Until recently, cholecystitis was considered a disease of the adult population. But every year the disease becomes “younger”; now the pathology is increasingly common in children.
This is facilitated by poor nutrition, parasitic infections and many other factors. The disease is diagnosed using ultrasound. The disease is dangerous for a child, as it leads to serious complications, which may even require removal of the gallbladder.
Therefore, at the first symptoms, parents should consult a doctor and begin treatment. For therapy, medications, diet, and herbal treatment are used. With adequate timely therapy, the prognosis is favorable.
Definition of the concept
Cholecystitis is an inflammatory disease of the gallbladder
Cholecystitis is an inflammatory disease of the gallbladder. The process develops in the walls of the organ, accompanied by a violation of bile outflow and deterioration of bile motility. The following pathological processes occur with cholecystitis:
- Hyper- or hypomotility.
- Shutdown of the bladder due to blockage of the ducts by stones.
Inflammation of just one gall bladder is rare and is usually accompanied by cholangitis (inflammation of the ducts) and liver involvement (hepatocholecystitis).
Types of cholecystitis
Cholecystitis is classified according to various parameters.
Depending on the presence of stones, it can be:
- calculous, in which there are stones blocking the bile duct;
- non-calculous, or stoneless.
Considering the nature of the flow, there are:
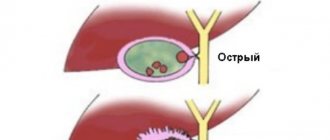
- acute cholecystitis - manifests itself with a sudden onset and violent symptoms; most often occurs in the presence of gallstones;
- chronic, which is characterized by a slow, asymptomatic course; most typical for childhood.
Depending on the nature of the changes in the gallbladder wall in the acute form, cholecystitis can be:
- catarrhal - has a fairly favorable course, characterized by superficial inflammatory changes in the wall of the gallbladder;
- phlegmonous - characterized by purulent lesions of all layers of the gallbladder wall;
- gangrenous - the most severe form, in which necrotic changes in the wall are detected, which is fraught with the development of complications.
Causes and risk factors
In children, the main causes of the disease are bacterial infections. Microorganisms with the bloodstream from other organs penetrate into the gallbladder in such chronic diseases as: sinusitis, tonsillitis, caries, pyelonephritis. Sometimes acute infections also contribute to the development of pathology: influenza, salnollosis, intestinal infection, sore throat.
Parasites play a major role in the development of childhood cholecystitis: Giardia, opisthorchid, roundworm. The gall bladder also becomes inflamed due to other gastrointestinal diseases: gastritis, pancreatitis, Crohn's disease.
Anomalies in the structure of the organ, in which reverse reflux of bile occurs, cannot be discounted. The inflammatory process can begin due to gallstones, but such cases in childhood are very rare.
Poor diet can lead to cholecystitis
Factors that provoke the appearance of the disease are:
- Incorrect diet: long breaks in food, fast food, a high percentage of carbohydrates and a small amount of plant fiber.
- Passion for fast food, sweet carbonated drinks, fatty foods.
- In infants under one year old, the disease is caused by improper feeding.
- Lack of physical activity, which leads to bile stagnation.
- Endocrine disorders (diabetes, thyroid diseases).
- Injuries to the gastrointestinal tract.
- Food allergies.
- Excessive physical and emotional stress.
- Poisoning with chemicals, mushrooms, long-term use of medications.
Causes of cholecystitis
The mechanism of development of this pathology includes the following components:
- Violation of the outflow of bile , resulting in its stagnation in the gallbladder - cholestasis. The outcome of this is thickening of the bile, creating conditions for the formation of gallstones (calculi). In addition, due to cholestasis, intravesical pressure increases, which leads to disruption of the barrier functions of the bladder wall. As a result, the risk of microorganisms entering the gallbladder increases.
