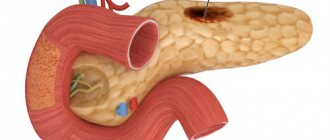
Pseudotumorous pancreatitis is one of the few most dangerous types of pancreatic lesions of the pancreas, having a ICD 10 code - K86.1, with a chronic course. This form of the disease received this name because of its similarity of symptomatic signs with the development of a tumor-like neoplasm in the pancreas. In translation, “pseudo” means false, or imaginary, and “tumor” means a tumor. The pseudotumorous form of chronic pancreatitis is an inflammation of the pancreas, causing the development of partial fibrosis and hypertrophy of pancreatic tissue structures. The peculiarity of the development of this disease is the local enlargement of any part of the pancreas, which is a good reason for differential diagnosis with an oncological neoplasm. In most cases, it is the head of the gland that is affected, so the clinical picture of this form of the disease is often accompanied by obstructive jaundice and subhepatic hypertension.
Causes of pseudotumor pancreatitis
Chronic pseudotumor pancreatitis begins to develop against the background of the following provoking factors:
- untimely and ineffective treatment of chronic pancreatic lesions of the pancreas,
- against the background of gallbladder diseases,
- with excessive consumption of alcohol-containing drinks,
- in some forms of infectious diseases,
- autoimmune pathologies,
- mechanical trauma to the pancreas,
- the development of cystic lesions of the organ, as well as the formation of a tumor.
The main reason for the development of pseudotumorous pancreatitis is the lack of appropriate treatment for pancreatic lesions of the gland, which have a chronic nature of development, as well as deviation from the prescribed diet and the presence of bad habits in the form of drinking alcoholic beverages and smoking. Heredity also plays an important role.
Tumorous pancreatitis mainly includes males who abuse alcohol-containing drinks in its risk group.
The mechanism of occurrence of pathology
The development of a destructive process in the pancreatic cavity begins with the activation of enzymatic components in the form of lipase, trypsin, phospholipase, etc., which contribute to the formation of swelling and self-digestion of the tissue structures of the organ, leading to necrotic damage to certain areas of the gland.
To prevent products from self-digestion of glandular tissue from entering the bloodstream, a protective mechanism begins to activate in the patient’s body, limiting the spread of toxic components, by fencing off the foci of necrosis with connective tissues with the formation of pseudo-cystic formations. With the onset of each exacerbation of pancreatitis, the number of pseudocystic formations increases, which leads to swelling of the pancreas. Over time, the surface of these formations begins to desaltize, and after a decade contribute to the development of compaction in the organ and an increase in its size. This development of the mechanism of the pathological process in the pancreatic cavity, from one point of view, has a protective function and prevents premature death, and from another point of view, contributes to the development of significant hypertrophic processes in the parenchymal organ and further exerting a compressive effect on adjacent organs.
Definition
Pseudotumorous pancreatitis is not a separate nosological (independent) unit, but one of the chronic groups of pancreatitis;
a clinical and morphological form of a chronic inflammatory process in the pancreas, which develops due to untimely initiation of therapy for the underlying disease. This form of the disease received this name because of its similarity of symptomatic signs with the development of a tumor-like neoplasm in the pancreas. In translation, “pseudo” means false, or imaginary, and “tumor” means a tumor. The peculiarity of the development of this disease is the local enlargement of any part of the pancreas, due to hypertrophy of the parenchyma and an increase in the size of the organ, which is a good reason for differential diagnosis with an oncological neoplasm. In most cases, it is the head of the gland that is affected. From the moment of diagnosis of chronic pancreatitis until the development of this form, ten to fifteen years pass. The main factors provoking the development of pseudotumor pancreatitis are long-term abuse of alcoholic beverages and biliary pathology (cholelithiasis and other diseases of the liver and biliary tract) - more than 80% of all cases are caused by these reasons. Less commonly, pseudotumorous pancreatitis occurs as a result of taking certain medications or other somatic diseases. It is believed that pseudotumor pancreatitis of alcoholic etiology develops after an acute process in only 10% of cases, while episodes of exacerbation of pancreatitis are much more often diagnosed against the background of long-term chronic inflammation. It has been proven that the likelihood of chronicity increases significantly in smoking patients.
Biliary-dependent pseudotumor pancreatitis (biliary pancreatitis) in approximately half of cases is a consequence of cholelithiasis; More often, this form of pathology is registered in women; the risk of its development is determined by the duration of the underlying disease and the location of the stones. The etiological factors of biliary-type pancreatitis also include congenital anomalies of the biliary tract, diseases of the papilla of Vater and common bile duct. The pathogenesis of pancreatitis in this case is characterized by the constant reflux of aggressive bile into the pancreatic duct. An important mechanism is also lymphogenous damage to the pancreatic tissue, mainly the head of the pancreas, in which the inflammatory process from the gallbladder spreads through the chain of lymph nodes.
