Anal sphincter and its structure
Anal sphincter spasm causes a lot of discomfort
The main function of the anal sphincter is to control the release of what is contained in the intestines. The sphincter consists of two parts:
- Internal sphincter
- External sphincter
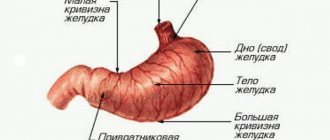
If we talk about the internal sphincter, then it is a kind of ring structure that consists of smooth muscles. This system surrounds the output channel. The length of the internal sphincter is about twenty-five to thirty millimeters, and the width is five millimeters.
This part of the sphincter is different in that its action does not depend on the person’s consciousness, in other words, muscle contraction occurs on its own. In its normal state, the muscle is always contracted, and relaxation occurs only in the process of irritation of the rectum.
The internal sphincter has an important function, namely, it is designed to keep all the contents of the intestines inside, and it also does not allow gases to escape arbitrarily. This function contains several levels:
- First of all, this is the so-called intramural level
- Then comes the spinal level
- The third level is suprasegmental, which is located in certain parts of the brain
The first two levels can operate thanks to the autonomic system. Special fibers allow the muscles of the internal sphincter to always be in a contracted form and work to slightly inhibit and weaken the motor activity of the rectum itself. The external sphincter is also presented in the form of a ring system, but in this case the system consists of striated muscles. These muscles, unlike the internal sphincter, are controlled by the human consciousness. The outer part of the muscles is formed by three main layers:
- Muscles that are located under the skin and look like a ring system
- The second layer is the superficial muscles. It is an elliptical muscle that attaches to the tailbone.
- And the final layer is the so-called deep muscle, which is closely associated with the puborectal muscles.
The length of this part is eight to ten centimeters, the thickness is approximately two and a half centimeters.
There are special stretch receptors in the outer part of the muscles. Thanks to such receptors, a person is able to control the output of feces, its quantity and consistency.
Anal sphincter insufficiency
Anal sphincter insufficiency is manifested by a complete or partial violation of the voluntary retention of rectal contents (gases or feces). It is often combined with a related symptom - the inability to control the act of urination, since the nervous regulation of both processes occurs with the participation of nerve centers that are similar in nature. Fecal incontinence is most often not an independent disease, but only a manifestation of other pathologies. This pathology does not threaten the patient’s life, but significantly worsens the quality of life, as it creates many problems for the patient and the people around him. You can encounter this problem at any age.
As a rule, anal sphincter insufficiency occurs as a result of 2 groups of reasons:
- Group 1: against the background of diseases related to the digestive tract and excretory system (rectal prolapse, anal injuries, accumulation of large amounts of hard feces in the rectum).
- Group 2: against the background of other diseases (birth injuries of the pelvis, anal tumors, neurological consequences of severe forms of diabetes, etc.)
In practice, fecal incontinence is usually divided according to severity:
- I degree – manifests itself in gas incontinence.
- II degree – characterized by incontinence of unformed feces.
- III degree – is expressed in the patient’s inability to retain dense stool.
Diagnosis of fecal incontinence is based on: - assessment of the patient’s complaints; — examining the patient with a digital examination; - sigmoidoscopy - examination of the rectum using an endoscopic apparatus; — physiological research methods in order to clarify the nature of changes and the severity of weakness of the pelvic floor muscles: sphincterometry, electromyography, anorectal manometry. - electromyography of the pelvic floor muscles and rectal muscles to determine the correct functioning of the nerves that control these muscles.
The issue of the scope of diagnostic examinations and therapy for fecal incontinence is very important and is prescribed individually after a visit to the doctor.
Treatment depends on the cause that led to this pathology, the degree of dysfunction of the pelvic floor muscles, the patient’s condition and his age. Surgical and conservative methods of treating fecal incontinence are used.
Conservative methods include:
- diet therapy;
- normalization of stool consistency;
- a set of physical exercises aimed at strengthening the pelvic floor muscles.
