- home
- Treatment of cancer (oncology)
- Intestinal tumors
- Small bowel cancer
—
—
—
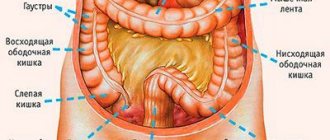
Small intestinal cancer - tumors of the duodenum, small or ileum of a malignant nature (carcinomas and adenocarcinomas, lymphomas, leiomyosarcoma, etc.). Risk factors for their development are chronic gastrointestinal diseases, bad habits, poor diet, radiation exposure, living or working conditions, which a person comes into contact with carcinogens, genetic predisposition.
Approximately half of the cases of oncology of the small intestine occur in tumors of the duodenum, since it is this section that is in direct contact with food containing carcinogens, as well as pancreatic juice and bile.
Classification of small bowel cancer
There are five types of malignant tumors found in the small intestine:
- Adenocarcinoma is, strictly speaking, only cancer. These tumors develop from glandular cells of the mucous membrane, most often found in the jejunum and duodenum.
- Sarcoma is a malignant tumor of connective tissue. The most common tumors are leiomyosarcomas , which are smooth muscle tumors in the intestinal wall. These tumors usually affect the ileum. Gastrointestinal stromal tumors originate from Cajal cells , which are located in the walls of the digestive tract from the esophagus to the anus and provide motility - smooth muscle contractions.
- Carcinoid tumors belong to the group of neuroendocrine tumors . They are most often found in the ileum.
- Lymphomas are tumors of lymphoid tissue. Non-Hodgkin's lymphomas most often occur in the small intestine , usually in the jejunum and ileum.
Causes and risk factors for small intestine cancer
The causes of the disease are unknown: it is impossible to say exactly what exactly led to mutations in the cell and its malignant degeneration in each specific case. The only known factors that increase the risk of the disease are:
- A high-fat, low-fiber diet.
- Crohn's disease , a chronic inflammatory bowel disease, increases the risk of small bowel cancer by about 6 times.
- Celiac disease is a disease in which the villi of the small intestine are damaged and a person cannot tolerate gluten , a protein found in many grains.
- Familial adenomatous polyposis is a hereditary disease in which there are hundreds or thousands of polyps in the large intestine. Over time, these polyps are highly likely to transform into a malignant tumor; in addition, the risk of cancer of the duodenum, stomach, thyroid gland, liver ( hepatoblastoma ), and pancreas increases.
Book a consultation around the clock +7+7+78
When to see a doctor
At the first symptoms of small intestine cancer, which we described above, you should consult a specialist. It is recommended to carry out preventive measures by carrying out regular examinations at a medical center. This will protect you from the hidden development of small intestinal cancer and oncology in other locations.
If you are concerned about the symptoms of small intestinal cancer, then you can make an appointment with an oncologist working in an oncology department. We are located in the central district of Moscow, close to the Mayakovskaya, Belorusskaya, Novoslobodskaya, Tverskaya, Chekhovskaya metro stations.
Symptoms of small intestine cancer
Often the tumor does not cause any symptoms. But even if symptoms are present, they are nonspecific and most often indicate some other disease. You need to visit a doctor and get checked if there is blood in the stool for a long time, or the stool has become dark, black, like tar. Prolonged abdominal pain, diarrhea, unexplained weight loss, severe nausea and vomiting are all possible signs of small bowel cancer. An accurate diagnosis can only be established after examination.
Clinical observation
Patient L., 55 years old, a resident of Moscow, was admitted to the gastroenterology department of MONIKI with complaints of nausea, episodes of vomiting 1-2 times a week with food an hour after meals, bringing relief; moderate aching pain in the epi- and mesogastrium on an empty stomach and an hour after eating; progressive weakness, sweating during physical activity and at night; losing 3-4 kg over the past few months; loosening and increased frequency of stools (3-4 times a day); vesicular rashes on the mucous membrane of the lower lip.
Over the past 8–10 years, she has been experiencing occasional pain in the epigastric region. Esophagogastroduodenoscopy (EGDS) was performed repeatedly; erosive and ulcerative processes of the stomach and duodenum were excluded. Repeated ultrasounds of the abdominal cavity did not reveal any pathology. No blood tests were performed. The deterioration of the patient’s condition was noted 5 months before hospitalization, when epigastric pain resumed and became permanent, nausea and vomiting were bothersome. An endoscopy was performed on an outpatient basis: there was contents in the stomach cavity (food eaten the day before), examination was impossible. The study was not repeated. I took phosphalugel as prescribed by the doctor. During treatment, epigastric pain was relieved, but nausea and episodes of vomiting persisted; noted instability of stool with a tendency to diarrhea. A repeat examination was carried out only after 4 months. With endoscopy - gastric erosion, gastroduodenitis. IDA was detected - hemoglobin 80 g/l, serum iron 2.4 µmol/l; other laboratory examination indicators are not presented. During 7 days of therapy (Nexium 80 mg/day, Motilium 10 mg 3 times a day), pain in the epigastric region decreased and stool returned to normal. To clarify the genesis of IDA, he was hospitalized in the gastroenterology department of MONIKI.