Drug-induced pseudotumor pancreatitis develops with long-term use of acetaminophen, estrogens, and other drugs. Also, chronic pancreatitis with parenchymal hypertrophy may have a hereditary etiology: this form is characterized by systematic progression, increasing endocrine and exocrine organ failure, and a high risk of malignancy.
Typical for chronic pseudotumor pancreatitis:
- Age – younger.
- Gender – men are more often affected.
- Alcohol abuse.
- History of the disease for more than one and a half years.
- Significant loss of body weight (more than 10 kg).
- Abdominal pain syndrome.
- Jaundice in no more than 20% of patients is regressive in nature, with a moderate increase in bilirubin.
- Ultrasound and CT show a decrease in the echogenicity of the head of the gland in approximately 18% of cases.
Characteristic for cancer of the head of the pancreas:
- More mature age, on average, 59 years.
- Both men and women are affected equally.
- Moderate weight loss up to 5-6 kg.
- Progressive jaundice with high bilirubin levels in 90% of patients.
- Ultrasound and CT show a decrease in the echogenicity of the head of the gland in approximately 75% of cases.
Symptoms and signs of the disease
The development of the pseudotumor form of pancreatic lesions of the pancreas is accompanied by the appearance of the following symptomatic signs:
- the occurrence of pain that has a pronounced course,
- a sharp decrease in body weight over a short period of time,
- determination of uneven enlargement of the pancreas at the time of palpation examination of the abdominal cavity,
- pathological change in the exocrine functionality of the organ,
- dyspeptic system disorders,
- vomiting and nausea,
- paleness of the skin with the acquisition of a jaundiced tint,
- enlargement of the head of the gland.
Patients also experience a regular feeling of weakness, immediate fatigue and the development of insomnia, which causes the development of a disorder in their psycho-emotional state.
How is the procedure done?
To accurately identify the condition of the pancreas, specialists resort to MRI with contrast. A contrast agent is injected into the patient's vein. It is necessary for coloring organ tissues in a certain color, depending on their condition and density. This leads to a clearer, more contrasty image and allows you to more accurately determine the condition of the gland. Next, the patient lies down on a mobile table and assumes a stationary position. The table is rolled into a tomograph machine and a scan is performed. An MRI can take up to an hour.
Diagnostic methods
Diagnosis of this form of pathology consists of a step-by-step examination of the patient:
- stool, blood and urine tests are prescribed for a general clinical examination,
- performing ultrasound,
- blood for biochemistry,
- radiography,
- MRI and CT,
- endoscopic examination of the pancreatic ducts,
- histological examination for differential diagnosis with the development of a cancerous tumor in the area of the head of the gland.
Laboratory diagnostic results
Laboratory testing reveals the following in the blood:
Treatment of pseudotumorous pancreatitis
In most cases, therapeutic treatment of pseudotumor pancreatitis has a positive prognosis, subject to an integrated approach to its elimination, which consists of the following:
- drug therapy,
- diet therapy,
- conservative treatment methods,
- endoscopy,
- operation,
- folk treatment.
Conservative treatment
This type of treatment is not as effective in the development of this disease. The use of analgesic drugs, fasting during an exacerbation of the pathology, and the use of drugs that ensure the normalization of the secretory functionality of the gland do not give the necessary effect and do not contribute to transferring the disease to the stage of stable remission.
Although, carrying out these measures is necessary in order to calm the pancreas a little for a more favorable surgical intervention.
Surgical intervention
During the operation, the overgrown tissue structures of the pancreas are excised, which helps relieve compression from the Wirsung and bile ducts. The excised tissue of the affected organ is immediately examined for histology. In the case when a histological examination shows the presence of cancer cells, then, without interrupting the operation, the patient undergoes pancreaticoduodenal excision of the affected tissue.
If, during histological examination, the presence of cancer cells was not detected, then the patient undergoes resection of the head of the gland and enucleation of the largest cystic formations, which exert a compressive effect on the pancreatic ducts.
After such an operation, the disease almost immediately goes into a stage of stable remission.
Folk remedies
Recipes from traditional healers are also widely used to treat the pancreas. Such remedies as infusions and decoctions of medicinal herbs, as well as tinctures and oatmeal jelly, which help not only normalize the gland, but also cleanse the entire body of harmful wastes and toxins, will help restore the functionality of the affected organ and support it during periods of remission.
Description example
1. Descriptive part: The pancreas is enlarged in size due to the head: sagittal size... cm, coronal size... cm, vertical size... cm; in other parts of the gland it is not enlarged, with transverse dimensions: body ... cm, tail ... cm, has clear uneven contours, a homogeneous structure, with native examination without pathological focal changes, with a mildly expressed stromal component. The pancreatic duct in the projection of the head is moderately expanded to .. cm, in the projection of the body and tail it is not expanded.