- Infection of the gallbladder wall or bile itself. Penetration of the infection can occur in an ascending way - from the intestinal lumen through the common bile duct, as well as through the lymphogenous or hematogenous route from foci of infection located in other organs (oral cavity, kidneys, lungs, etc.). Most often, the cause of cholecystitis is a bacterial infection, but the development of viral inflammation (adenovirus, enteroviruses) is also possible.
There are quite a lot of factors that can affect the development of this disease, since they create conditions for the occurrence of cholestasis and the implementation of the mechanisms discussed earlier. The main ones are the following:
- genetic predisposition (heredity);
- the presence of congenital anomalies of the gallbladder and biliary tract;
- dyskinesia of the gallbladder, which is manifested by impaired tone and motility of the muscular wall of the bladder and bile ducts;
- infectious diseases affecting the liver (viral hepatitis, infectious mononucleosis, etc.);
- helminthic infestation (most often Giardia, roundworm);
- the presence of chronic or acute diseases of the gastrointestinal tract (GIT): duodenitis, pancreati, Crohn's disease, celiac disease, etc.;
- dysbacteriosis;
- duodenobiliary reflux, which is characterized by the reflux of pancreatic and gastric juices into the cavity of the gallbladder;
- metabolic disorders (diabetes mellitus, obesity);
- violation of the regime and nature of nutrition (prolonged fasting, overeating, excessive consumption of fatty and fried foods);
- sedentary lifestyle;
- tumor diseases of the liver and pancreas.
Stages and types
Acute and chronic cholecystitis occurs in children. Acute develops rapidly and is accompanied by severe symptoms. Chronic is a consequence of improper treatment of the acute stage. It also develops against the background of chronic diseases.
According to the type of course, the disease is:
- Latent. It is practically asymptomatic.
- With frequent relapses (more than 2 attacks per year).
- With rare relapses (1 attack).
The following forms are also found:
- Easy.
- Average.
- Heavy.
- Complicated.
Symptoms
one of the symptoms is discomfort in the right side
Latent and chronic forms of the disease are more common in children. With latent, there are no characteristic signs. The child often has headaches, gets tired quickly, sleeps poorly, and has a decreased appetite. Such children are distinguished by pale skin and bruises under the eyes.
The chronic form is expressed in the following symptoms:
- Nausea, bitter belching.
- Flatulence.
- Diarrhea or constipation.
- Loss of weight, appetite.
- Periodic dull pain in the right side.
Exacerbation of chronic cholecystitis occurs in the following cases:
- Eating disorder.
- ARVI.
- Stressful situation.
During an exacerbation, the child experiences the following symptoms:
- Fever.
- Attacks of nausea and vomiting.
- Sharp pain in the right hypochondrium, radiating to the scapula.
- The pain gets worse after eating or exercising.
- Tense abdominal wall.
- Pale skin, dry mouth.
- Painful attacks can last from several hours to several days.
Cholelithiasis in children - issues of choosing therapeutic tactics
AND
Herringbone disease (HSD) in childhood is no longer a casuistry. In this connection, the question arises for pediatricians: “Which treatment method should be preferred? How can we prevent the progression of the disease?” Despite the vast experience accumulated by therapists and gastroenterologists in the field of studying cholelithiasis, in pediatrics the issues of pharmacotherapy of cholelithiasis are at the stage of study, since it is not possible to extrapolate the data accumulated by interns to pediatrics; one should take into account the anatomical and physiological characteristics of children; take into account the formation and chemical composition of gallstones. Modern advances in surgical and endoscopic technology make it possible to revise treatment tactics in children with cholelithiasis.
Gallstone disease in children is a hereditarily determined disease of the liver and biliary tract, which is based on a violation of the processes of bile formation and bile excretion, accompanied by chronic inflammation with a progressive course, the natural outcome of which is sclerosis and dystrophy of the gallbladder.
Treatment tactics
in children with cholelithiasis currently includes two diametrically opposed approaches. Some authors, when stones are detected in the gallbladder, suggest surgical intervention, others adhere to the so-called wait-and-see approach, recommending conservative treatment. Both points of view have a number of advantages and disadvantages. On the one hand, removing the gallbladder, which acts as a reservoir for storing bile, allows you to get rid of the shock organ. On the other hand, even with a well-performed surgical intervention, there is a possible risk of intra- and postoperative complications, which is of no small importance [2,4,5,7].