On admission the condition was of moderate severity. The physique is correct, high nutrition, hypersthenic constitution. The skin is pale, normal moisture, clean, there is a vesicle on the mucous membrane of the lower lip (herpes?). Lymph nodes accessible by palpation are not enlarged. The tongue is moist, clean, the papillary layer is smoothed. On palpation, the abdomen is soft and painless. The liver along the right midclavicular line does not protrude from under the edge of the costal arch, the edge of the liver is sharp and painless on palpation. The spleen is not palpable. Stool 1–2 times a day without visible pathological impurities, mushy. There is no peripheral edema. The dynamics of laboratory parameters during hospitalization are presented in the table.
.Dynamics of laboratory parameters.
Coprogram: the reaction to occult blood is positive, erythrocytes - 1-2-3 in the subsurface, single leukocytes in the subsurface, a large amount of mucus.
Analysis of data obtained at the prehospital stage and from the results of the initial examination in the hospital revealed progression of the severity of IDA.
Based on complaints, results of physical and laboratory examinations, the differential range included: gastrointestinal neoplasm (cancer, lymphoma) and erosive-ulcerative process (Crohn's disease, ulcerative colitis), complicated by chronic iron deficiency anemia.
Blood test for tumor markers: CEA; CA 19-9 15.7; CA 15-3; CA 125; PSA general – no deviations from the norm were revealed.
Diagnosis of small intestine cancer
You can examine the duodenum from the inside during fibrogastroduodenoscopy (FGDS) . If the doctor discovers a pathologically changed area on the mucous membrane, he can immediately perform a biopsy and send a piece of tissue for histological and cytological examination.
Special endoscopic techniques are used to examine the jejunum and ileum. During capsule endoscopy, the patient is given a capsule containing a miniature video camera to swallow. It travels through the digestive tract and records an image. With balloon enteroscopy, a tube equipped with one or two balloons is inserted into the small intestine and an endoscope is passed inside it. It can be pulled out of the tube. During balloon enteroscopy, a biopsy can be performed, bleeding can be stopped, and a small tumor can be removed. The end of the small intestine can be examined during a colonoscopy , a test in which a special instrument called a colonoscope is inserted through the anus.
The location of the narrowing in the intestine can be shown by a contrast-enhanced x-ray. Some time before taking x-rays, the patient is given a suspension of barium sulfate to drink. The drug travels through the digestive tract and creates a noticeable shadow in photographs. Sometimes contrast is injected through a probe directly into the duodenum. Barium enemas are used - with the help of such contrast it is sometimes possible to examine the final part of the small intestine.
Computed tomography and MRI are used to assess the location, size and number of tumors, and to identify lesions in the liver, lungs and other organs. To obtain a more informative image, contrast is used: it is administered intravenously or given in tablet form.
PET scanning helps find small metastases that have not been detected by other methods. The patient is injected with radioactively labeled sugar. Since tumor cells need a lot of energy, they absorb this sugar in much greater quantities than healthy tissue. Due to the accumulation of radioactive tracers, tumor foci are clearly visible in images taken using a special apparatus. PET is often combined with CT.
Diagnostics of ZOTK
Early diagnosis of PTD is very difficult. When clinical symptoms appear, already common forms of neoplasms are identified [1, 6]. Palpation of the abdomen reveals infiltration in the abdominal cavity.
Coprological tests for occult blood: Gregersen's test (modified guaiac test) requires dietary restrictions for at least 3 days and has low specificity; immunochemical fecal occult blood tests (FITs) do not require dietary restrictions, but also have relatively low sensitivity and specificity (35–50%); molecular tests for determining DNA containing mutations are highly sensitive (64–91%) and specific (93–96%), but their use is limited by technical difficulties and material costs.
Among the routine instrumental diagnostic methods, the main and most accessible one is X-ray, which includes a survey radiography of the abdominal cavity to exclude intestinal obstruction, a study of the passage of a contrast agent (barium suspension) along the TC in conditions of hypotension, which makes it possible to determine the neoplasm and/or its complications - organ perforation, stenosis. Ultrasound examination (ultrasound) of the abdominal cavity is a mandatory screening method for examining every patient with gastrointestinal pathology; it has high resolution, is simple to perform, does not require complex preparation, and allows not only to diagnose a tumor, but also to identify metastases and perform a diagnostic puncture biopsy.
Both methods require very high qualifications of the researcher and allow diagnosing a tumor only in half of the cases - usually in late stages. Computed tomography and magnetic resonance imaging of the abdominal cavity are used as additional diagnostic methods to clarify the location and extent of the tumor, and detect metastases.