Conclusion: The MR picture is more consistent with pseudotumorous chronic pancreatitis with an increase in the size of the head of the pancreas.
2. Descriptive part: The pancreas has transverse dimensions: head .. cm, body ... cm, tail ... cm. In the projection of the head of the pancreas, an additional formation is visualized, dimensions ... x ... x ... cm, slightly hyperintense in T2, slightly hypointense in T1, heterogeneous in a consequence of a more intense increase in the MR signal in the central parts of T2, and a decrease in the MR signal in T1. The contours are clear, uneven. In the remaining parts of the head, the intact part of the pancreas is visualized. In the projection of the body and tail, pronounced atrophic changes are noted. The parenchyma is presented in the form of separate thin elements. The Wirsung duct is significantly dilated (up to 0.9 cm).
Conclusion: MRI picture of an additional space-occupying formation in the projection of the head of the pancreas /to differentiate the neoplastic process /tumor/ and pseudotumorous pancreatitis/, morphological verification is recommended to clarify the process.
Diet and prevention
To carry out diet therapy, a dietary diet is prescribed with table No. 5, which provides for the exclusion of the following foods:
- strong tea and coffee drinks, as well as alcohol,
- bakery and confectionery delights,
- fatty foods
- cabbage and legumes,
- fruit crops with a pronounced sour taste.
Allowed to use:
- thermally processed vegetable and fruit crops,
- non-fatty varieties of boiled meat and fish,
- puree soups,
- non-fat dairy products,
- pasta and cereals,
- compote, fruit drink, herbal tea drinks.
Dietary nutrition should become a major change in the patient’s entire lifestyle, which must be adhered to throughout the subsequent period of life. This is the only way to count on stable remission of the pathology.
Complete cessation of bad habits such as drinking alcohol and smoking will be a reliable preventive measure against the development of relapse and exacerbation of the disease.
Prognosis for cure and complications of the disease
Therapeutic treatment of pathology generally has a favorable prognosis, but despite this, the process of eliminating pathology itself must be approached with full responsibility and follow all doctor’s instructions. Otherwise, further development of the medical history may provoke the following types of complications:
- jaundice,
- peritonitis,
- vein thrombosis,
- increased intensity of cystic lesions,
- internal hemorrhage,
- malignancy.
Also, an advanced form of pseudotumor pancreatitis can cause the development of diabetes mellitus.
Bibliography
- Panov S.V., Diseases of the pancreas. Pancreatitis. M.: AST, 2011
- Bozhenkov, Yu. G. Practical pancreatology. Guide for doctors M. Med. book N. Novgorod Publishing House NGMA, 2003
- V.A. Kubyshkin, G.G., Karmazanovsky, S.A. Grishankov. Cystic tumors of the pancreas: diagnosis and treatment. M., Vidar-M, 2013
- Minushkin O.N. Maslovsky L.V. Evsikov A.E. Evaluation of the effectiveness and safety of the use of micronized multienzyme drugs in patients with chronic pancreatitis and exocrine pancreatic insufficiency of breast cancer, section “Gastroenterology” No. 17 2022, pp. 1225-1231.
- Bunin V.A. Objectification of the choice of minimally invasive drainage interventions in patients with obstructive jaundice of tumor origin. Abstract of the dissertation. Surgery. VMedA named after. CM. Kirova, St. Petersburg, 2011
Chronic pancreatitis: from pathogenesis to therapy
Throughout the world, over the past 30 years, there has been an increase in the incidence of acute and chronic pancreatitis by more than 2 times [2]. In Russia, a more intensive increase in the incidence of CP has been observed. Thus, the prevalence of pancreatic diseases among adults over the past 10 years has increased 3 times, and among adolescents - more than 4 times. It is believed that this trend is associated with an increase in alcohol consumption, including low-quality alcohol, a decrease in the quality of nutrition and the general standard of living [3]. Typically, CP develops at the age of 35–50 years; the proportion of women among those affected has increased by 30%. Morbidity rates are constantly growing due to improved diagnostic methods and the recent emergence of new high-resolution imaging methods of the pancreas, which make it possible to detect CP at earlier stages of disease development [4]. Chronic pancreatitis (CP) is a slowly progressive inflammatory disease of the pancreas, characterized by focal necrosis in combination with fibrosis and leading to a progressive decrease in the exo- and endocrine function of the organ (even after the cessation of exposure to the etiological factor). Conventionally, we speak of CP when the inflammatory process in the pancreas continues for more than 6 months. CP usually occurs with episodes of exacerbations and remissions. Acute and chronic pancreatitis. A practicing physician knows how important it is to distinguish between acute and chronic pancreatitis, since there are fundamental