The possibility of conservative treatment of cholelithiasis looks quite attractive, when the current level of the pharmaceutical industry offers such a promising effect from the use of drugs that dissolve gallstones. These include drugs containing chenodeoxycholic acid (Chenofalk) and ursodeoxycholic acid (Ursofalk). However, their use in children is limited by several factors, including the special mechanism of stone formation, the age of the child, the high incidence of anomalies in the development of the biliary tract, and the characteristics of the chemical composition of gallstones [1,6,8].
Features of the formation of gallstones in childhood
In children, bilirubin stones are more often detected, and only in puberty and adolescence does cholesterol lithiasis begin to predominate (Table 1).
In addition, the division into cholesterol and bilirubin stones in children is arbitrary - stones mixed in chemical composition are more common. This fact indicates that children are not characterized by a homogeneous type of nucleation, where stone formation is based on the mechanism of impaired cholesterologenesis (Fig. 1.). For the formation of bilirubin and mixed gallstones, additional factors (promoters) are required, which play the role of stone formation triggers. Three factors play a leading role in the genesis of stone formation in children: inheritance of specific antigens according to the HLA system (B12 and B18), the presence of anomalies in the development of the biliary tract and an aseptic inflammatory process in the wall of the gallbladder. All these three factors are interdependent and are accompanied by a violation of lipid peroxidation, the accumulation of oxygen free radicals, causing a cascade of pathophysiological processes and biochemical disorders, the natural outcome of which is not only the formation of gallstones, but also progressive, continuously relapsing inflammation of the gallbladder wall. The process becomes irreversible (Fig. 2).
Rice. 1. Pathogenesis of cholesterol lithiasis BA - bile acids; Gallbladder - gallbladder; CS - cholesterol
Rice. 2. Pathogenesis of mixed bilirubin gallstones GB - gallbladder; LPO—lipid peroxidation; CS - cholesterol; PL - phospholipids
Obviously, these are the reasons for the low efficiency of gallstone dissolution in childhood.
According to our own data, even in the presence of a single small-sized cholesterol stone, preserved gallbladder function, and complete patency of the bile ducts, dissolution can be achieved in no more than 5% of children. In addition, within two years after the end of therapy, stones recur again. In this regard, conservative therapy
in children suffering from cholelithiasis can be carried out in the following cases:
1. Children who have contraindications to surgical treatment due to the presence of severe concomitant diseases, where the risk of surgical intervention exceeds the effectiveness of treatment (children with severe congenital heart defects, lung defects, hemolytic anemia, diseases of the endocrine system, etc.);
2. Before and after planned surgical intervention for cholelithiasis;
3. Children with sediment in the gallbladder.
In all cases, conservative therapy begins with the provision of general routine measures. In case of exacerbation of cholelithiasis, manifested by an attack of “acute abdomen”; suspicion of obstructive jaundice - the appearance of dark urine the color of “beer” and acholic stools; in case of biliary colic, hospitalization of the patient is necessary.
During the period of remission, children do not show any complaints. Nevertheless, conditions should be created for them to maintain an optimal daily routine with limitation and sometimes elimination of physical activity. This is due to the fact that when running, jumping, or sudden movements, stones may move in the bile ducts, which may result in stone obstruction. However, physical inactivity is also considered as one of the unfavorable factors contributing to stone formation.
Dietary activities
for cholelithiasis, they are aimed at mechanical and chemical sparing of the digestive tract, preventing the cholekinetic effect of food. Table No. 5 according to Pevzner is prescribed, to which dietary fiber is added: vegetables, fruits, wheat bran, etc. They bind bile acids in the intestines, which promotes their synthesis in the liver. When clinical signs appear, there is a need to use pharmacological agents.
