The parasite of humans, cats and dogs, Giardia duodenalis (also known as Giardia lamblia), is distributed throughout the world, and giardiasis, caused by G. duodenalis, is the most common intestinal parasitic disease. The largest number of reported cases occur in children aged 1 to 9 years and adults aged 35 to 44 years. Most cases occur between early summer and early fall and are associated with recreational water sports (such as swimming) and outdoor activities. Humans are the main reservoir of Giardia. The parasite is also found in many animal species, although the role of zoonotic transmission is still unclear.
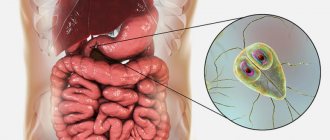
What is Giardia?
Giardia is a flagellated protozoan that comes in two forms: trophozoites and cysts. The infectious and environmentally resistant form is the cyst. Once ingested by a child, each cyst produces two trophozoites in the small intestine. The separated trophozoites pass through the intestine and form smooth, oval, thin-walled infectious cysts that are excreted in the feces. The duration of removal of a cyst usually has a finite period, but can last for months. Studies have shown that ingestion of 10 to 100 cysts of fecal origin is sufficient for infection. Giardia cysts become infectious immediately after excretion in feces and remain viable for at least 3 months in water at 4°C. Although freezing does not completely eliminate the infectivity of Giardia cysts, heating, drying, or immersing them in seawater renders them nonviable.
Is there immunity to Giardia?
Cellular and humoral immunity are formed after treatment of Giardia for a period of 2-6 months. During this time, a healthy child is protected from this type of invasion. Immunity disorders lead to the disease becoming chronic.
Recovery of the digestive system after treatment is slow. Abdominal pain and bloating may persist for some time. In some cases, such manifestations indicate incomplete treatment. Diagnostics 1-2 weeks after completion of treatment can detect parasites again.
The doctor will determine whether this can be considered a failure of therapy, or whether the patient has re-invaded. In any case, the specialist will prescribe an effective treatment regimen and monitor its effectiveness.
How does Giardia infection occur?
Giardia infection can occur directly through the fecal-oral route or indirectly through ingestion of contaminated water or food. Water contaminated with Giardia cysts appears to be the main reservoir and means of spread of the parasite. Most outbreaks of waterborne giardiasis have been associated with the consumption of untreated or improperly treated surface water. Transmission of giardiasis from person to person often occurs in child care institutions and in families where there are children with diarrhea. Human immune defense is dependent on B cells, with secretory immunoglobulin A playing a major role in immunity. Children with humoral immunodeficiencies, such as X-linked agammaglobulinemia and hypogammaglobulinemia, who develop giardiasis are predisposed to chronic disease.
G. duodenalis infection is more common in certain high-risk groups, including children, staff and visitors of child care facilities, patients and staff of institutions for people with developmental disabilities, people who drink contaminated drinking water or water from lakes, rivers or insufficiently treated swimming pools, travelers to endemic areas of the world, close contacts of people with Giardia, people taking antibiotics, and people in contact with domestic and wild animals (eg dogs, cats, cattle, deer and beavers).
What are the symptoms and signs of giardiasis?
The incubation period of the disease usually lasts from 1 to 2 weeks, averaging 7 days. Infection with G. duodenalis can cause a wide range of clinical manifestations. Children usually present with short-term, acute, watery diarrhea with or without low-grade fever, nausea, anorexia, and abdominal pain. In other cases, the infection follows a longer, intermittent course, characterized by foul-smelling stools associated with flatulence, bloating, and anorexia. Malabsorption combined with anorexia can lead to significant weight loss, stunted growth, and malnutrition in children. The stool may initially be large and watery, but later become greasy and foul-smelling. There is no blood, mucus, or leukocytes in the stool. Varying degrees of malabsorption may occur, and abnormal bowel movements may alternate with periods of constipation and normal bowel movements. Post-infectious lactose intolerance can occur in 20% - 40% of patients. This syndrome may take several weeks to resolve and may contribute to malnutrition in children. Malnutrition and repeated episodes of Giardia infection in the early years of life are associated with cognitive decline in late childhood. In addition, a proportion of children will develop chronic gastrointestinal symptoms such as post-infectious irritable bowel syndrome (PI-IBS).