differences in the management of such patients. This is sometimes extremely difficult to do, since exacerbation of chronic pancreatitis in its clinical picture is very similar to AP, and AP, in turn, can remain unrecognized (in 60% of cases!), occurring under the masks of other gastrointestinal diseases. In the diagnosis of AP, the most important marker is an increase in serum amylase levels by more than 4 times. It is known that acute pancreatitis transforms into chronic in 10% of cases (and taking into account unrecognized episodes of AP - much more often). Classification of CP I. According to the Marseille-Roman classification (1988), adopted in European countries, the following clinical forms of CP are distinguished: • obstructive, • calcifying, • inflammatory (parenchymal). Chronic obstructive pancreatitis develops as a result of obstruction of the main duct of the pancreas. The damage to the pancreas is uniform and is not accompanied by the formation of stones inside the ducts. In the clinical picture of this form of CP, the leading one is constant pain. With calcifying CP, protein precipitates or calcifications, stones, cysts and pseudocysts, stenosis and atresia, as well as atrophy of acinar tissue are found in the ducts. This form of CP is characterized by a relapsing course with episodes of exacerbation, in the early stages resembling acute pancreatitis (chronic recurrent pancreatitis). As a rule, such CP has an alcoholic etiology. Chronic parenchymal pancreatitis is characterized by the development of foci of inflammation in the parenchyma with a predominance of mononuclear cells and areas of fibrosis in the infiltrates, which replace the pancreatic parenchyma. With this form of CP there is no damage to the ducts and calcifications in the pancreas. In the clinical picture, the leading ones are slowly progressive signs of exocrine and endocrine insufficiency and the absence of pain syndrome (CP, painless form). II. The classification of CP proposed by V.T. is generally accepted in Russia. Ivashkin et al. [8]. CP is divided according to several characteristics: 1. According to morphological characteristics: 1) interstitial-edematous; 2) parenchymal; 3) fibrous-sclerotic (indurative); 4) hyperplastic (pseudotumorous); 5) cystic. 2. According to clinical manifestations: 1) pain; 2) hyposecretory; 3) asthenoneurotic (hypochondriacal); 4) latent; 5) combined. 3. According to the nature of the clinical course: 1) rarely relapsing; 2) often recurrent; 3) persistent. 4. By etiology: 1) alcoholic; 2) biliary dependent; 3) dismetabolic; 4) infectious; 5) medicinal; 6) idiopathic. 5. Complications: 1) disturbances in the outflow of bile; 2) portal hypertension; 3) infectious (cholangitis, abscesses); 4) inflammatory (abscess, cyst, parapancreatitis, “enzymatic cholecystitis”, erosive esophagitis); 5) gastro-duodenal bleeding; 6) effusion pleurisy, pneumonia, acute respiratory distress syndrome, paranephritis, acute renal failure; 7) exocrine disorders (diabetes mellitus, hypoglycemic conditions). Etiology of CP The main reasons for the development of CP are the following: 1) alcohol consumption - alcoholic pancreatitis (more often in men) in a dose of more than 20-80 mg of ethanol/day. for 8–12 years (according to various sources) – 40–80% [5] and tobacco smoking; 2) diseases of the gallbladder and duodenum - biliary pancreatitis (more often in women); • cholelithiasis is the cause of CP in 35–56%; • pathology of the sphincter of Oddi (stenosis, strictures, inflammation, tumor); • duodenitis and peptic ulcer 12 PCs. Thus, peptic ulcer of the 12th PC in 10.5–16.5% of cases is the direct cause of the development of CP [6]. 3) cystic fibrosis (often in children); 4) hereditary pancreatitis. It is most common in Northern Europe, its incidence is about 5% of all cases of CP. The absence of etiological factors and cases of pancreatitis in the family of the patient’s relatives allow one to suspect a hereditary form of pancreatitis; 5) idiopathic pancreatitis. When at the time of the study identification of the etiological factor is impossible - 10 to 30% of all pancreatitis; 6) other causes: • autoimmune pancreatitis • systemic diseases and vasculitis • viral (Coxsackie, CMV) and bacterial infections • helminthic infestations (opisthorchiasis) • metabolic disorders (hyperlipidemia, diabetes mellitus, chronic renal failure, etc.) • circulatory disorders (ischemic pancreatitis) • anomalies of pancreas development • injuries, acute poisoning. Pathogenesis of CP The pathogenesis of CP, regardless of the cause, is based on the premature activation of its own enzymes, which leads to autolysis (“self-digestion”) of the pancreas. The main factor is the conversion of trypsinogen into trypsin directly in the ducts and in the tissue of the pancreas (normally this occurs in 12 PCs), which is an extremely aggressive factor that damages the pancreas, resulting in an inflammatory reaction. The mechanisms underlying premature enzyme activation will vary depending on the underlying etiological factor. Effect of alcohol on the pancreas Several mechanisms are involved in the pathogenesis of alcoholic pancreatitis [7]: 1. Ethanol causes spasm of the sphincter of Oddi, which leads to the development of intraductal hypertension and the walls of the ducts become permeable to enzymes. The latter are activated, “triggering” the autolysis of pancreatic tissue. 