Drug-induced hepatitis
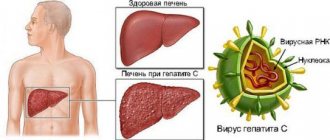
The most important function of the liver in the body is to neutralize and render harmless toxic substances entering it through the bloodstream. Metabolism and utilization of chemical and biological toxins occurs under the influence of the enzymatic neutralizing system of hepatocytes, with the subsequent removal of harmful products from the body. The process of utilization of toxic substances occurs in the liver in several stages, during which metabolites are formed - intermediate products of biotransformation. Metabolites of some drugs are even more hepatotoxic than the pharmaceuticals themselves. Long-term use of such medications or their high dosage leads to depletion of neutralizing enzymatic systems and damage to hepatocytes, resulting in the development of drug-induced hepatitis.
Today, more than a thousand types of medications are known that lead to the development of drug-induced hepatitis. The toxicity of drugs increases when 2-3 drugs are taken in combination, and when 6 or more drugs are taken simultaneously, the likelihood of toxic liver damage increases to 80%. The rate of development of drug-induced hepatitis while taking medications varies from several days to several years.
Risk factors for the development of drug-induced hepatitis include genetically determined hypersensitivity to any drug; the presence at the time of taking the drug of chronic hepatitis, viral hepatitis, autoimmune hepatitis, ascites; alcohol intake or toxic effects of solvents, poisonous gases during drug therapy; pregnancy; protein deficiency in the diet; stress; renal failure, heart failure, etc.
The main groups of drugs that cause drug-induced hepatitis include:
- Drugs for the treatment of tuberculosis (rifampicin, isoniazid)
- Antibiotics: tetracyclines (tetracycline, chlortetracycline, dixycycline), penicillins (benzylpenicillin, amoxicillin, etc.), macrolides (erythromycin)
- Sulfonamides (sulfamethoxazole + trimethoprim, sulfadimethoxine, etc.)
- Hormones (steroid hormones, oral contraceptives, etc.)
- NSAIDs (diclofenac, ibuprofen)
- Anticonvulsants and antiepileptic drugs (phenytoin, carbamazepine, clonazepam, etc.)
- Antifungal drugs (amphotericin B, ketoconazole, fluorocytosine)
- Diuretics (hydrochlorothiazide, furosemide, etc.)
- Cytostatics (methotrexate)
- Drugs for the treatment of arrhythmia, diabetes, peptic ulcers and many others. etc.
The list of drugs that have hepatotoxic effects is far from exhausted by the medications mentioned above. Drug-induced hepatitis can be caused by almost any drug and especially by a combination of several drugs.
Classification of drug-induced liver injuries
Acute drug-induced hepatitis.
Occurs when using anti-tuberculosis drugs, aminoglycosides, antihypertensive drugs, antifungal, antiandrogenic drugs; tacrine, pemolina, clozepam; nicotinic acid preparations. In the liver of patients, necrosis and inflammatory infiltration can be detected. Develops approximately 5-8 days from the start of taking the drug.
Chronic drug-induced hepatitis.
Occurs when using isoniazid, fibrates (clofibrate), minocycline, nitrofurans. Acinar and periportal lesions can be found in the liver of patients; plasma cell infiltrates, fibrosis. Clinically it occurs as autoimmune hepatitis.
Liver damage as a hypersensitivity reaction.
Occurs when using sulfonamides, nonsteroidal anti-inflammatory drugs, antithyroid drugs; quinine drugs, anticonvulsants. Develops 2-4 weeks from the start of taking the drug. Patients present with symptoms of acute hepatitis with severe jaundice; arthritis, vasculitis, eosinophilia and hemolysis. In the liver of patients, one can detect “variegated” necrosis, involvement of bile canaliculi in the process, eosinophilic infiltration of the hepatic parenchyma; formation of granulomas is possible.
Drug-induced tubular cholestasis.
