Causes of gas incontinence
Physiological factors
Increased gas formation and, as a result, difficulties with gas retention are provoked by the consumption of large amounts of legumes, cabbage and radishes, and whole grain products.
Increased gas formation is caused by fruits: pears and apples, grapes, peaches. If gas incontinence is caused by nutritional factors, the symptom occurs 1-2 hours after eating. In the morning before breakfast, bloating is not observed. Flatulence (gas production), which occurs in old age, is a normal variant. Incontinence is associated with age-related weakening of the muscular apparatus of the anal sphincter. The problem is aggravated by a deficiency of digestive enzymes, which causes partially digested food to accumulate in the intestines, leading to increased gas formation.
Irritable bowel syndrome
With IBS, intestinal motility and coordination of the muscular sphincters of the rectum are impaired. The disease is characterized by gas incontinence without bloating. The patient is not able to control this process; sometimes a person becomes aware of an unpleasant situation only when a specific smell appears. Less commonly, flatulence develops against the background of severe pain in the rectum. Symptoms typically worsen in the morning and improve after bowel movements.
Anal sphincter insufficiency
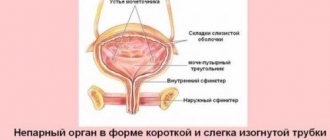
Isolated gas incontinence is characteristic of the first degree of the disease, when the act of defecation has not yet been disrupted. At the second stage of insufficiency, the separation of not only intestinal gases, but also liquid feces is not controlled - the so-called “wet anus”. In the third degree, the patient cannot retain gases, liquid and formed feces. Incontinence and other symptoms are not related to eating habits. Incompetence of the anal sphincter is caused by the following diseases:
- Proctological pathology
. External and internal hemorrhoids, rectal fissures and fistulas, rectal prolapse. - Injuries
. Perineal rupture after childbirth, consequences of sphincterotomy, household injuries. - Anorectal anomalies
.
Intestinal diverticula
With intestinal diverticulosis, increased gas formation is constantly observed, which inevitably leads to flatulence. Diverticula are characterized by rumbling in the abdomen and the passage of gases with a strong unpleasant odor. The condition is aggravated by errors in diet. With diverticulosis, incontinence is also accompanied by pain and cramps in the abdomen, and irregular bowel movements similar to “sheep feces.”
Gynecological diseases
Pathologies of the internal genital organs are the main cause of gas incontinence in gynecological practice. The symptoms are due to the close location of the gastrointestinal tract and genitourinary system and their joint innervation. Incontinence is more often diagnosed in women after 50 years of age, but can also affect patients of reproductive age after multiple births. The main diseases that may cause gas incontinence are:
- Pelvic floor dysfunction.
The symptom occurs with “posterior prolapse,” when the rectum descends along with the vaginal wall and a rectocele occurs. Uncontrolled release of gases occurs during physical exertion, laughter, and in advanced stages of the disease it occurs without provoking factors. - Prolapse of the uterus.
Incontinence is observed in a third of women with this pathology. Often the patient is unable to retain both gases and liquid feces. When the uterus prolapses or prolapses, proctological symptoms are combined with urological ones - urinary incontinence, frequent painful urination. - Elongation of the cervix.
Increased gas production is observed in 15% of women suffering from elongation of the uterine cervix. The sign is typical for stage 2-3 disease. Spontaneous flatulence appears when coughing, sneezing, or laughing. Urine leakage usually occurs simultaneously, and in severe cases, fecal incontinence.
CNS damage
Flatulence is associated with damage to the parts of the spinal cord that are responsible for the innervation of the rectum and anal sphincters. Less commonly, incontinence is caused by damage to certain areas of the brain. Uncontrolled passage of gases is combined with involuntary passage of feces and urine. A similar clinical picture is observed with spinal and head injuries and demyelinating diseases.
Mental disorders
In patients with mental disorders, control over the passage of gases is lost. In this case, the disorder develops during normal bowel function and does not depend on diet. The symptom is most characteristic of senile dementia, schizophrenia, and bipolar disorder. Sometimes gas incontinence worries patients with neuroses and post-stress psycho-emotional disorders. The condition is completely normalized after eliminating the stress factor.
Incontinence of feces and gases
Incontinence of feces and gases is associated primarily with disturbances in the functioning of the sphincters - special muscles that prevent prolapse of the contents of the rectum. Sphincters can be damaged during surgery to remove hemorrhoids, polyps, and fimbria. Incontinence can occur after pregnancy or due to rectal prolapse. Your doctor can determine the exact causes of incontinence.
Degrees of incontinence
According to the degree of insufficiency of the anal sphincter, incontinence is divided into 3 types:
Incontinence degree I
Mild form of incontinence. The patient cannot control the release of gases. Leakage of feces is observed with the urge to defecate.
Incontinence degree II
Gases and feces are released involuntarily. At the same time, there was no desire to empty the intestines.
Incontinence degree III
A severe form of pathology in which not only gases and liquid feces, but also solid feces are released uncontrollably.