2. Under the influence of alcohol, the qualitative composition of pancreatic juice changes, which contains an excess amount of protein and a low concentration of bicarbonates. In this regard, conditions are created for the loss of protein precipitates in the form of plugs, which then calcify and obstruct the pancreatic ducts (calcific pancreatitis). 3. Ethanol disrupts the synthesis of phospholipids in cell membranes, causing an increase in their permeability to enzymes. 4. Direct toxic effect of ethanol and its metabolites on pancreatic cells, a decrease in the activity of the oxidase enzyme, which leads to the formation of free radicals responsible for the development of necrosis and inflammation with subsequent fibrosis and fatty degeneration of pancreatic tissue. 5. Ethanol promotes fibrosis of small vessels with impaired microcirculation. Mechanisms of development of biliary pancreatitis 1. The anatomical proximity of the places where the common bile and pancreatic ducts flow into the duodenum, for various reasons, can lead to bile reflux, as a result of which trypsinogen is activated. 2. Due to obstruction of the duct or ampulla of the duodenal papilla, hypertension develops in the pancreatic duct with subsequent rupture of the small pancreatic ducts. This leads to the release of secretions into the parenchyma of the gland and the activation of digestive enzymes. Frequent relapses of biliary pancreatitis usually occur with the migration of small and very small stones (microlites), the most dangerous are stones up to 4 mm in size. 3. A fairly common cause leading to the development of CP is duodenopancreatic reflux, which occurs against the background of atony of the sphincter of Oddi, especially in the presence of duodenal hypertension. 4. Pathogenetic factors for the development of CP in peptic ulcer disease are: • swelling of the papilla of Vater (papillitis) with secondary obstruction of the outflow of pancreatic secretions; • hyperacidity of gastric juice with excessive stimulation of the pancreas with hydrochloric acid, in conditions of obstructed outflow this leads to intraductal hypertension. 5. Often in the development of biliary CP there is a combination of etiological mechanisms; for example, in patients with cholelithiasis, tumors of the obstructive system, peptic ulcer disease, etc. are detected. Other mechanisms Ischemia. Ischemic pancreatitis occurs quite often in the elderly and senile age. There are several main causes of pancreatic ischemia: • compression of the celiac trunk by enlarged retroperitoneal lymph nodes, pancreatic cysts; • pressure of the feeding vessels of the enlarged pancreas in pseudotumor pancreatitis. • atherosclerotic lesion of the celiac trunk; • thromboembolism; • diabetic angiopathy. Hyperlipidemia. A high risk of pancreatitis occurs when triglycerides rise above 500 mg/dL. The mechanism of development of CP is associated with the toxic effect on pancreatic tissue of high concentrations of free fatty acids, which cannot be completely bound by serum albumin in the blood plasma. Clinical manifestations of CP The most common clinical syndromes in CP are: • abdominal pain syndrome, • pancreatic exocrine insufficiency syndrome, • endocrine disorder syndrome, • dyspeptic syndrome, • biliary hypertension syndrome. 1. Pain syndrome Pain can occur both during exacerbation and in the remission phase of CP. It does not have a clear localization, occurring in the upper or middle abdomen on the left or in the middle, radiating to the back, sometimes taking on a encircling character. More than half of the patients have extremely intense pain. The following mechanisms for the development of pain in CP can be distinguished: 1) acute inflammation of the pancreas (damage to the parenchyma and capsule); 2) pseudocysts with perifocal inflammation; 3) obstruction and dilatation of the pancreatic and bile ducts; 4) fibrosis in the area of sensory nerves, leading to their compression; 5) pressure on the surrounding nerve plexuses of the enlarged pancreas; 6) stenosis and dyskinesia of the sphincter of Oddi. a) Pain associated with pseudocysts and ductal obstruction is significantly worse during or immediately after eating. The pain is usually girdling and paroxysmal. Antisecretory drugs and pancreatin preparations (Panzinorm), which reduce pancreatic secretion through a feedback mechanism, significantly reduce pain. b) Inflammatory pain does not depend on food intake, is localized, as a rule, in the epigastrium, and radiates to the back. Such pain is relieved with analgesics (NSAIDs, in severe cases - narcotic analgesics) c) Exocrine pancreatic insufficiency leads to excessive bacterial growth in the small intestine, which is also the cause of pain in a significant proportion of patients with CP. These