Occurs when using oral contraceptives containing estrogens and gestagens, androgenic and anabolic steroids. Patients are concerned about skin itching (with a slight increase in bilirubin levels). A transient increase in liver aminotransferase levels can be detected. Signs of cholestasis may be detected in the liver (mainly in zone III).
Parenchymal tubular cholestasis.
Occurs when using chlorpromazine, sulfonamides, semi-synthetic and synthetic penicillins, macrolides, histamine receptor blockers, oral hypoglycemic drugs - sulfonylurea derivatives. In patients, cholestatic syndrome may persist for several months and years after discontinuation of the drug. Signs of cholestasis may be detected in the liver (in zones I and III); eosinophil infiltrates, possible formation of granulomas.
Intraductal cholestasis.
Occurs when using benoxyprofen. Patients experience severe jaundice and may develop acute renal failure. In the liver, the ducts and tubules are filled with clots of concentrated bile without an inflammatory reaction in the surrounding tissues.
Drug-induced biliary sludge.
Occurs when using cephalosporins. This type of liver damage may be asymptomatic. In some cases, patients are bothered by attacks of biliary colic. Agglomerates of cholesterol crystals, mucin, calcium bilirubinate and other pigment crystals are found in the liver. These changes are the result of a violation of the physicochemical properties of bile.
Drug-induced sclerosing cholangitis.
Occurs when chemotherapy drugs are administered into the hepatic artery. Patients experience persistent cholestasis.
Drug-induced liver tumors.
Occurs when using hormonal drugs (estrogens, androgens, gestagens) and their antagonists. Variants of this type of liver damage are: focal nodular hyperplasia, adenoma, hepatocellular carcinoma.
Forecast
Depends on the severity of the damage - some drugs lead to pronounced functional failure, others create the prerequisites for the formation of cirrhosis due to a moderate but long-lasting toxic effect. Recovery is possible if a drug-induced injury is detected in a timely manner, which occurs acutely, but is not associated with massive death of hepatocytes.
The chronic form has an unfavorable prognosis, since it is often detected at the stage of cirrhotic changes.
They cannot be eliminated - you can only slow down or temporarily stop the progress, however, non-compliance with the diet, alcohol consumption, continued use of toxic drugs or an infectious liver disease leads to the so-called adaptation failure. An organ that functions under conditions of loss of some of the necessary cells cannot cope with the increasing load, and decompensation occurs (which is manifested by a picture of liver failure).
Nutrition
Plays a very important role in treatment - both during the period of severe manifestations and during the recovery stage. Table No. 5 according to Pevzner is used, an example menu for which can be presented in the table:
| Type of food | Allowed | Prohibited |
| First meal | Vegetable soups (without pre-frying the ingredients). | Cooked based on meat, fish, mushrooms, including legumes, sorrel, spinach. You can't eat okroshka. |
| Side dishes | Puree viscous porridges (semolina, oatmeal, rice, buckwheat). Pilaf with dried fruits, boiled pasta. | Peas, pasta with sauce. |
| Meat | Lean varieties of beef, chicken, steamed or boiled in water. Definitely crushed. | Offal, sausage, canned food. |
| Fish, seafood | Pike perch, cod, hake, occasionally lightly salted versions of salmon or salmon, boiled shellfish in small quantities. | Caviar, sushi, sprats, smoked, salted fish. |
| Sweets | Bran and rye bread, crackers. Marmalade, marshmallow, honey, marshmallow. Sugar – limited. | Chocolate, cocoa, halva, fatty cream. |
| Vegetables | Potatoes, pumpkin, beets, cauliflower, carrots, zucchini. Bell peppers and cucumbers are also allowed. Processing – cooking, oven. | Tomatoes, sorrel, spinach, radish, eggplant, onions, herbs. |
| Fruits, berries | Baked sweet apples, compotes, dried apricots, raisins. | Raw species. |
| Milk, fermented milk food | Cheese, sour cream, low-fat kefir, yogurt without additives. | Cream, cottage cheese with a high fat content. |
| Beverages | Juice without sugar, compote, tea. | Coffee, hot chocolate, Fanta, Cola and analogues, alcohol. |
The diet for drug-induced hepatitis is followed for a long time, it provides a gentle regime for the liver, so it is very important to adhere to the diet recommended by the doctor.