The choice of medications depends on the nature of the associated disorders. If they are associated with biliary dyskinesia, then the prescription of antispasmodics is usually appropriate. This not only relieves clinical symptoms, but also prevents conditions conducive to the migration of stones. More often, belladonna extract is prescribed in combination with drotaverine. It should be remembered that the use of metamizole is not always effective. If a painful attack is caused by a spasm of the sphincter of Oddi, then narcotic analgesics such as promedol are more effective. However, morphine should not be used, as it may, on the contrary, lead to increased pain. Peripheral vasodilators such as nitroxoline are effective for severe pain; sometimes it is enough to put validol under the tongue.
The practice of prescribing choleretic drugs for cholelithiasis lacks clear scientific justification and often does more harm than good. This applies to drugs not only with kinetic, but also with choleretic activity. Thus, the prescription of choleretics is contraindicated in the presence of stones in the common bile duct and any narrowing of it, which, unfortunately, doctors do not always take into account. The exception here is drugs such as rovachol, rovatin, enatin, olimethin, containing vegetable oils. Their positive effect is associated not so much with choleretic, but with antispasmodic and anti-inflammatory effects. There is also evidence that monoterpenes enhance the effect of agents that cause the dissolution of gallstones. It is recommended to combine their use with litholytic therapy, and after successful litholysis they are used for a long time for prophylactic purposes.
A great achievement in recent years is the inclusion in the treatment of patients of quite active agents that promote the dissolution (litholysis) of cholesterol gallstones. For this purpose, litholytic agents containing chenodeoxycholic acid - Henofalk and ursodeoxycholic acid - Ursofalk are used.
Currently, in children, preference is given to products containing ursodeoxycholic acid. They are more effective and have virtually no toxic effects. The mechanism of action of ursodeocholic acid is shown in the figure (Fig. 3).
Rice.
3. Action of ursodeoxycholic acid Ursofalk
, the active substance of which is ursodeoxycholic acid (UDCA), suppresses the reabsorption of hepatotoxic endogenous bile acids in the small intestine. Replaces them in the pool with non-toxic ursodeoxycholic acid, reduces the cytotoxic effect of aggressive lipophilic bile acids, and reduces the saturation of bile with cholesterol. Causes partial or complete dissolution of gallstones, has a choleretic effect and is practically free of side effects. Prescribed 10 mg per kg body weight per day. The course of treatment is 24 months. continuous use of the drug. Daily doses of the drug are presented in Table 2. Dissolution of gallstones is a long process that requires especially conscientious attention of sick children and their parents. It is this reason that often underlies unsuccessful treatment. The effectiveness increases significantly if Ursofalk is taken not 2-3 times, but once a day - at night, when cholesterol synthesis increases (Table 3). If after 12 months. There is no reduction in the size of gallstones, treatment is stopped. In addition to this therapy, a mixture of terpenes is added, especially for stone formation in the common bile duct. However, terpenes are less effective for stones located in the gallbladder. To flush out small stones from the bile ducts, it is recommended to use dehydrocholic acid. It stimulates the formation of liquid bile containing a lot of water.
Litholytic therapy must be combined with hepatoprotectors of plant origin
. To avoid polypharmacy, preference should be given to drugs with combined action.
One of these drugs is Hepatofalk Planta
, containing: flavonoid silibinin, which has hepatoprotective and antitoxic effects; alkaloid chelidonine – choleretic and antispasmodic effects; curcumin, which has an anti-inflammatory effect. A contraindication to its use for cholelithiasis can only be complete obstruction of the biliary tract.
In children with cholelithiasis, the use of medicinal preparations and herbs should be avoided, since they all have a powerful choleretic effect. This may entail increased motor function of the bile ducts with the development of obstruction of the bile ducts by the stone. An emerging attack of biliary colic leads to the need for emergency surgery. Therefore, herbal medicine should be actively prescribed to children after surgery in order to prevent recurrence of stone formation,
After successful dissolution of gallstones, their reappearance may occur. These relapses are the result of metabolic disturbances that persist after drug discontinuation. In this regard, long-term treatment with small doses of UDCA is recommended, which leads to a marked decrease in the lithogenic index of bile and the prevention of recurrent stone formation.
