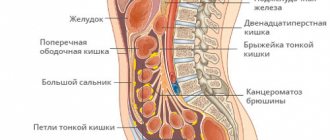
Classification
There are 6 main forms of benign tumors of the esophagus:
- esophageal leiomyoma (arising from the muscle tissue of the esophagus);
- cysts (thin-walled formations with fluid inside);
- neurofibroma (arises from the nerve sheath);
- hemangioma (arising from the blood vessels of the esophagus);
- fibroma (arising from the connective tissue of the esophagus);
- lipoma (arises from adipose tissue).
Polyps can be located in any part of the esophagus. They are most often found in the cervical or abdominal region. These tumors can grow on a broad base or a long stalk. Usually these formations are removed during endoscopic examination.
Esophageal cysts are not true tumors: their formation is associated with blockage of the mucous glands when embryogenesis is disrupted. Most often, cysts form in the lower third of the esophagus. They are thin-walled formations filled with clear, yellowish or hemorrhagic fluid.
Diagnosis and removal of complex esophageal tumors using modern endoscopic methods
Tumors of the esophagus are not uncommon in the clinical practice of a surgeon. One of them, esophageal leiomyoma, is a benign tumor of smooth muscle tissue; in half of the cases it remains asymptomatic and is often an incidental finding during gastroscopy.
If the formation reaches a large size, dysphagia (problems with swallowing) and pressing pain in the chest may appear; less often, patients complain of heartburn, weight loss, and nausea. With large tumor sizes and in a number of other cases, indications for surgical intervention arise, and here endoscopic methods of diagnosis and treatment become especially relevant. They allow us to assess the situation in great detail and carry out an intervention that minimizes various risks (in particular, postoperative ones) and contributes to the rapid rehabilitation of the patient.
Patient, diagnosis
The patient is 35 years old. Diagnosis: tumor (leiomyoma) of the lower third of the esophagus.
How events developed
The patient was routinely examined at her place of residence in May 2020, and a computed tomography scan of the chest was performed, in which an incidental finding was a neoplasm at the level of the lower third of the thoracic esophagus measuring about 6 cm (Fig. 1 and 2).
Rice. 1
Rice. 2
Gastroscopy revealed a nonepithelial tumor of the esophagus with compression of the esophagus in the middle third. Oncologists recommended observation. However, another problem arose: after the patient learned about the existence of the tumor, she began to experience discomfort when swallowing and passing food through the esophagus.
The patient contacted the National Medical Research Center for Surgery named after. A.V. Vishnevsky in order to resolve the issue of further treatment. Additional diagnostic procedures were performed. An endosonographic study (endoUS) visualized a non-epithelial tumor of an oval shape, with a clear, even contour, measuring 3x6 cm with calcifications in the structure, emanating from the muscular layer of the esophagus (Fig. 3).
Rice. 3
How the decision was made
Taking into account the results of the examination and the large size of the tumor, it was decided to perform an operation using minimally invasive endoscopic technologies - thoracoscopic removal of the esophageal tumor using intraoperative navigation.
A feature of the situation - in addition to the size of the tumor - was its extra-organ growth, as well as its proximity to the vital anatomical structures of the mediastinum and chest: the anterior surface of the tumor was adjacent to the inferior vena cava and the left atrium, and the left surface was adjacent to the aorta. Taking these circumstances into account, a 3D virtual computer reconstruction was performed, in which the spatial relationship of the tumor with adjacent anatomical structures was assessed (Fig. 4, 5).
Rice. 4
Rice. 5
The essence of surgery
During surgery, a thoracoscopic approach was used, when the operation is performed through three small punctures ranging in size from 5 to 10 mm. During the operation, the right lung is temporarily switched off (collapsed) to gain access to the tumor.
Once the tumor was found (Fig. 6), through careful precision dissection, it was isolated from the wall of the esophagus and adjacent anatomical structures and removed without opening the lumen of the esophagus itself.
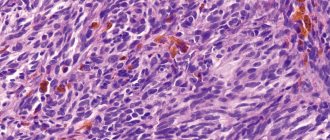
The wall of the esophagus at the location of the tumor was sutured in layers with interrupted sutures. A nodular neoplasm of irregular shape, 7.5 x 4 x 1.5 cm, was removed (according to the histological conclusion - esophageal leiomyoma).
