1.General information
A bezoar is a concretory formation in the stomach, that is, in fact, an analogue of kidney, gallstones or fecal stones. Some sources indicate that the term comes from the Arabic “bâzahr”, while others consider it to be a translation from the French “bézoard”.
The absolute frequency of occurrence in terms of the general population is not given in the literature and is usually not even approximately estimated. As a rule, only the specific shares of various types (see below) in the total flow of bezoars included in the register, or the share of bezoars (approx. 1%) among the causes of intestinal obstruction, are statistically analyzed. In any case, the formation of bezoar stones is interpreted as a rare or, rather, rarely diagnosed phenomenon. Often without showing any clinical symptoms, bezoars can exist in the stomach for years and are discovered only when there is a tendency to grow, the appearance of discomfort, during an autopsy, or simply by chance (for example, during an examination performed for other indications). Wikipedia reports that by the end of the twentieth century, only about 400 cases of detection of bezoars in humans were described in the world medical literature. However, this information is hardly accurate. According to Perm gastroenterologists, who recently carried out a deep statistical and bibliographic search, domestic doctors alone reported at least 300 cases of bezoar stones in the stomach (since 1912, when such an observation was published for the first time). However, this does not fundamentally change the overall picture: even if the real frequency is hundreds of times higher than the estimated frequency, in relation to the population size it will still remain very small. Another question is that the difficulties of objective diagnosis, as well as the lack of sufficient personal experience among therapists and gastroenterologists in this area (when analyzing a specific case, doctors do not immediately remember that the cause may be a bezoar, and not a tumor, inflammation, etc.) – cause a very large proportion of incorrect diagnoses: according to the results of the above-mentioned statistical analysis, at the first stages of the examination, a bezoar is identified correctly only in every tenth case.
In different historical eras and in different cultures (including modern fantasy art), miraculous and protective properties were attributed to bezoar stones: most often they were considered an antidote or even a panacea. In ruminants and some marine animals, bezoars are much more common than in humans.
A must read! Help with treatment and hospitalization!
Introduction
Bezoars of the gastrointestinal tract (GIT) are a pathology that is extremely rare in the practice of a surgeon. According to their origin, bezoars are divided into phyto-, stibo (sebo)-, trichobezoars, as well as foreign bodies of organic (resin, tar, mineralization of a blood clot in the lumen of the stomach) or embryonic origin [1, 2]. In this case, the most common finding should be considered phytobezoars (up to 70-75% of observations), which, as a rule, are noted in the general population, while trichobezoars, which are a conglomerate of hair and food masses, are a consequence of trichotillomania and are most often recorded in a contingent with emotional lability, as well as sluggish schizophrenia [1, 3-6]. In the case of trichotillomania, trichophagia is detected in 1/3 of patients, and the risk of the formation of conglomerates and the development of complications in the form of obstruction, organ perforation occurs with a frequency not exceeding 0.064% [3]. As a rule, this pathology is more common in females who have an irresistible desire to bite (bite) and swallow their own hair. Gradually, conglomerates of intertwined hair and food masses of varying sizes and density form in the stomach, reaching the consistency of felt [1].
According to summary data, by 1991, about 400 descriptions of trichobezoars of gastric localization were registered in the world press [7], and in Pub Med as of February 2022, a little more than 1300 literary references were identified, with the combination of the terms “gastrictrichobezoar” and “Rapunzelsyndrome” (extreme variant of trichobezoars of the gastrointestinal tract) is registered only in 106 literary sources.
To highlight the problem of foreign bodies in the gastrointestinal tract, to the descriptions of this rarity, if not the casuistic nature of the pathology, let us add an expressive example of a giant trichobezoar of the stomach in a young woman of 24 years old.
Clinical example
Patient S.
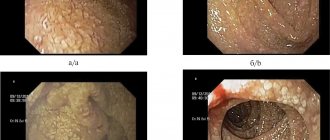
, 24 years old, applied on June 14, 2016 as planned to the surgical clinic of the State Budgetary Healthcare Institution of the City Clinical Hospital named after. V.V. Veresaeva with complaints of heaviness in the epigastric region, dyspepsia, and a feeling of rapid satiety. The above-described complaints are noted by the patient for 3-4 months. Fibrogastroduodenoscopy was performed on an outpatient basis on 05/31/16, and a trichobezoar up to 20 cm in length was detected in the lumen of the stomach, occupying almost the entire lumen of the organ and consisting of hair and food masses (Fig. 1),
Rice.