Diagnostic methods
- History taking
- Physical examination
- Laboratory research
- Instrumental diagnostic methods
- Diagnostic algorithm
- Diagnosis of drug-induced liver damage is based on medical history, namely:
- Information about the drug the patient was taking.
- Dose of the drug.
- Duration of taking the drug.
- Information about previous use of the same drug and reactions to it.
In addition, it is important to establish a temporal relationship between the identified clinical and laboratory data and the use of the drug.
It is necessary to evaluate the dynamics of the identified clinical and laboratory data after discontinuation of the drug, as well as to study the patient’s condition after repeated (accidental) administration of the same drug.
To confirm the diagnosis and carry out differential diagnosis, it is important to conduct a morphological examination of the liver biopsy.
In addition, additional examination of the patient is carried out to exclude other liver diseases.
Clinical signs of toxic hepatitis
Signs of an acute form of the disease
Symptoms of toxic hepatitis are very variable and in most cases depend on the degree of poisoning and on which particular toxic substance provoked the development of the pathological process.
However, there are also characteristic signs that are common to all types of toxic hepatitis:
- fast fatiguability;
- loss of appetite;
- bitterness in the mouth;
- belching;
- bloating;
- pain in the right hypochondrium;
- yellowing of the sclera, skin and mucous membranes;
- increase in body temperature to 37–38 °C.
Many patients with toxic hepatitis develop a rash on the skin, accompanied by itching of varying intensity, urine becomes the color of dark beer, and stool becomes light-colored with a clay consistency. Often, liver damage is accompanied by an increase in the size of the organ, the appearance of small hemorrhages on the skin, bleeding gums and nosebleeds (a consequence of the destructive effect of toxic substances on the walls of blood vessels). In some cases, lethargy or excessive agitation, hand tremors, and spatial disorientation are observed.
Signs of a chronic form of the disease
As the disease becomes chronic, the symptoms of toxic liver damage become less pronounced. Typically, patients complain of the following symptoms:
- periodic pain in the right hypochondrium, worsening after eating;
- bitterness in the mouth;
- decreased performance;
- fatigue;
- flatulence;
- nausea;
- occasional bouts of vomiting;
- stool disorders;
- hepatosplenomegaly (marked enlargement of the liver and spleen).
During remission, symptoms may subside, but during an exacerbation they reappear.
Diagnostics at the clinical hospital on Yauza
Diagnosis of liver damage in the clinical hospital on Yauza is aimed primarily at establishing the cause that led to toxic liver poisoning. To do this, a conversation is held with the patient, during which it becomes clear what medications the patient used, in what conditions he works, whether he abuses alcohol, whether he was exposed to any other toxic substances, in what doses the substance entered the body, etc.
To make an accurate diagnosis and select the most appropriate treatment regimen, the patient is sent for examination, which consists of laboratory and instrumental diagnostics.
Laboratory diagnostics include:
- blood chemistry;
- general blood analysis.
A general blood test allows you to assess the condition of the body as a whole, while a biochemical study gives a detailed picture of the functional state of the liver, kidneys, and pancreas, which often also suffer from poisoning. Particular attention is paid here to the level of liver enzymes and their ratio. Total, direct and free bilirubin, aspartate aminotransferase, alanine aminotransferase, cholinesterase, albumin, and prothrombin index are assessed.
Instrumental diagnostics includes:
- Ultrasound of the abdominal organs;
- esophagogastroduodenoscopy.
- CT and MRI;
- fibroelastography;
- according to indications - endosonography.
All studies in our hospital are carried out using modern, highly informative equipment, which allows us to quickly and accurately diagnose liver lesions and determine the stage of the disease.