During control intraoperative esophagoscopy, the lumen of the esophagus is not deformed, we can easily pass through the endoscope.
The use of thoracoscopic access to the esophagus made it possible to avoid a large traumatic incision of the chest (thoracotomy), minimize postoperative pain and discharge the patient on the 4th day after surgery.
Rice. 6
Surgeon's comment
Yuri Gennadievich Starkov, Doctor of Medical Sciences, Professor, Head. Surgical Endoscopic Department of the National Medical Research Center of Surgery named after. A.V. Vishnevsky, member of the board of the Russian Society of Artists, Russian Society of Economics, RANDO, Association of Hepatopancreatobiliary Surgeons of the CIS
In our patient, the esophageal tumor was an incidental finding rather than a disease that reduced the quality of life. However, the indication for surgical intervention in this case was the size of the formation - more than 4 cm.
We used minimally invasive treatment methods that provide a lower incidence of complications, better pain control and minimization of respiratory disorders after surgery, shorter hospital stay and faster rehabilitation.
Today, endoscopic technologies make it possible to perform many surgical interventions for non-epithelial formations of the esophagus. A significant proportion of these tumors are removed by intraluminal endoscopic surgery using submucosal tunneling dissections (STER).
And in this context, it is important to name two key links in the work of the surgical endoscopic department. The first is the use of the most modern diagnostic methods and surgical treatment. The second is a personalized approach to choosing the optimal type of surgical intervention for each patient in accordance with his specific clinical situation.
Operations team
Operators: Yu.G. Starkov, S.V. Dzhantukhanova Assistants: A.A. Zvereva, P.K. Kontorshchikov Anesthesiologist: A.Yu. Ershova Operating nurse: N.V. Kalashnikov
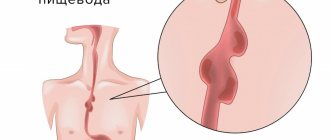
Symptoms
The main symptoms are dysphagia and pain .
Dysphagia (impaired passage of food through the esophagus) usually progresses slowly.
The clinical course of benign esophageal tumors depends mainly on the size of the tumor and its location. The course at the initial stage of the disease, when the tumor is still small, may be asymptomatic. When the tumor grows in size over time, it can gradually block the lumen of the esophagus or compress neighboring organs.
Postoperative follow-up
After the operation, 3-4 incisions 5-10 mm long remain on the skin of the abdomen. From the first day, patients begin to get out of bed, drink, and on the second day take liquid warm food. Discharge from the hospital is carried out on 3-4 days, depending on the severity of the disease. The patient can begin work in 2 - 3 weeks. A strict diet should be followed for one and a half to two months, a softer diet should be followed for 2-3 months. Further, as a rule, the patient leads a normal lifestyle - without medications or diet.
In the postoperative period, gastroesophageal reflux often develops, which may require repeated antireflux surgery. Unfortunately, it is extremely rare (due to the presence of many sutures on the esophagus and the danger of their failure) that it is possible to perform antireflux surgery (fundoplication) immediately during tumor removal. During surgery for esophageal leiomyoma, I always perform cardiopexy. In most cases, this intake is enough to prevent the onset of GERD symptoms.
At the request of patients, the clinic can undergo a full examination before surgery to determine the optimal treatment tactics and choose the method of surgical intervention.
Diagnostics
- Esophagogastroduodenoscopy (EGD) is a diagnostic procedure during which the doctor examines and evaluates the condition of the inner surface of the esophagus, stomach and duodenum using a special optical instrument (endoscope). If a mass in the esophagus is detected, a biopsy is taken to further examine it and determine the tactics of examination and treatment. If a polyp of the esophagus is detected, it can be immediately removed by taking biopsy material.
- X-ray examination of the esophagus with contrast (the patient drinks a barium suspension, as a result of which the accuracy of the study increases, since barium is clearly visible on the x-ray). Used to identify irregularities in the esophagus, which may indirectly indicate the presence of tumors in the esophagus.
- Transesophageal ultrasound . If a formation of the esophagus is suspected, an endoscopy of the esophagus is performed, in which an ultrasound sensor is inserted into the esophagus, which determines the thickness of the walls of the esophagus and the location of the formation, the degree of invasion of the wall.