1. a, b. Endoscopic photo of a trichobezoar in the lumen of the stomach. upon instrumental palpation it showed a loose consistency. A decision was made to inpatient treatment and endoscopic extraction of the foreign body. On objective examination: the patient has satisfactory nutrition and proper physique. Emotionally labile. No hemodynamic or respiratory disorders were noted. The abdomen is of regular shape, soft, painless, pathological mass formations are not palpable. The patient was consulted by a psychiatrist on an outpatient basis at the prehospital stage: no organic pathology was detected, a picture of a hysteroid personality type with pronounced emotional lability. A clinical blood test showed signs of mild hypochromic anemia (blood Hb 107 g/l, RBC 4.12×1012/l, color index 0.78).
Taking into account the findings, the patient was prepared for endoscopic extraction of the foreign body. Esophagogastroduodenoscopy from 06/15/16: almost the entire lumen of the stomach is occupied by a trichobezoar measuring 18.0×5.0×5.5 cm, consisting on the outside of many long hairs with inclusions of food masses. The gastric mucosa is patchily hyperemic. An overtube is installed into the esophagus using a flexible endoscope to protect the oropharynx and esophagus. A two-legged gripper was passed through the working channel of the endoscope to remove foreign bodies. Attempts have been made to fragment the trichobezoar using various instruments and various methods - without achieving results. With a deeper instrumental grasp and palpation of the bezoar with an instrument, its extremely dense consistency is noted at a depth of about 1.0 cm from the surface along its entire length, and therefore, given the size of the formation and the impossibility of its intraluminal endoscopic removal, the study was stopped.
Taking into account the impossibility of endoscopic extraction, the patient was offered surgical removal of the foreign body using video laparoscopic technologies. Laparoscopy of the abdominal cavity from June 16, 2016: the stomach is enlarged throughout its entire length, palpation reveals a dense, displaceable formation, occupying up to 75-80% of the volume of the organ cavity. A gastrotomy up to 5-6 cm long was performed along the greater curvature; a foreign body in the form of an organ cast, consisting of hair and food masses, rocky in depth and loose at the periphery, was identified in the stomach cavity. The foreign body is placed in an endocontainer, the latter is removed from the abdominal cavity through a minilaparotomy (4 cm) incision in the area of the optical trocar. The gastrostomy opening was sutured with a double-row atraumatic intracorporeal suture (Vicryl 2/0), the abdominal cavity was sanitized, and drained in the subhepatic space. Desufflation. Sutures of trocar wounds. The macropreparation is represented by a conglomerate of hair with food masses, rocky density down to a cloth roll in the depths of the conglomerate, with areas of softening on the periphery, measuring 18.0×6.0×6.5 cm (Fig. 2)
Rice. 2. The removed macropreparation is a trichobezoar of the stomach. with the smell of fermentation. The mass of the removed conglomerate is slightly more than 1.5 kg.
The course of the postoperative period is smooth, the patient’s early activation. The drainage was removed on the 2nd day after surgery. She was discharged on the 5th day for outpatient follow-up treatment. The sutures were removed on the 10th day, the trocar wounds and the perprima minilaparotomy approach were healing.
Examination six months later: the patient has satisfactory nutrition, has no complaints, recovery. During endoscopic examination, foreign bodies are not detected in the gastric cavity.
2. Reasons
Despite a certain similarity with stones formed in the urinary tract, biliary ducts, intestines, etc., the etiopathogenesis of gastric bezoars is still different; in addition, to date it has not been sufficiently studied.
If in the first case the main etiopathogenetic role is played by the deposition of salts of various organic acids, then the trigger factor for the formation of bezoars is the ingestion of indigestible substances into the stomach: hair (especially if the patient has an obsessive habit of gnawing or biting hair), casein, synthetic fibers, etc.
There are many such variants known (pyxo-, tricho-, sebobezoars, and many others). Thus, bezoars that had the property of burning were repeatedly extracted from the stomachs of alcoholics who regularly consumed alcohol-containing chemical compounds.