Physiotherapy
Physiotherapy for cholelithiasis should be aimed at improving the outflow of bile and restoring impaired body functions involved in the process, increasing the overall reactivity of the child’s body. Paraffin and azokerite applications and inductothermy to the liver area are prescribed. There are 8–15 procedures per course. You can use magnesium electrophoresis, as well as a 1% solution of papaverine hydrochloride, 0.2% solution of platiphylline hydrotartrate. Inductothermy is indicated. However, you should not prescribe tonic procedures - sinusoidally modulated currents. It is useful to use fresh or pine baths at a temperature of 37–37.5C for 7–12 minutes, every other day. Course 10–12 baths.
Sanatorium treatment at the resorts: Zheleznovodsk, Essentuki, Goryachiy Klyuch is important.
Surgical methods of treatment
Surgical methods for treating cholelithiasis are still alternative. They can be divided into two groups: 1) gentle, which are endoscopic interventions (laparoscopic, transpapillary and laparocentesis operations); 2) operations requiring standard laparotomy [1,2,6,7].
In children, 2 types of laparoscopic operations are used - laparoscopic cholelithotomy, when the stone is removed from the gallbladder and the gallbladder is preserved [5]; and cholecystectomy - in which the gallbladder is removed along with the stones [7,21,34,35]. Follow-up observations indicate that good results are observed in children operated on before the onset of severe symptoms of cholelithiasis. The optimal method for surgical treatment is to implement the principle of “operation for cholelithiasis before complications occur.”
Among the surgical methods of treating cholelithiasis, laparoscopic cholelithotomy, first performed by I.D., deserves great attention. Prudkov (1968). To perform it, a number of conditions must be present: a mobile and easily removable gallbladder, the thickness of the anterior abdominal wall is no more than 3 cm, the location of the gallbladder is below the costal arch. However, removal of stones from the gallbladder does not exclude relapses of stone formation, which, according to our data, amount to up to 34% during the first 6 months after surgery.
Obviously, one should agree with the opinion of most authors that the gallbladder is nothing more than a reservoir for storing bile, and is not dangerous only as long as its motor function is preserved and there is no inflammation in it. Therefore, any detection of a stone in the gallbladder (asymptomatic or painful) should be considered as a reason for planned, gentle surgical intervention, because, as Mayo said: “A safe stone is a myth. It is always fraught with danger, which can await the patient at the most unexpected period and can be accompanied by a wide variety of complications.” These patterns were confirmed by observation of children in follow-up. Studies of the morphological structure of the gallbladder in the children we observed revealed the presence of an inflammatory process in it in all those operated on. It was noteworthy that the inflammation tended to be recurrent with the subsequent development of dystrophic and sclerotic processes both in the lamina propria of the gallbladder mucosa and in the muscular layer (Fig. 4). Such morphological changes were detected both in children with the classic picture of biliary colic, and in cases of the presence of asymptomatic silent gallstones. This confirms the idea that asymptomatic stone carriage does not guarantee a favorable course of cholelithiasis. In children, obviously, we should not talk about asymptomatic gallstones, but about the latent course of cholelithiasis, which sooner or later manifests itself in a painful form, leading to the need for emergency surgical intervention.
Rice. 4. Intermuscular sclerosis of the gallbladder wall. GE staining, magnification 400
When stones are localized only in the gallbladder, cholecystectomy leads to a permanent cure for cholelithiasis. Obviously, the removal of the shock organ, the functional and compensatory capabilities of the child’s body lead to the normalization of the rhythm of bile secretion and bile formation, which, in turn, makes it possible to restore both the functional state of the liver and normalize the digestive processes. Therefore, laparoscopic cholecystectomy, performed routinely in the early stages of the disease, should be considered pathogenetically justified.