- Computed tomography (CT) with contrast is also an informative study. It allows you to clarify the size, location and possible invasion of neighboring structures by this formation.
- Magnetic resonance imaging (MRI) is done to identify tumors in the esophagus.
Surgical technique for esophageal leiomyoma.
Watch a video of operations performed by Professor K.V. Puchkov. You can visit the website “Video of operations of the best surgeons in the world.”
Due to the location of the tumor outside the mucosa, in most cases it is possible to remove the leiomyma from the wall of the esophagus. Traditionally, thoracotomy is used (left- or right-sided, depending on the level of localization of the leiomyoma). Which leads to major trauma to the chest wall, poor cosmetic effect and a long recovery period.
Puchkov K.V., Ivanov V.V. and others. Technology of dosed ligating electrothermal effects at the stages of laparoscopic operations: monograph. - M.: ID MEDPRACTIKA, 2005. - 176 p.
Puchkov K.V., Bakov V.S., Ivanov V.V. Simultaneous laparoscopic surgical interventions in surgery and gynecology: Monograph. - M.: ID MEDPRACTIKA, 2005. - 168 p.
Puchkov K.V., Rodichenko D.S. Manual suture in endoscopic surgery: monograph. - M.: MEDPRACTIKA, 2004. - 140 p.
Our clinic has accumulated experience in video-assisted thoracoscopic and laparoscopic operations when removing esophageal leiomyomas. With this method, leiomyoma is removed without thoracotomy, through 4 punctures on the chest or abdominal wall.
Treatment
There are no effective conservative methods for treating benign tumors of the esophagus. Medicines are used temporarily and only to reduce the severity of symptoms that cause discomfort.
Surgical treatment of benign neoplasms of the esophagus . Usually, when these formations are identified, they have already reached a size that narrows the lumen of the esophagus and causes dysphagia in the patient. Surgical treatment consists of removing this formation while maintaining the integrity of the esophageal wall. These operations are performed mainly thoracoscopically, that is, through punctures.
If a benign lesion is not treated surgically, it can lead to serious adverse consequences. Namely:
- Tumor malignancy (degeneration into a malignant tumor, the cell type of which is different from the cell type of the organ from which it originated).
- Tumor perforation (formation of a hole in the wall of the esophagus with subsequent release of its contents into the chest cavity).
- Stenosis (significant reduction or narrowing of the lumen) of the esophagus - it occurs most often when the tumor reaches a large size and blocks the lumen of the esophagus.
- Tumor surface ulceration is the formation of ulcers (deep defects in the esophageal mucosa) on the surface of the tumor.
- The occurrence of bleeding from a tumor of the esophagus.
Forecasts
The postoperative prognosis is usually favorable. Relapses of the disease are rare; In almost all cases, the function of the esophagus is completely restored, and the ability to work is preserved.
Treatment of esophageal leiomyoma. Indications for surgical intervention.
To identify leiomyoma of the esophagus, its localization, as well as choose the correct surgical treatment tactics, you must send me a complete description of gastroscopy, X-ray of the esophagus and stomach with barium, preferably an ultrasound of the abdominal organs, by indicating your age and main complaints. Then I will be able to give a more accurate answer to your situation.
My experience in treating patients with esophageal leiomyomas is more than 15 years. During this time, I was able to successfully operate and treat more than 90 patients laparoscopically.
For esophageal leiomyoma, treatment should only be surgical. Due to the slow growth of this tumor, surgical treatment is indicated only in cases of dysfunction of the esophagus and severe symptoms (listed above), provided there is no increased risk of surgery. If there is no clinical picture of esophageal leiomyoma, and the size of the tumor does not exceed 5 cm (and according to MSCT with contrast, there is no accumulation of it in the tumor tissue), then you can refrain from surgical treatment in this situation. Dynamic observation is permissible if regular endoscopic and x-ray examinations are possible in one medical institution, so that if the size of the formation increases or complaints appear, indications for surgery can be established in a timely manner. When planning treatment, it is necessary to take into account that the final conclusion about the benignity and malignancy of the tumor can be judged only after histological examination, which is possible only after a biopsy of the formation.