- instrumental methods of treatment - the biofeedback method (biofeedback, BFB) - a modern, highly effective non-drug method that uses the combined effects of training methods aimed at increasing the tone of the pelvic floor muscles. During the sessions, patients are trained to control changes in the condition of the pelvic floor muscles.
Electrical stimulation is also used, which actively affects the obturator apparatus of the rectum and increases tonic muscle tension. The need and method of surgical correction are decided together with the proctologist surgeon after further examination of the patient.
Do not delay your visit to the specialists of our Center. This will help to diagnose this condition in a timely manner and choose the right treatment tactics. Doctors of the State Budgetary Healthcare Institution MKSC named after A.S. Loginova DZM are always ready to help you.
Development, causes and symptoms
Pain may occur due to irritation and inflammation of the mucous membrane. Most often, pain of this kind occurs in patients with anal fissure, which has existed for quite a long time. The pain subsequently develops into muscle spasm. In addition, in this case, muscle spasm creates a vicious circle: feces, which inevitably fall into the crack, cause pain and even greater inflammation, which leads to the development of spasms, which in turn cause increased pain and the appearance of symptoms.
It should be said that the most common cause of pain is various types of injuries. Often, the culprit of the disease is hemorrhoids, the hemorrhoidal nodes of which are located inside. In addition, the cause may be a certain kind of purulent inflammation that develops near the rectum.
The most important symptom when spasms occur is a sharp sensation in the anus. They appear during the process of defecation, and can also intensify significantly throughout the entire process. Other symptoms that appear during spasms cannot be called specific to this disease. Very often such diseases are accompanied by bleeding. However, in this case, the spasm helps to compress the blood vessels, thereby accelerating the cessation of bleeding and significantly reducing it.
Also, constant severe pain during defecation forces the patient to postpone this process as long as possible, which ultimately leads to the development of constipation.
“THE SITE IS UNDER RECONSTRUCTION WE APOLOGIZE FOR THE TEMPORARY INCONVENIENCE”
Anal sphincter insufficiency is a partial or complete violation of the voluntary retention of colon contents.Normally, the rectal closure apparatus is capable of retaining solid, liquid and gaseous intestinal contents not only in various body positions, but also during exercise, coughing, sneezing, etc.
According to the etiological factor, there are the following types of incontinence: post-traumatic, postpartum, functional and congenital.
The most common cause of incontinence is injury to the obturator apparatus of the rectum, most often associated with obstetric or surgical trauma. Then in frequency follows functional insufficiency of the anal sphincter, caused by neuro-reflex disorders and pronounced changes in muscle structures. The cause of these disorders is most often various diseases of the rectum and anal canal, such as rectal prolapse, hemorrhoids with prolapse of internal hemorrhoids, as well as various inflammatory diseases of the colon. In third place are various malformations of the rectum and anal canal, which are complicated by insufficiency of the anal sphincter.
There are three degrees of clinical manifestations of sphincter insufficiency: at grade 1, patients cannot retain gases; at grade 2, liquid feces incontinence is added to this symptom; at grade 3, patients cannot retain all components of intestinal contents (gases, liquid and solid feces).
Diagnosis of anal sphincter insufficiency is based on the patient’s complaints, examination of the patient on a gynecological chair with digital examination, anoscopy and sigmoidoscopy. Instrumental methods for examining such patients include physiological research methods: sphincterometry, electromyography, manometry and profilometry.
In addition, patients undergo X-ray examinations, including proctography and irrigoscopy with double contrast. Ultrasound examination with a rectal probe, examination of the intestinal flora for dysbacteriosis are of great importance in diagnosis; in women, a bacterioscopic examination of the vaginal flora is mandatory for the degree of purity and the presence of sexually transmitted diseases (especially in case of postpartum insufficiency).