Asymptomatic giardiasis is also common. Extraintestinal invasion can occur when trophozoites migrate into the bile or pancreatic ducts. Extraintestinal manifestations were previously considered uncommon, but recent studies suggest that one third of patients will exhibit long-term extraintestinal symptoms, including ocular, muscular, and metabolic complications. The subsequent development of reactive arthritis may also be associated with giardiasis.
Allergy
Allergic reactions in children appear regardless of the severity and severity of the infectious process. This is confirmed by an increase in the level of immunoglobulins IgE and IgM, as well as eosinophils in the patient’s blood. Skin lesions in the form of atopic dermatitis are most often recorded with giardiasis (70% of cases), less often with enterobiasis (16% of cases) and ascariasis (3% of cases). In children under one year of age, allergic manifestations are very diverse - from an itchy rash to eczematous lesions.
Rice. 18. Atopic dermatitis can be a manifestation of giardiasis in children.
Diagnosis of giardiasis
A definitive diagnosis of Giardia infection is made by detecting trophozoites or Giardia cysts in stool samples, intestinal contents, or small intestinal tissue by microscopic examination using staining techniques such as trichrome. Also used are direct fluorescent antibody tests (DFA), detection of soluble stool antigens using enzyme-linked immunosorbent assay (EIA), and the use of molecular methods, including polymerase chain reaction (PCR). EIA or multiplex PCR is the main currently recommended diagnostic methodology. There are currently commercially available multiplex PCR panels for the detection of gastrointestinal pathogens, including Giardia. These tests are highly sensitive (92% to 100%) and specific (96.9% to 100%) and can simultaneously detect multiple GI pathogens.
Identification of both trophozoites and cysts can be made on direct smears of concentrated stool samples. Correctly performed direct examination of stool allows a diagnosis of giardiasis to be made in 70% of patients during a single examination and in 85% during a repeat examination. Identification of Giardia can be difficult due to the periodic release of cysts. Stool samples should be examined within 1 hour of collection. Trophozoites are more likely to be present in unformed stool due to rapid passage through the intestine. Cysts are stable outside the gastrointestinal tract.
If giardiasis is suspected and stool tests are negative, aspiration, biopsy, or both should be performed during endoscopy of the duodenum or upper jejunum. In a fresh specimen, trophozoites can usually be visualized on a direct wet mount. Histological evaluation of duodenal biopsy specimens has low sensitivity for detecting infection, however this diagnostic approach may be necessary in patients with clinical characteristics of Giardia infection but negative stool and duodenal fluid specimens. The commercially available Entero-Test is an alternative method for direct collection of duodenal fluid.
Treatment of the disease
Effective antiparasitic therapy is the main initial method of treating Giardia in children and adults. Patients should receive supportive care with hydration, correction of electrolyte abnormalities, and nutritional supplements. Drugs that reduce intestinal motility (antidiarrheals) should be used with caution in young children. Patients with chronic diarrhea should be monitored for malabsorption leading to wasting.
The therapeutic efficacy of metronidazole against Giardia has led to the development of other nitroimidazole derivatives such as tinidazole and secnidazole. The advantage of these drugs is that they have a longer half-life than metronidazole, making them suitable for single daily dose treatment. A single dose of 2 g (or an equivalent pediatric dose of 50 mg/kg in a single dose) of tinidazole has demonstrated cure rates of 80% to 100%. Cure rates for patients with giardiasis have been shown to be consistently higher with the use of tinidazole than with other antiparasitic drugs such as metronidazole, nitazoxanide, mebendazole, albendazole, and chloroquine. Tinidazole is approved for use in children aged 3 years and older. The drug is available in tablets that can be crushed into a flavored syrup for patients who are unable to swallow tablets.