Endoscopic methods should certainly be considered the most promising and informative, but there are technical, organizational and financial difficulties. Endoscopy of the colon, as a rule, is limited to the distal sections (duodenoscopy, jejunoscopy) of the jejunum and distal sections of the ileum (ileocolonoscopy), and is not carried out in all medical institutions. Capsule enteroscopy, unfortunately, is rarely used, primarily due to the high cost of the study. The method is very informative, but has its limitations: it is not indicated for suspected TB stricture and does not allow a biopsy.
The most valuable method today is endoscopic single- or double-balloon intestinoscopy, but it is also expensive, is performed in specialized centers, the number of which is small, and requires anesthesia.
The final diagnosis of PTD is based on the result of a morphological examination of the neoplasm.
Special methods include determining the levels of serotonin, chromogranin in the blood and 5-hydroxyindoleacetic acid in the urine to diagnose carcinoid. If lymphoma is suspected, it is recommended to perform a sternal puncture and trepanobiopsy, and study an immunogram (in blood, saliva, intestinal contents).
The prognosis of PVD is relatively favorable only if it is detected early, if there is no spread of the process to surrounding tissues and distant metastasis, which allows successful surgical removal of the tumor or a full course of chemotherapy (for lymphoma).
Stages of small intestine cancer
There are five stages of intestinal adenocarcinoma:
- Stage 0 : “cancer in situ.” A single small tumor that is located on the surface of the mucous membrane and does not grow deeper.
- Stage I : The tumor has grown deeply into the intestinal wall, but has not spread to neighboring organs.
- Stage II : the tumor has grown through the entire thickness of the intestinal wall and has spread to neighboring organs.
- Stage III : Cancer cells have spread to regional lymph nodes.
- Stage IV : There are distant metastases. Most often they are found in the lungs and liver.
Surgery
Surgeries for small intestine cancer can be radical or palliative . During radical surgery, the surgeon removes the affected area of the intestine, including healthy tissue above and below, and nearby lymph nodes. If the cancer has spread to neighboring organs, they are also removed.
Palliative operations are aimed at improving the patient's condition. If the tumor blocks the intestinal lumen, a bypass anastomosis is performed.
List of sources
- Tsukanov A.S., Shelygin Yu.A., Achkasov S.I., Frolov S.A., Kashnikov V.N., Kuzminov A.M., Pikunov D.Yu., Shubin V.P. Principles of diagnosis and personalized treatment of hereditary forms of colorectal cancer. Bulletin of the Russian Academy of Medical Sciences. — 2019
- Association of Oncologists of Russia. Practical recommendations for drug treatment of patients with colon cancer. — 2014
- V.V. Martynyuk. Colon cancer (morbidity, mortality, risk factors, screening). St. Petersburg Medical Academy of Postgraduate Education. — 2000
Chemotherapy
If adenocarcinoma cancer cells have spread to the lymph nodes, adjuvant chemotherapy is given after surgery to prevent recurrence. In case of adenocarcinoma with metastases, chemotherapy drugs are used for palliative purposes to slow down the progression of the tumor, improve the patient’s condition, and prolong life.
Combinations of chemotherapy drugs are often prescribed for adenocarcinomas:
- FOLFOX: leucovorin + fluorouracil + oxaliplatin.
- FOLFORI : leucovorin + fluorouracil + irinotecan.
If relapse occurs after surgery, fluorouracil may be prescribed in combination with radiation therapy. This therapy is called chemoradiotherapy .
Questions and answers
How to recognize bowel cancer?
The initial symptoms of bowel cancer are similar to a number of other, less dangerous diseases, so patients often do not pay attention to them. If for no apparent reason:
- loss of appetite, aversion to meat dishes;
- stomach ache periodically;
- there is constant discomfort in the abdomen, gas formation has increased;
- prolonged constipation began, alternating with bouts of diarrhea;
this means that you should contact a gastroenterologist or proctologist for examination as soon as possible.
Is there a cure for bowel cancer?
Patients with intestinal tumors can be treated at any stage of cancer. The chances of complete relief from malignant pathology remain even in the most advanced cases.
Colon cancer with metastases: how long do patients live?
Without medical care, the life of a patient with metastases to other organs is 6-11 months, depending on the rate of development of secondary tumors. When completing a course of treatment, the five-year survival rate in patients with metastases is 30-45%, i.e. at least thirty people out of a hundred live more than five years after surgery.
Attention! You can cure this disease for free and receive medical care at JSC "Medicine" (clinic of Academician Roitberg) under the State Guarantees program of Compulsory Medical Insurance (Compulsory Medical Insurance) and High-Tech Medical Care. To find out more, please call +7(495) 775-73-60, or on the VMP page for compulsory medical insurance