Patients with functional sphincter insufficiency of 1-2 degrees, which developed as a result of rectal prolapse or prolapse of internal hemorrhoids, after surgical treatment of the underlying disease (rectopexy; hemorrhoidectomy, etc.) are shown conservative therapy as the main type of treatment for anal sphincter insufficiency. In addition, patients with 1-2 degrees of insufficiency with organic damage to the sphincter with a linear defect over no more than a quarter of the circumference of the anal canal with no deformation of the walls of the anal canal are subject to conservative treatment. Conservative treatment includes electrical stimulation, physical therapy, and drug therapy.
The indication for surgical treatment is a violation of the anatomical structure of the anal sphincter, as well as 2-3 degrees of insufficiency that has developed as a result of other diseases of the rectum and anal canal (rectal prolapse, hemorrhoids, etc.). For patients with anal sphincter insufficiency, grade 1-2. with a sphincter defect extending up to a quarter of the circumference of the anal canal, an operation is performed - sphincteroplasty.
With 2-3 degrees of anal sphincter insufficiency, the presence of a defect from 1/4 to 1/3 of its circumference, an operation in the scope of sphincterolevatoplasty is performed.
With 2-3 degrees of anal sphincter insufficiency, the presence of a defect from 1/3 to 1/2 of its circumference, sphincterogluteoplasty is performed (replacement of the sphincter defect with a short flap of the gluteus maximus muscle).
Patients whose sphincter defect is more than half the circumference of the anal canal or have a complete absence of the sphincter represent the most difficult group of patients to treat. For these patients, an artificial rectal apparatus is created from a long flap of one of the two gluteal muscles, and more recently from the tender thigh muscle (graciloplasty).
4.Treatment
As a rule, the therapeutic approach to the treatment of anal sphincter ruptures is complex, multi-vector. Almost always, medications are prescribed in the form of suppositories, ointments, baths, microenemas, etc.; physiotherapeutic procedures and exercise therapy; antiseptic hygiene and antibiotic prophylaxis; a special diet excluding spicy and other irritating foods. Sometimes novocaine blockades are used to relieve pain. In other cases, for example, with large ruptures, independently and/or against the background of conservative therapy, proctosurgical intervention is performed to eliminate the defect. The prognosis in the vast majority of cases is favorable (subject to the obligatory condition of seeking help and following all instructions received).
1.General information
Rupture of the rectal sphincter (anal sphincter, locking muscle) is an unpleasant phenomenon, often painful, causing severe hygienic and psychological discomfort, but it is by no means rare.
We are talking about mechanical damage to the orbicularis muscle, which, outside the act of defecation, should tightly block the anus. The term “sphincter rupture” is close in meaning to another common proctological pathology, anal fissure, and the shape of the rupture is most often linear, but these are still not identical concepts. Anal fissure is a chronic disease; this is a non-healing and/or recurrent ulceration, whereas a “rupture” is usually understood as a simultaneous, gross and precisely mechanical violation of integrity. However, such damage can easily lead to infection, inflammation and the formation of an anal fissure, fistula and many other complications.
A must read! Help with treatment and hospitalization!
2. Reasons
The most common risk factors and immediate causes of sphincter rupture are:
- complicated childbirth associated with exceeding the maximum permissible stress in the tissues of the perineum, vagina and rectum (as a rule, such ruptures are multiple in nature and are more often observed in first-time mothers);
- tendency to constipation, prolonged strained bowel movements and the formation of intestinal stones, the migration of which “towards the exit” can damage both the walls of the colon and the terminal sphincter;
- insertion of any solid objects into the rectum (regardless of their nature, purpose and circumstances of insertion into the anus - for example, an unsuccessful attempt to give yourself an enema, an accident, a fall, violence, a childish or pathological desire to experiment, etc.);
- sharp sudden spasm of the anal sphincter;
- an attempt to lift and/or hold a load that is obviously unbearable;
- anal sex.
Risk factors also include hereditary predisposition, physical inactivity, “sedentary” work and, in general, any other causes of dystrophic-degenerative processes in muscle tissue (smoking, sitting for many hours in front of the computer, hypovitaminosis, dietary imbalances, frequent alcohol consumption, age-related changes, etc.) .d.).
Visit our General Surgery page