pains are caused by increased pressure in the duodenum. In the later stages of CP, with the development of fibrosis, pain decreases and may disappear after a few years. Then the manifestations of exocrine insufficiency come to the fore. 2. Exocrine insufficiency syndrome Exocrine pancreatic insufficiency is manifested by a violation of the processes of intestinal digestion and absorption. Clinically, it is manifested by: • diarrhea (stool 3 to 6 times a day), • steatorrhea (occurs when pancreatic secretion decreases by 10%, stool is mushy, fetid, with a greasy sheen). • weight loss, • nausea, • occasional vomiting, • loss of appetite. The syndrome of bacterial overgrowth in the small intestine develops quite quickly, manifested by: • flatulence, • rumbling in the abdomen, • belching. Later, symptoms characteristic of hypovitaminosis appear. Exocrine pancreatic insufficiency is based on the following mechanisms: 1) destruction of acinar cells, resulting in decreased synthesis of pancreatic enzymes; 2) obstruction of the pancreatic duct, interfering with the flow of pancreatic juice into the duodenum; 3) a decrease in the secretion of bicarbonates by the epithelium of the pancreatic ducts leads to acidification of the contents of the duodenum to pH 4 and below, resulting in denaturation of pancreatic enzymes and precipitation of bile acids. 3. Biliary hypertension syndrome Biliary hypertension syndrome is manifested by obstructive jaundice and cholangitis and is not rare. Up to 30% of patients in the acute stage of CP have transient or persistent hyperbilirubinemia. The causes of the syndrome are enlargement of the head of the pancreas with compression of the terminal part of the common bile duct, choledocholithiasis and pathology of the obstructive system (calculi, stenosis). 4. Endocrine disruption syndrome Is detected in approximately 1/3 of patients. The development of these disorders is based on damage to all cells of the islet apparatus of the pancreas, resulting in a deficiency of not only insulin, but also glucagon. This explains the features of the course of pancreatogenic diabetes mellitus: a tendency to hypoglycemia, the need for low doses of insulin, the rare development of ketoacidosis, vascular and other complications. 5. Symptoms caused by fermentemia • Intoxication syndrome is manifested by general weakness, loss of appetite, hypotension, tachycardia, fever, leukocytosis and increased ESR. • Tuzhilin's symptom (symptom of “red droplets”): the appearance of bright red spots on the skin of the chest, back, and abdomen. These spots represent vascular aneurysms and do not disappear with pressure. Diagnosis of CP I. Objective examination data II. Instrumental diagnostic methods 1. Ultrasound diagnosis of chronic pancreatitis. • Transabdominal ultrasound allows you to determine changes in the size of the pancreas, uneven contour, decrease and increase in its echogenicity, pseudocysts, calcifications, etc. • Endoscopic ultrasonography (EUS) is a diagnostic method in which the examination is carried out not through the abdominal wall, but through the wall of the stomach and duodenum. This allows you to study in detail the structure of pancreatic tissue, the state of the ductal system, identify stones, and carry out a differential diagnosis of pancreatitis with pancreatic cancer. 2. Computed tomography is a highly informative method, especially in conditions of poor visualization of the pancreas with ultrasound. 3. ERCP allows to identify pathology of the common bile and main pancreatic duct, determine the localization of obstruction, and detect intraductal calcifications. 4. Magnetic resonance imaging - the latest MRI programs that allow you to obtain a direct image of the pancreatic ducts (as with ERCP) without invasive intervention and the introduction of contrast agents. 5. A survey X-ray of the abdomen allows us to detect the presence of calcifications in the projection area of the pancreas, which are detected in 30% of patients with CP. III. Laboratory diagnosis of chronic pancreatitis 1. Clinical blood test (with exacerbation of CP, leukocytosis, acceleration of ESR may occur, with the development of protein-energy deficiency - anemia). 2. Study of the content (activity) of pancreatic enzymes: • amylase in the blood and urine. During the period of remission, CP may be normal; during exacerbation, it increases moderately (by 30%); when serum amylase increases above 4 norms, one should think about AP. Urine amylase is a less sensitive marker of AP than blood amylase; • elastase 1 in blood and feces is a highly sensitive marker. The activity of this enzyme in the blood increases with pancreatitis earlier than the level of other enzymes and lasts longer. The enzyme-linked immunosorbent method for determining elastase 1 in feces is currently the “gold standard” - the most informative non-invasive method for diagnosing exocrine pancreatic insufficiency. This enzyme is absolutely specific for the pancreas, is not destroyed when passing through the gastrointestinal tract and, importantly, the test results are not affected by pharmacological replacement therapy. Exocrine insufficiency is diagnosed when elastase 1 decreases below 200 μg/g of feces. 