Metronidazole was recognized as a therapeutic agent against giardiasis in 1962. Since then, clinicians have used metronidazole and other nitroimidazoles as the mainstay of therapy for giardiasis. Metronidazole is the drug most commonly used to treat giardiasis worldwide. Children have been included in many clinical trials of metronidazole with results similar to those in adults (average effectiveness of 94%) with 5-day and 10-day course regimens. Metronidazole is not available in standard liquid form, but a suspension can be prepared by thoroughly crushing metronidazole tablets using glycerin as a lubricant and suspending the mixture in a flavored syrup.
Side effects of tinidazole are not as common as those of metronidazole. The most common side effects of metronidazole treatment include headache, dizziness, nausea, and a metallic taste in the mouth. Nausea occurs in 5–15% of patients receiving standard multi-day courses. In addition, metronidazole has been associated with reactive pancreatitis, central nervous system toxicity at high doses, and transient reversible neutropenia.
Astheno-neurotic syndrome
In more than half of the cases of giardiasis in children, asthenoneurotic cider develops along with dyspeptic syndrome. Vitality decreases, the child gets tired quickly, headaches and dizziness appear, small children become tearful, and sleep is disturbed. Professor D. F. Lambl, who described the microorganism in 1859, called Giardia “a parasite of melancholy and sadness.”
In 50% of cases in children with giardiasis, three main clinical syndromes are simultaneously determined: dyspeptic, pain and asthenoneurotic.
Rice. 16. Headaches and tearfulness are symptoms of astheno-neurotic syndrome.
Rice. 17. The “marble” pattern of the skin indicates the reaction of the autonomic nervous system to the development of the infectious process.
Preventing relapses of giardiasis
There are no known pharmacological agents that effectively prevent relapse of giardiasis. Reinfection often occurs in endemic areas or in situations where hygiene levels are poor or contaminated water (such as private wells) is not properly treated. Re-infection can be prevented by consistent hand hygiene, especially after bowel movements and handling soiled diapers. You should also practice hand hygiene before preparing and eating food. To reduce the risk of disease transmission, children with diarrhea should be removed from childcare settings until the diarrhea stops. Children with giardiasis should not go to recreational water facilities for 2 weeks after the symptoms disappear.
Diet for lamblia in children
1-2 weeks before the start of medication treatment, changes are made to the child’s diet. The need to follow a diet is due to impaired digestion and cholestasis, and the high toxic activity of the parasite.
Fatty foods, fried foods, whole milk, carbohydrates in the form of sweets and refined foods are removed from the diet.
Children are offered porridge made from buckwheat, oatmeal, millet, baked fruits, salads and vegetable dishes seasoned with vegetable oil, cranberries and lingonberries.
It is recommended to drink medicinal mineral water (Essentuki No. 4).
Recommendations for the prevention of giardiasis
Because giardia is most often spread through contaminated water and food or contact with an infected person or animal, you should avoid using untreated water sources and wash your hands with soap and water after handling potentially contaminated fecal material or contact with an infected person or animal. Alcohol-based gels are ineffective against Giardia cysts and should not be used as a substitute for hand washing when there is a risk of Giardia infection.
In the hospital, standard precautions include wearing gloves and washing hands after removing gloves.
Before traveling to areas where water may be contaminated or the safety of drinking water is questionable, travelers, tourists, and vacationers should be informed of methods to make the water safe to drink.
These measures include using bottled water, disinfecting the water by heating it to a boil for 1 minute, or using a filter that has been tested and certified to NSF Standard 53 or Standard 58 to reduce cysts and oocysts. Outbreaks of waterborne giardiasis can be prevented by a combination of proper filtration of water sources, chlorination, and maintenance of water distribution systems. Travelers should also be advised of the possibility of transmission of giardiasis through the use of contaminated water for recreational purposes (eg, lakes, rivers, inadequately treated swimming pools). Call a doctor at home Make an appointment with a doctor or call +7 (812) 331-17-74