Causes and risk groups
Bowel incontinence usually occurs in older people. It is often accompanied by urinary incontinence. Patients with chronic bowel dysfunction also suffer from anal incontinence. Sphincter dysfunction can be caused by surgery.
However, there are also situations when incontinence occurs in healthy people for a number of reasons:
- food poisoning
- excessive physical stress
- stress, etc.
Diagnostics
A proctologist diagnoses and treats diseases of the intestines and anus. To diagnose incontinence, a doctor simply needs to listen to what is bothering the patient. Further diagnostic measures are prescribed to identify the causes of the pathology and choose a treatment method. The following methods are used for this:
- study of sphincter muscle tone
- identification of pathologies and defects of the sphincter
- measuring the level of sensitivity of the rectum
Treatment of fecal incontinence
Treatment tactics are selected depending on the root cause, the age of the patient and the degree of development of the pathology.
Surgery
Used for injuries and defects of sphincter fibers. Based on the extent of the lesion, the doctor can choose one of four types of surgery: sphincteroplasty, Thiersch operation, sphincterogluteoplasty, Faerman method. The surgical intervention is plastic in nature.
Drug treatment
Prescribed for disorders of the gastrointestinal tract. Two groups of medications are used for therapy. The first is aimed at normalizing the functions of the digestive and excretory systems. The second tones the muscles of the anus. In some cases, tranquilizers are additionally prescribed to reduce the patient's excitability.
Non-drug treatment
It is used in the initial stages in the absence of sphincter defects and gastrointestinal pathologies. Various methods are used for treatment:
- Kegel and Dukhanov physical exercises. The doctor lubricates a special tube with Vaseline. Then he carefully inserts it into the patient's rectum. The patient begins to tense and relax the anus. One approach takes up to 15 minutes. 5 procedures must be performed per day. The course of treatment averages 5 weeks. Additionally, exercises may be prescribed to strengthen the abdominal and gluteal muscles.
- Biofeedback. An elastic balloon is inserted into the anus. The patient needs to squeeze it. Process data is sent to the computer.
- Electrical stimulation. The nerve endings of the sphincter are exposed to current. In this way, the muscles are literally trained to contract and control bowel movements.
- Psychotherapeutic methods. Effective only for psychological causes of incontinence. Based on the development of reflexes to acts of defecation in a specific place and time.
Don't be shy about proctological problems. If the pathology is not treated in time, it can progress and ultimately cause you not only physical, but also psychological problems.
Diagnostics
During a physical examination, the proctologist draws attention to the gaping of the anus; with fecal incontinence, maceration of the skin around the anus is observed. To assess the closing function of the sphincter and identify signs of rectal pathology, a digital rectal examination is performed. To diagnose the causes of gas incontinence, the following laboratory and instrumental studies are used:
- Functional methods.
To study the contractile function and tonic tension of the anal sphincter, sphincterometry is indicated. Electromyography allows you to assess muscle tone. Diagnosis of reflex contractility of the anus is made by profilometry. - Sigmoidoscopy.
Endoscopy is the most informative method of visualizing the rectal mucosa. During the study, the doctor identifies inflammatory, erosive and tumor processes. If intestinal diverticula are suspected, a colonoscopy is required. - Radiography
. X-ray examination with oral contrast is informative for measuring the anorectal angle, studying the size and relief of the rectal mucosa. For a more detailed examination, irrigoscopy with double contrast is necessary. - Gynecological examination.
All women who complain of gas incontinence are advised to consult a gynecologist. The doctor performs a standard vaginal speculum examination. If a pathology is found, colposcopy, hysterosalpingoscopy, and ultrasound of the pelvic organs are indicated.
Treatment
Diet
All patients who are concerned about gas incontinence are prescribed conservative measures that are aimed at reducing gas formation in the intestines. Foods that cause flatulence are excluded from the diet. You need to eat small meals 4-5 times a day. While eating, it is important to chew food thoroughly and avoid aerophagia (swallowing air). To reduce gas formation, you must stop smoking and chewing gum.
Conservative therapy
Treatment depends on the cause of gas incontinence. In case of functional disorders (IBS), it is necessary to eliminate stress and provoking factors and carry out diet therapy. For hemorrhoids, electrocoagulation, sclerotherapy of hemorrhoids, and ligation with latex rings are performed. To eliminate the insufficiency of the sphincter apparatus, drugs are indicated that increase the excitability of nerve endings.
For functional sphincter insufficiency, physiotherapeutic treatment is effective. Electrical stimulation is useful to increase the tone of muscle fibers. A promising direction of therapy is the biofeedback method. The essence of the technique is to train the muscles of the pelvic floor and anus, which allows the patient to control the release of gases. Special exercise therapy complexes are also prescribed.
Surgery
In case of severe damage to the anal sphincter, surgeons perform plastic surgery: sphincteroplasty or sphincterolevatoroplasty. After interventions, as a rule, the obturator function of the anus improves. If these methods are ineffective, a new sphincter apparatus is formed. For anorectal defects, various methods of surgical correction are used.
Gas incontinence, which develops with gynecological diseases, disappears after the issues with the underlying disease are resolved. Women undergo surgery to strengthen the pelvic floor muscles. In case of serious pathologies, combined surgical treatment is performed, which involves fixation of the uterus, vaginal plastic surgery and strengthening of the muscular-ligamentous apparatus.