The results of the studies made it possible to outline ways of therapeutic correction of cholelithiasis in children. The algorithm of therapeutic tactics for cholelithiasis in children is presented in Figure 5.
Rice.
5. Therapeutic approaches to identifying gallstones in children (UDCA - Ursofalk; GF - Hepatofalk Planta) Literature:
1. Bairov G.A., Ergashev N.Sh. Diagnosis and treatment of cholelithiasis in children // Clinical surgery. – 1989. – No. 6. – P. 45–47.
2. Blinov V.Yu. Laparoscopic cholecystolithotomy and transfisural endoscopic sanitation of the gallbladder as a method of treating acute calculous cholecystitis in patients with a high degree of surgical risk. // Diss. Ph.D. honey. Sciences. – M. – 1990. – P. 123.
3. Gallinger Yu.I., Timoshin A.D., Tsatsanidi A.K. Laparoscopic cholecystectomy.//Surgery. – 1993. – No. 6. – P. 34–39.
4. Zaprudnov A.M., Kharitonova L.A. Treatment of children with gallstones. disease (lecture) //Ros. Perinatol Bulletin. and Pediatrics, 2000, No. 2
5. Kaluzhskikh V.V. Long-term results of organ-preserving surgery for chronic calculous cholecystitis.//Surgery.– 1994.– No. 1. pp. 18–20.
6. Karey M. Pathogenesis of cholelithiasis. // Falk symposium “New directions in hepatology”. – St. Petersburg, 1996. – P. 23–24.
7. Lutsevich O.3. Laparoscopic cholecystectomy.//M. – 1993. – P. 57–64.
8. Maksimov V.A., Chernyshev A.L., Tarasov K.M. and others. Modern non-surgical methods of treating cholelithiasis // Clinical pharmacology and clinical medicine. – 1996. – pp. 16–20.
Complications
With cholecystitis, adhesions may occur
Cholecystitis in children leads to serious complications in a short time. The baby may develop consequences such as:
- Pancreatitis.
- Adhesions in the gallbladder.
- Transition of inflammation to purulent.
- Abscess development.
- Organ rupture and peritonitis.
- Entry of bacterial flora into the bloodstream and subsequent sepsis.
All this is very dangerous, so it is important to prevent or respond to complications in a timely manner. After all, it can even lead to death.
Diagnostics
The acute form is usually diagnosed by external signs. The most difficult thing to detect is the latent course, since there are no characteristic signs. To make a diagnosis, the following studies are prescribed:
- Ultrasound. A simple and informative method that allows you to detect changes in the organ.
- X-ray. Prescribed to assess wall thickness.
- Blood chemistry. Pay attention to the following indicators: alkaline phosphatase, transminase.
- FGDS. Necessary to confirm or exclude gastritis or ulcers.
- Blood test for parasites.
- Duodenal sounding. Examines the composition of bile and bladder motility.
Diagnosis of cholecystitis
The initial stage of diagnosis is an examination of the child by a doctor, as well as a conversation with the parents and the child, during which the doctor learns all the necessary anamnestic data, determines the main complaints, as well as their nature and time when they arose. Then the specialist conducts a thorough physical examination, during which the child can identify characteristic symptoms that are determined by diseases of the gallbladder - the so-called cystic symptoms. After the examination and analysis of the medical history, the doctor refers the child for additional laboratory and instrumental studies.
Laboratory diagnostic methods include:
- Carrying out general clinical tests (blood, urine). A general blood test shows an increase in leukocytes and an increase in the erythrocyte sedimentation rate (ESR), which indicates the presence of an inflammatory process in the child’s body.
- Blood biochemistry with determination of liver tests, glucose and other indicators necessary for diagnosis.
- Coprogram.
- If a child is suspected of having viral hepatitis, a hepatitis test is performed.
It is also extremely important for diagnosis to conduct a number of instrumental studies:
- Ultrasound of the abdominal organs makes it possible to assess the condition and size of the gallbladder, determine the presence of stones, and wall thickness.