However, three quarters of bezoar stones are of plant origin (phytobezoars). In this regard, it is quite well known that the most dangerous products are those that are dense, fibrous, leathery, with a high content of astringent, sticky, tannin, resinous substances (nuts, dates, figs, wild plums, sunflower seeds, etc.), and the leader Persimmons always appear on this list - most often unripe, or completely ripe, but consumed on an empty stomach and in large quantities.
Such lumps of plant fiber, especially if it is poorly chewed, become the center of compacted formations (usually round in shape and with a smooth surface), which are then often compressed to stone hardness. In general, stone-hard bezoars are more common - sometimes such a stone cannot be broken with a hammer - however, much less dense formations are also known, with a consistency reminiscent, for example, of thick dough.
As a rule, bezoar stones have a foul odor. The dimensions are usually several centimeters, but giant bezoars have also been encountered, representing almost a complete internal cast of the gastric space. In approximately 15% of cases, the stone is formed not in the stomach, but in the small intestine.
Risk factors are disturbances in the evacuation of gastric contents, the vital activity of yeast fungi (for which the bezoar substance serves as a very favorable nutrient medium), hyposecretion of gastric juice, viscous mucus, insufficient primary processing of food in the oral cavity (due to dental problems, constant haste, or simply a bad swallowing habit). large pieces, practically without chewing them), as well as some previous surgical interventions, for example, vagotomy with pyloroplasty.
Visit our Gastroenterology page
Types of gallstones
Types of gallstones that can form in the gallbladder include:
Cholesterol stones in the gall bladder. The most common type of gallstones, called cholesterol gallstones, are often yellow in color. These gallstones are composed primarily of undissolved cholesterol, but may contain other components.
Pigment stones in the gall bladder. These dark brown or black stones form when your bile contains too much bilirubin.
3. Symptoms and diagnosis
The clinical picture depends on a number of factors - the number of bezoars (they can be multiple), their size, location, composition, “age”, mobility - and therefore varies widely. In the first stages, symptoms may be completely absent, and for a very long period. Then, as gastric functions become impaired, nonspecific symptoms appear: nausea, vomiting, loss of appetite, belching, abdominal pain, general weakness, weight loss, sensations of a full stomach or, if large, a “ball” inside, etc.
If the formation of multiple bezoars is recurrent in nature and if they are mobile enough to be evacuated into the duodenum before reaching a significant size (more often the stone remains in the stomach), the patient’s condition can change in waves, but there are also cases when a bezoar becomes the cause of obstruction and obstruction Gastrointestinal tract.
It is necessary to clearly differentiate a bezoar stone from a malignant tumor, gastroenteritis and other types of symptomatically similar pathology. The most informative diagnostic method is FEGDS; sometimes radiography and ultrasound can also help establish the correct diagnosis. Careful examination of all available anamnestic information is essential.
About our clinic Chistye Prudy metro station Medintercom page!
Clinical manifestations of trichotillomania
In TTM, hair pulling can occur in any area of the body, but the most common sites are the scalp (up to 73%), eyebrows and eyelashes (56%), and pubic area (51%). Less common is auto-depilation of the armpits, chest, abdomen and limbs. It is more common to pull out hair one at a time rather than in strands.
Hair pulling, as a rule, occurs daily, taking from several minutes to several hours, often representing a whole ritual - the hair is twisted in a special way around the finger and pulled out. If the hair is short, then it is clamped in a certain way, then extracted, after which it is held between the teeth in order to bite off the bulb and make sure that the hair is completely removed. Many people use devices such as tweezers or scissors for auto-depilation. Hair pulling during TTM is centrifugal - you can always find a “starting point” from which, like waves, foci of auto-depilation with hairs of different lengths diverge in different directions.
There are two types of trichotillomania – automatic and focused. In the automatic version of TTM, autodepilation is carried out without consciousness control, in a “trance-like” or dissociative state. This form of trichotillomania is associated with more severe consequences and is manifested by more dramatic symptoms - extensive and multiple foci of alopecia. The focused type of trichotillomania is accompanied by a purposeful and conscious desire for auto-depilation, while all the subject’s attention is focused on the process of pulling out hair.