3. Other pancreatic enzymes. Highly sensitive and specific tests indicating an exacerbation of the disease are an increase in the activity of serum lipase, as well as serum trypsin and a decrease in the concentration of trypsin inhibitor. However, with severe pancreatic fibrosis, the level of enzymes in the blood serum, even during exacerbation of the disease, may be normal or low. 4. Assessment of the exocrine function of the pancreas: 1) standard coprological examination. The criteria for exocrine insufficiency are an increased content of neutral fat and soap in the feces with a slightly changed content of fatty acids. An increased number of muscle fibers in the feces (creatorrhea) is a later sign of pancreatic failure than steatorrhea and indicates a more severe degree of impairment; 2) the quantitative determination of fat in the feces is a time -consuming, but rather informative test (a normal amount of fat in feces less than 5 g/day). • probes methods - 1) Secretine - pancreosimine (secretin - cholecystokinin) test, 2) indirect probe method (Test Lund). The tests are informative, but laborious, expensive and can have complications. Currently, rarely used. • Bisanding diagnostic methods are simpler, cheaper and carry a minimum risk of complications. However, they have less sensitivity and specificity than probe methods. All of them are based on the oral introduction of specific substrates for pancreatic enzymes. After the interaction of the latter with the enzymes of the pancreas in the urine and/or in the blood serum, the products of splitting are determined, by the number of which they judge the degree of executionary failure. 1) Bentiramidal test (NBT - Paba Test). NBT - a tripeptide specific for chipripsin, breaks down to a ram, which is determined in the urine; 2) iodolipol test: lipase breaks the iodolip to iodide, which are determined in the urine; 3) Fluorescein - a divine test 5. Assessment of the increting function of the pancreas. Disorders of carbohydrate metabolism in CP are detected in approximately 1/3 of patients. All patients with CP are recommended to conduct a glucosotolerant test to detect NTG and diabetes. Treatment of CP because the leading pathogenetic mechanism in CP is the activation of its own enzymes, the main target of pathogenetic therapy will be precisely the executive function of the pancreas. What is important, we must achieve a decrease in our own secretion of the pancreas not only with exacerbation, but also in remission of HP. This is necessary for the treatment of pancreatic pain, and to reduce the degree of inflammation in the pancreas. The main stimulants of the secretion of pancreas are hydrochloric acid, bile acids, fats, especially animal origin, alcohol. It is important to maximize the influence of these factors on the pancreas. Dietotherapy alcohol is excluded at all stages of CP, regardless of the cause of its development. Also exclude salted, fried and fatty foods. With exacerbation of CP in the first 2 days, hunger is recommended. Only fluid is allowed in an amount of 1.0-1.5 liters per day (5-6 times 200 ml). Assign alkaline mineral water without gas, rosehip decoction, weak tea. As the condition improves (usually on the 2-3rd day from the start of exacerbation), you can slowly expand the diet. At the same time, it is important to observe the basic principles of diet therapy of patients with CP - the diet should be mechanically and chemically sparing, low -calorie and containing the physiological norm of protein (with the inclusion of 30% of animal protein). Since liquid food and carbohydrates to the smallest degree stimulate pancreatic and gastric secretion, oral nutrition begins with mucous soups, liquid wiped milk cereals, vegetable puree and jelly. With light exacerbations, oatmeal or rice porridge on water, pasta, and low -powered protein foods are prescribed. Pharmacotherapy Principles for the treatment of pancreatic pain 1. Diet and exclusion of alcohol! 2. Analgesics. To quickly stop the pain, a phased analgesic therapy is prescribed [9], including antispasmoanalgesics. In the absence of the effect, antipsychotics (dropperol 2.5–5 mg + fentanin 0.05–0.1 mg ° V) are prescribed for 3-4 hours. Often additionally used in the drip administration of lidocaine of 400 mg/day. (4 ml of a 10% solution in 100 ml of isotonic solution of sodium chloride or glucose). With a pronounced pain syndrome that cannot be treated, narcotic drugs (Promedol) are prescribed. 