- X-ray contrast examination of the gallbladder (cholecystocholangiography) allows you to evaluate the dynamics of the biliary system, as well as detect disorders and identify gallstones.
- Duodenal intubation, in which three portions of bile are obtained, followed by microscopic and bacteriological examination.
- If indicated, CT, MRI, EGDS (esophagogastroduodenoscopy) are used.
Treatment
Surgical treatment of cholecystitis in children is carried out in exceptional cases: large stones, blockage of the ducts. In this case, there is a danger to the health and life of the baby.
In other cases, conservative treatment is used, which includes:
- Drug therapy.
- Herbal treatment.
- Diet.
Watch a video about the surgical treatment of cholecystitis in children:
Drug therapy
If cholecystitis worsens, the child requires bed rest. If his condition is satisfactory, then the medications can be taken at home. In severe cases, hospitalization is necessary. The following groups of drugs are prescribed for treatment:
| Antispasmodics (No-shpa, Drotaverine) | They relax smooth muscles and relieve pain. |
| Antibiotics of the macrolide or cephalosporin group (Cetriaxon, Tsiprolet) | Necessary to get rid of bacterial microflora. |
| Anthelmintics (Nemazol, Furozalidone). | Remove worms and parasites. |
| Choleretic (decoction of corn silk, Olahol). | They promote the outflow of bile, but are prohibited in the calculous form of the disease. |
| Hepatoprotectors (Essentiale, Esliver Forte) | Restore damaged liver cells, protect the liver from the influence of microorganisms. |
| Sedatives (Novopassit, Tenoten for children) | Prescribed if the child does not sleep well or is worried. |
Phytotherapy
Herbal treatment is part of complex therapy. When the acute period is over, herbal medicine is continued until complete recovery. Effective means are:
- Chamomile and immortelle. Brew two tablespoons of the mixture with boiling water (500 ml), cool, and take 50 ml 2 times a day.
- 20 grams of calendula flowers are poured with boiling water, left in a thermos for 8 hours, and drunk 14 glasses 2 times a day before meals.
- Mix elecampane, string, and mint in equal proportions. A spoonful of the mixture is steamed with boiling water and cooled. Take 50 ml three times a day before meals.
The following traditional medicines have proven themselves to be effective:
- Red rowan juice. Take 30-50 ml before meals up to three times a day. Can be sweetened with honey.
- A mixture of salt and lemon. The juice of one fruit is diluted with a glass of warm water and a spoonful of salt is added. Drink a glass per day, dividing it into equal portions.
Diet
Nutrition rules
Diet is the main component of cholecystitis treatment. Without normalizing nutrition, it is impossible to get rid of pathology. During an exacerbation, doctors even recommend fasting for 24 hours. Then they move to table No. 5.
It involves the exclusion of the following products:
- Fatty, fried, salty, spicy, smoked.
- Fast food, soda, chips.
- Chocolate, sweets.
- Sweet baked goods.
- Fatty meat and fish.
- Fatty dairy products.
- Nuts, mushrooms.
- Store-bought sauces, hot spices.
- Sour berries, fruits.
- Bobovykh.
- Vegetables with a spicy taste: radish, radish, onion, garlic.
The baby's diet consists of the following products:
- Lean meat, fish.
- Low-fat dairy products.
- Dried bread.
- Stewed vegetables.
- Vegetable soups.
- Porridge on the water.
- Protein omelettes.
