles group at a dose of 500 mg 2 times a day. Recent studies comparing this regimen with triple therapy provide encouraging results and suggest the effectiveness of the new eradication regimen.
Target
To compare sequential eradication therapy with other eradication regimens for H. pylori infection.
Materials and methods
The study included randomized controlled trials (RCTs) identified by searching databases such as Medline (from 1950 to May 2013), Embase (from 1980 to May 2013) and the Cochrane Central Register of Controlled Trials (to May 2013). which compared sequential therapy with other eradication regimens in patients over 18 years of age.
results
Sequential therapy versus 7-day triple therapy. According to the results of 22 RCTs, sequential therapy was more effective (RR=1.21, 95% CI: 1.17-1.25). A total of 2449 patients who received sequential therapy were compared with 2566 who received 7-day triple therapy, with eradication rates of 86.5% (95% CI: 82.9-89.7%) and 71.5 ( 95% CI: 68.4-74.5%) respectively.
One study compared the effectiveness of sequential therapy with triple therapy using a PPI, amoxicillin and metronidazole and a PPI, amoxicillin and clarithromycin; sequential therapy was 15.9% more effective than the first and 24.0% more effective than the second.
Sequential therapy versus 10-day triple therapy. The results of 14 RCTs showed only a small difference in the effectiveness of the sequential eradication regimen (RR=1.11, 95% CI: 1.04-1.19).
In total, the study included 1368 patients who were treated with components of a sequential regimen and 1376 patients in whom eradication was carried out using 10-day triple therapy; the effectiveness was 84.3% and 75.3%, respectively.
Sequential therapy versus 14-day triple therapy. The results of 7 studies suggest that there is no difference in effectiveness when comparing the two above-mentioned regimens (RR=1.00, 95% CI: 0.94-1.06).
The effectiveness of the sequential therapy regimen in 1224 patients was 80.8%, and in the group of patients (n=1227) using 14-day triple therapy - 81.3%.
Sequential therapy versus quadruple therapy based on bismuth preparations. Analysis of the results of 3 RCTs did not show any advantages of one eradication regimen over another (RR=1.01, 95% CI: 0.95-1.06).
The effectiveness of eradication in 546 patients in whom sequential therapy was used was 86.2%, and in 545 patients in whom eradication was carried out with drugs included in quadruple therapy - 84.9%.
Sequential therapy versus quadruple therapy without bismuth. 6 RCTs compared the effectiveness of sequential therapy (n=1039) and quadruple therapy (n=1031) using PPIs, amoxicillin, clarithromycin and metronidazole (the duration of therapy was 10 days in 4 studies, 5 days in 2 studies). Analysis of the results showed that the percentage of eradication when using both regimens was the same (81.3% when using quadruple therapy and 81.7% when using sequential therapy).
Results from studies not included in the meta-analysis
Sequential therapy versus sequential therapy with levofloxacin. Three studies compared the effectiveness of sequential therapy using clarithromycin with sequential therapy in which levofloxacin was used instead of clarithromycin at a dose of 500 to 1000 mg per day.
Among 240 patients who received a regimen using 1000 mg of levofloxacin per day, the eradication rate was 90.0%, and among 240 patients who received classical sequential therapy with clarithromycin, the eradication rate was 78.7%. The incidence of side effects was approximately the same (24.3% and 24.4%, respectively).
When comparing therapy using levofloxacin 500 mg per day (n=241) and the classical sequential eradication regimen (n=240), the effectiveness in the first case was 89.8%, and in the second - 79.5%. The incidence of side effects was 13.8% and 14.3%, respectively. Analysis of the results led to the conclusion that a sequential eradication regimen using levofloxacin is more effective than a sequential eradication regimen using clarithromycin.
Comparison of 10-day and 14-day sequential eradication regimens. Two RCTs compared the duration of sequential therapy: 340 patients received 10 days of sequential therapy and 340 received 14 days of sequential therapy. The effectiveness of the therapy was 87.6% and 89.7%, respectively, which did not prove that increasing the duration of therapy increases its effectiveness.
Conclusion
The results of the meta-analysis show that a sequential eradication regimen for Helicobacter pylori infection is more effective than 7 days of standard triple therapy and shows similar effectiveness when compared with eradication regimens prescribed for more than 10 days and including more than 2 antimicrobial drugs.
Source: Luigi Gatta, Nimish Vakil, Dino Vaira, Carmelo Scarpignato. Global eradication rates for Helicobacter pylori infection: systematic review and meta-analysis of sequential therapy. BMJ 2013; 347 doi: https://dx.doi.org/10.1136/bmj.f4587 (Published 7 August 2013) Cite this as: BMJ 2013;347:f4587.