3. Pancreatic enzymes. To relieve pancreatic pain, a high content of lipase and trypsin is necessary. Important is the exclusion of bile acids in the enzyme preparation. Such requirements are satisfied with the panzinorm Fort 20,000. The drug contains pancreatin with enzymatic activity in each pork tablet: 20,000 Lipases 20,000 PH.Eur., Amylase 12,000 PH. EUR., Proteases 900 PH. Eur. The drug is available in the form of tablets coated with a film shell. The pancreatic enzymes (lipase, a -amilasis, tripsin, chiriperipsin) contribute to the breakdown of proteins to amino acids, fats to glycerol and fatty acids, starch - to dextrins and monosaccharides, thus reducing the stimulating effect of food on the secretion of the pancreas. Tripsin also suppresses the stimulated secretion of the pancreas, having an analgesic effect. Pancreatic enzymes are released from the dosage form in the alkaline medium of the small intestine, because Protected by the action of gastric juice with a shell, which also increases the effectiveness of this drug. The maximum enzymatic activity of the drug is observed after 30–45 minutes. after reception. The correct regime of taking the drug is very important. So, in order to stop the pain syndrome, a panzinorm Forte 20,000 must be prescribed during fasting 1 tablet every 3 hours or 2 tablets every 6 hours (1-3 days), and after eating a meal, 1 tablet in 20-30 minutes. before meals. And for replacement therapy of external spray insufficiency, a panzinorm Fort 20,000 is prescribed 1-2 tablet with food. 4. Somatostatin and octreotide are prescribed mainly with severe exacerbations of CP and for OP. 5. Antisecretory drugs. In order to reduce the secretion of the pancreas, proton pump inhibitors (omeprazole), or H2 -blockers (Ranitidine), aluminum containing antacids (rutacid), binding bile acids are prescribed. Polyerferment therapy replacement for compensation for the extension of the pancreas, as a rule, is used to use highly active enzyme preparations containing large doses of enzymes (at least 10,000 Lipase units). Replacing therapy is necessary for diseases accompanied by atrophy of more than 90% of the organ parenchyma [10]. The dose of enzymes depends on the degree of external spray deficiency, as well as on the patient's ability to observe a diet. In case of external spraying pancreatic failure, a single dose of enzymes is from 10,000 to 20,000, and sometimes up to 30,000 units. lipases. The effectiveness of therapy is evaluated clinically and laboratory (coprological study, excretion of fat with feces, elastasic test). Panzinorm 10,000 is proven in relation to the correction of the excretory function of the pancreas. The drug is produced in the form of a capsule, each contains pancreatin in the form of pellets, with the activity of lipase 10,000 PH. EUR, amylase at least 7200 PH. Eur., Proteases of at least 400 PH. Eur. The drug has high enzyme activity. Panzinorma 10,000 take 1-2 capsules during meals 3 times/day. With a properly selected dose of enzymes in patients, weight stabilizes or increases, diarrhea, flatulence, abdominal pain ceases, steator and creator disappears. Panzinorma 10,000 with CP with external spray deficiency is prescribed for life. Doses can be reduced subject to a strict diet with limitation of fat and protein and increase when expanding it. Infusion and detoxification therapy for severe exacerbations during the first days of exacerbation is indicated in/in the introduction of a liquid of 3 or more l/day: reopoliglyukin (400 ml/day), hemodez (300 ml/day), 10% Albumin solution (100 ml/day), a 5-10% solution of glucose (500 ml/day), which, along with a decrease in pain and intoxication, prevents the development of hypovolemic shock. Literature 1. Korotko G.F. Pancreatic secretion regulation // Ross. magazine Gastroenterol., Hepatol. And Koloproctol. - 1999. - No. 4. - S. 6–15. 2. Maev I.V., Kazyulin A.N., Kucheryovy Yu.A. and others. Some issues of epidemiology of chronic pancreatitis // Clinical -epidemiological and ethno -ethnic problems of digestive diseases: Materials of the Third East Siberian Gastroenterological Conference / Ed. prof. V.V. Tsukanova. - Krasnoyarsk, 2003. - S. 9–52. 3. Tuchina L.M., Poroshenko G.G. The prevalence of pancreatic diseases among the population of Moscow // Ross. gastroenterol. Journal - 2001 - No. 2 - P. 154. 4. Minko A.B., Pruchansky V.S., Korytova L.I. Complex radiation diagnosis of pancreatic diseases. - St. Petersburg: Hippocrates. - 2001.– 134 p. 5. Bagnenko S.F., Kurygin A.A., Rukhlyada N.V., Smirnov A.D. Chronic pancreatitis: Guide for doctors. - St. Petersburg: Peter, 2000. - 416 p. 6. Kokueva O.V., Tsymbalyuk Yu.M., Novosel N.V. Features of the ultrasonic picture in chronic pancreatitis in combination with duodenal ulcer // wedge, honey. 2001. No. 7. S. 57–60. 7. I.V. Maev, A.N. Kazyulin, Yu.A. Curly / chronic pancreatitis. - M.: Medicine, 2005. - 504 p. 8. Ivashkin V.T., Khazanov A.I., Piskunov G.G. et al. On the classification of chronic pancreatitis // Klin, honey. - 1990. - No. 10. - P.96–99. 9. Yakovenko, A.V. Practical approaches to the treatment of chronic pancreatitis / A.V. Yakovenko, N.A. Agafonova, E.P. Yakovenko // Experiment. and clinical Gastroenterology. - 2007. - N 6. - C. 67–70. 10. Sarles H., Pastor J., Pauli Am, Barthelemy M. Determination of Pancreatic Function. A Statistical Analysis Conducted in Normal Subjects and in Patents with Proven Chronic Pancreatitis (Duodenal Intubation, Glucose Toolence Test, Determination of Fat Content Content In the Stols, Sweat Test) // Gastroenterol. 1963. Vol. 99. P. 279–300.