Sample menu for the week:
Monday
| Breakfast | Millet porridge |
| Lunch | Yogurt |
| Dinner | Buckwheat, rabbit meatball |
| Afternoon snack | Pumpkin casserole with cottage cheese |
| Dinner | Mashed potatoes, tomato |
Tuesday
| Breakfast | Cottage cheese casserole |
| Lunch | Milk pudding |
| Dinner | Noodle soup with chicken broth |
| Afternoon snack | Syrniki |
| Dinner | Chicken meatball, steamed zucchini |
Wednesday
| Breakfast | Cottage cheese |
| Lunch | Rice balls |
| Dinner | Steamed chicken cutlet, mashed potatoes |
| Afternoon snack | Yogurt |
| Dinner | Pasta with cheese |
Thursday
| Breakfast | Rice porridge |
| Lunch | Fruit salad |
| Dinner | Turkey pasta |
| Afternoon snack | Rice pudding |
| Dinner | Vegetable casserole |
Friday
| Breakfast | Omelette |
| Lunch | Sweet fruit |
| Dinner | Fish soup |
| Afternoon snack | Banana |
| Dinner | Rice with turkey |
Saturday
| Breakfast | Syrniki |
| Lunch | Milk with cookies |
| Dinner | Vegetable stew with chicken |
| Afternoon snack | Fruit salad |
| Dinner | Stewed potatoes |
Sunday
| Breakfast | Oatmeal porridge |
| Lunch | Baked apple |
| Dinner | Pumpkin puree soup |
| Afternoon snack | Dried fruit compote, croutons |
| Dinner | Boiled fish, stewed vegetables |
Treatment methods for cholecystitis
The treatment tactics for this pathology primarily depend on whether one is dealing with acute or chronic cholecystitis.
In the chronic form, children are prescribed a special diet and provided with bed rest. Drug treatment consists of prescribing antibacterial drugs, anti-inflammatory drugs, and antispasmodics. Therapy also includes drugs that affect bile formation and excretion, and detoxification therapy is prescribed.
In case of acute cholecystitis, the child must be hospitalized in a surgical hospital. In the presence of such severe forms as phlegmonous or gangrenous cholecystitis, emergency surgical intervention is required. After the operation, children are prescribed medication and diet.
Clinical guidelines
The Ministry of Health has developed a clinical protocol for the treatment of cholecystitis. In addition to the main treatment, the following conditions must be met:
- Observation of the child for 2 years after treatment.
- Testing and ultrasound twice a year.
- Elimination of provoking factors.
- Spa treatment.
Treatment is considered successful if there are no exacerbations for 2 years, the motor functions of the gallbladder are restored, and there are no signs of inflammation and dyskinesia.
Consequences of cholecystitis
If you seek medical help in a timely manner, the prognosis for cholecystitis is favorable. If the symptoms of the disease are ignored for a long time, the following complications may develop:
- spread of inflammation with damage to the bile ducts (the occurrence of acute cholangitis);
- perforation, which occurs with purulent inflammation of the gallbladder with the development of peritonitis;
- intestinal obstruction;
- sepsis;
- After removal of the gallbladder, postcholecystectomy syndrome may develop.
Prognosis and prevention
The child should have moderate physical activity and a healthy diet
Prevention of childhood cholecystitis consists of the following measures:
- Compliance with diet.
- Elimination of junk food.
- Normalization of physical and emotional stress.
- Timely treatment of chronic diseases and parasitic infections.
If the disease is diagnosed in a timely manner and treatment is started, the prognosis is favorable. If the recommendations are not followed, the disease becomes chronic or complicated, and there is a risk of complications and even death.
Prevention
To prevent the development or exacerbation of chronic cholecystitis, it is necessary to ensure that the child has a proper diet, balanced in nutrients and calorie content in accordance with age standards, and adherence to a meal schedule.
It is equally important to motivate children to lead an active lifestyle and engage in regular physical exercise. Any gastrointestinal disease and detected helminthiasis must be treated promptly and correctly.
As prescribed by a doctor for chronic cholecystitis, to prevent exacerbation, preventive courses are carried out 2-3 times a year: physiotherapeutic procedures (electrophoresis with nicotinic acid, magnesium sulfate, paraffin applications), choleretic agents (depending on the type of motility of the gallbladder) and the use of mineral waters (Essentuki No. 17 and No. 4, Mirgorodskaya, Naftusya, Slavyanskaya, etc.). They are taken warm from 1/3 to 1 cup (the dose depends on the age of the child) three times a day.