The environment is an important factor influencing the frequency and intensity of auto-depilation. A sedentary lifestyle and spending long periods of time in a relaxing, comfortable environment, such as lying in bed before going to bed, have been shown to promote hair pulling.
Over time, the consequences of TTM become obvious to others, causing patients to experience feelings of shame and guilt, which only worsens their condition. It happens that a person denies the problem, tries to rationalize his own behavior, explaining auto-depilation by skin itching, injury, burn or “mere accident”, demonstratively engaged in “searching” for lost hair in the apartment, while showing bewilderment and indignation.
A peculiarity of the course of TTM in women is the connection between the “craving” for auto-depilation and the ovarian-menstrual cycle. According to one study (Ketheun NJ, 1997), in approximately half of the women observed, in the week before menstruation, the “urge to pull out hair” became more frequent and intense, and the ability to resist it significantly decreased.
4.Treatment
As a rule, an attempt is first made to eliminate the problem using conservative methods, for example, a soda solution in combination with a special massage, which in many cases is sufficient for the destruction and subsequent evacuation of the bezoar in parts. If the desired effect is absent, endoscopic destruction or removal is tried. If this does not produce results, they resort to surgical removal; in the presence of severe complications (ulceration, obstruction with a large stone, etc.), the operation is performed urgently, urgently or as an emergency.
The prognosis is usually favorable, especially if the diagnosis is made timely and accurately (for this, first of all, it is necessary to promptly seek help with the complaints described above).
Possible complications
If the bezoar is a large stone moving towards the small intestine, it can cause recurrent intestinal obstruction up to its complete blockage. For this complication, surgical treatment is indicated.
Another complication caused by the formed bezoar may be perforation of the stomach, as well as ulceration of its mucous membranes and bleeding. The same thing can happen with the duodenum.
Classification
Bezoars can be of different origins, that is, have different compositions.
So, what could such a stone consist of:
- trichobezoar - a stone made of hair, wool or fiber (thread);
- phytobezoar - a stone made of cellulose (dietary fiber);
- steobezoar – a stone made from crystallized fats (tard);
- organic bezoar - a stone made from blood clots treated with gastric juice;
- embryonic bezoar - a stone in a newborn child (meconium stones and stones from a cyst formed in the prenatal period);
- mixed stones.
Trichotillomania, obsessive-compulsive disorder and Tourette's syndrome
Until recently, TTM was classified as a disorder of impulse control and impulse control, along with pyromania (an irresistible urge to set fires and watch flames), gambling disorder (pathological urge to gamble) and kleptomania (a morbid urge to commit thefts), which was due to the similarity of manifestations these pathological conditions: an irresistible attraction to a certain action, accompanied by increasing internal tension, and ending with a feeling of relief and relaxation after its completion.
With the release of the new DSM-5 manual in 2013, TTM, along with obsessive-compulsive spectrum disorders (OCD), were classified under the same rubric, which was and is disputed by many experts. Apart from an irresistible compulsion to perform an unwanted action, TTM and OCD have little in common, differing in preferred age of onset, gender ratios, frequency and range of comorbidities, presumed neuroanatomical basis, and treatment effectiveness. And some researchers propose to classify trichotillomania, which began in childhood, as an independent disease (Chamberlain SR et al., 2007).
More and more evidence is emerging about the biological and essential affinity of trichotillomania with tic hyperkinetic disorder, better known as Gilles de la Tourette syndrome. A study conducted by Zuchner S. et al., 2006, demonstrated an increased incidence of SLITKR1 gene mutations in patients suffering not only from TTM, but also from Tourette's syndrome.
Features of trichotillomania in childhood
It is assumed that the development of trichotillomania in children is preceded by physical or psychological trauma: dysfunctional parenting models, rough treatment and attention deficit, forced separation from loved ones, physical and sexual violence, change of place of residence.
In adolescents, in addition to the costs of education, trichotillomania is provoked by a tense environment in the school community and problems in communicating with peers. Although these stressors themselves are not the direct causes of the development of TTM, they are certainly the provoking factors that contribute to the manifestation of the disease. In childhood, the disease usually manifests itself after 3 years. Children carry out auto-depilation uncontrollably, as if automatically: while playing, watching cartoons, and also in situations of stress. The child, unlike adults, does not seek to hide the pathological actions and consequences of TTM.