Night gases in a child
Elena
October 2, 2021
Girl, one year and 2 months.
Breastfed for up to a year. There were problems from birth. At 2 months old, she began regular treatment with a gastroenterologist. At the age of 2-3 months, greenish loose stools 4-5 times a day plus frequent regurgitation. And also night gases, which cause the child to toss around half the night and sleep restlessly. On the doctor’s recommendation, I followed a dairy-free diet during breastfeeding because the doctor believed that the child had intolerance to cow’s milk protein. She made this conclusion due to the presence of leukocytes in the coprogram. Until the introduction of complementary foods at 5.5 months, the situation did not change, although they tried to treat Primadophilus with enterofuril and enterol and prebiotics. They also diagnosed lactase deficiency, which was treated with lactazar. There was no effect. With the introduction of complementary foods, it became a little better, regurgitation disappeared. The stools stopped being so frequent, but still were not formed, and over time, the leukocytes in the coprogram also disappeared. But the night gases did not go away, although the colic had already ended. At night I had to give drops with simethicone almost every night (which I still do now, since the problem has not gone away), and massage the abdomen. Later, at 6-7 months, according to tests for dysbacteriosis, I treated the child with sporobacterin for 10 days and after Acipol the baby for 2 weeks. I didn't feel the effect. At the age of 8 months, due to the fact that the daughter slowly began to refuse breastfeeding, she introduced a small amount of Nestozhen formula, which she, by the way, didn’t drink much either, and at that time we went on vacation to Turkey for a month. During the first week, my daughter, as usual, tossed around at night due to gas and farted. But little by little it somehow went away by itself and I began to notice that I even stopped giving her drops at night. And her stool became hard and formed. In Turkey, I began to feed her more variedly, including adding butter to the porridge, and began introducing fish, even red fish, oranges, and strawberries. There were no rashes. And before the trip, she had dry spots in different parts of her body, they all went away on their own at sea. But we also had an episode during that trip when one night she didn’t sleep at all until four in the morning. She spun around every 20-30 seconds, cried, farted, drops did not help although she was given several times. Only in the morning did we fall asleep. The day before at 5 pm she gave her sweet yogurt, which she had not eaten before. I thought it was because of him. As soon as we returned home on the first night, everything happened again. She sank to her stomach, twisted and cried. Everything as usual. The coprogram that we took again showed that there was undigested fiber. The doctor prescribed Creon for 3 weeks, 3 times a day with food. She scolded me for not using formula (milk formula) and said that it was an allergy to BCM that was the cause of night gases. There was no effect from Creon. I began to slowly transfer the child from Nestozhen to a hydrolyzed formula. Now we are completely on this mixture, dairy-free diet, I try not to give fruits and vegetables after 4 pm. Dinner is mostly porridge with turkey. I also don’t give beef, again due to intolerance to BCM. I tried giving children's curds for a week, the night's sleep did not become any worse or better, the gases were as they were. But dry spots appeared on my legs, I suspect that after the cottage cheese. We also managed to catch an intestinal infection when we were one year old. We ended up in the hospital with vomiting. There they fed him with rehydron and treated him with Motilium, Smecta, and Enterouril once. After the hospital, Creon and prebiotics for 2 weeks. Another 3 weeks later, for the first time after the hospital, I gave her a quail egg for breakfast, and at lunch she vomited. Another 10 days after the egg for breakfast, she again vomited only twice during the day. The doctors and the ambulance did not really explain whether this was the consequences of a previous infection, a new infection, or even a reaction to an egg (I had eaten eggs before and this had never happened). Now I'm afraid to give. There are very rare nights when the daughter sleeps and is not disturbed by anything, maybe 2-3 nights a month, but consistently from one in the morning until three or four she begins to fidget, get up and try to cry. At the same time, the stomach is not inflated and soft, but during the massage it gurgles in places and feels like gas, then it farts and sleeps normally. Sometimes there is no gurgling, just a soft belly. I thought maybe she was spinning from hunger, I feed her formula at 4-5 in the morning. Unformed, soiling stools, often undigested food, happen up to 3 times a day. I don’t know if this is after an illness or maybe because of the mixture. Weight 8900. After illness almost 2 months ago, I weighed 8400. But in general, I’m not gaining weight well. He eats cereals, vegetables, sometimes white bread, children's cookies, turkey-chicken, and rarely rabbit. Fruit: apple, banana, nectarine. Even the gastroenterologist began to doubt that it was her stomach that was bothering her at night and referred her to a neurologist. She prescribed Dormikind, we take it for a week, I don’t see any difference. We took him to the doctor again, and based on tests, the pediatrician prescribed polyvalent pyobacteriophage. Today we started taking it. Help me figure out why a one-year-old child still suffers from stomach pain, or maybe it’s not his stomach that’s bothering him at all, why he doesn’t have a normal night’s sleep. How to help her. Chronic diseases:
No
The question is closed
dysbacteriosis
gases
child has poor sleep