the whole list
Peptic ulcer disease is a chronic disease that occurs with alternating periods of exacerbation and remission, the main symptom of which is the formation of a defect (ulcer) in the wall of the stomach and/or duodenum.
An ulcer is a defect in the mucous membrane that has a clear boundary. A superficial ulcer is called erosion. Peptic ulcer disease is detected in 5–10% of the adult population.
Depending on the location, ulcers are divided into gastric and duodenal (duodenum - duodenum).
The ratio of gastric and duodenal ulcers is approximately 1: 4. Young people have a lower incidence of gastric ulcers compared to duodenal ulcers (1: 13). Conversely, in middle-aged and elderly patients the frequency of gastric ulcers increases.
Along with peptic ulcer disease as an independent disease, it is now customary to distinguish secondary symptomatic ulcers of the stomach and duodenum that occur under the influence of stress, circulatory disorders, taking antipyretics, painkillers (acetylsalicylic acid, indomethacin, diclofenac, ibuprofen) and others.
Depending on the cause, there are:
- stress ulcers (for example, with myocardial infarction, widespread burns, after neurosurgery, etc.);
- drug-induced ulcers (taking non-steroidal anti-inflammatory drugs, hormones and other medications);
- endocrine ulcers (with Zollinger-Ellison syndrome, hyperparathyroidism);
- ulcers in certain diseases of internal organs (Crohn's disease, atherosclerosis of the branches of the abdominal aorta, etc.).
Causes of peptic ulcer
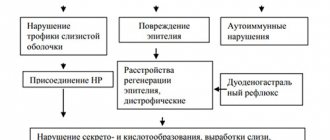
One of the main causes of peptic ulcer development is currently considered to be infection caused by the microorganism Helicobacter pylori (H. pylori). However, it should be noted that approximately more than half of the world's population is infected with H. pylori infection, and in many people this infection is asymptomatic; some of those infected develop chronic gastritis, atrophic gastritis, and stomach cancer. The effect of Helicobacter pylori on the gastric mucosa may depend on the state of the host’s immune system; the development of peptic ulcer disease depends on the presence of associated factors.
Factors contributing to the development of peptic ulcer disease (risk factors)
- Neuropsychic factor (stress).
- Smoking (smoking also impairs the healing of ulcers and increases the likelihood of their re-development - relapses; the degree of risk when smoking tobacco depends on the number of cigarettes smoked per day).
- Heredity.
- Violation of the regime and nature of nutrition.
- Alcohol abuse.
For the occurrence of a peptic ulcer, as a rule, it is not the isolated action of one of the listed factors that is necessary, but their combination. From a modern point of view, the development of peptic ulcer disease appears to be the result of an imbalance between the factors of “aggression” and the factors of “protection” of the mucous membrane of the stomach and duodenum. Factors of aggression (acid, gastroduodenal dyskinesia, Helicobacter pylori, etc.) prevail over protective factors (mucoproteins and bicarbonates of mucus, mechanisms for regulating the production of gastric juice, etc.).
Endoscopic stages of peptic ulcer
- open ulcer,
- scarring ulcer,
- stages of red scar, white scar.
Ulcer size
- small (less than 0.5 cm);
- medium (0.5–1 cm);
- large (1.1–3 cm);
- gigantic (more than 3 cm).
Treatment of the disease at the Yauza Clinical Hospital
Specialists of the gastroenterology department of the Yauza Clinical Hospital recommend dietary nutrition to patients with uncomplicated peptic ulcer disease and prescribe drug therapy, which includes:
- acid-lowering drugs;
- prokinetics;
- enveloping agents;
- enzymes.
If Helicobacter pylori bacteria are detected, antibacterial therapy is mandatory.
If stress is present, sedatives are added and psychotherapeutic treatment is indicated
In case of exacerbation of the disease, hospital treatment is recommended. If surgical treatment is necessary, the surgical method is selected depending on the course of the peptic ulcer, the location of the pathological focus and the nature of the complications.
The pharmacotherapy of concomitant diseases is adjusted - if possible, drugs that promote ulcer formation are replaced with safer analogues.
Clinical picture of peptic ulcer
The most consistent and important symptom of peptic ulcer disease is pain. Pain in peptic ulcer disease has a clearly defined rhythm (time of occurrence and connection with food intake), and seasonality of exacerbations.
Based on the time of occurrence and their connection with food intake, pain is distinguished between early and late, night and “hungry”. Early pain occurs 0.5–1 hour after eating, lasts 1.5–2 hours and decreases as gastric contents are evacuated. Such pain is more typical for gastric ulcer in the upper part.
Late pain appears 1.5–2 hours after eating, night pain occurs at night, and “hungry pain” occurs several hours after eating and stops after eating. Late, night and “hungry” pains are more typical for the localization of an ulcer in the antrum of the stomach or duodenal ulcer.
The nature and intensity of pain may vary (dull, aching, burning, cutting, cramping). The localization of pain in peptic ulcer disease is different and depends on the location of the ulcer: with an ulcer on the lesser curvature of the stomach, pain often occurs in the epigastric region, with duodenal ulcers - in the epigastric region to the right of the midline. With ulcers of the cardial part of the stomach, pain can be behind the sternum or in the heart area; in this case, it is important to differentiate peptic ulcer disease from angina pectoris or myocardial infarction. Pain often occurs after taking antacids, milk, food, and even after vomiting.
In addition to pain, the typical clinical picture of peptic ulcer disease includes various dyspeptic symptoms.
Heartburn is one of the early and frequent symptoms characteristic of peptic ulcer disease. Heartburn can occur at the same time after eating as pain. It often precedes the onset of pain, and subsequently is often combined with pain. These two symptoms are closely related, and some patients have difficulty distinguishing between them. In later stages of the disease, heartburn may disappear. But sometimes it can be the only subjective manifestation of a peptic ulcer.
Belching is a fairly common, but not specific symptom of peptic ulcer disease. The most typical belching is sour. The appearance of belching is associated with impaired evacuation of gastric contents due to prolonged spasm and severe inflammatory edema of the pylorus or duodenal bulb. It should also be remembered that belching is characteristic of a diaphragmatic hernia.
Nausea and vomiting are dyspeptic symptoms characteristic of exacerbation of peptic ulcer disease. Nausea is often accompanied by vomiting, although vomiting can occur without preceding nausea.
Vomiting in patients with peptic ulcer disease often has some specific features: firstly, it occurs at the height of pain, being, as it were, the culmination of pain; secondly, it brings significant relief. Vomit, as a rule, has an acidic reaction with an admixture of recently eaten food. Vomiting can also occur on an empty stomach.
Appetite in case of peptic ulcer is usually preserved or even increased (the so-called painful feeling of hunger). Decreased appetite is possible with severe pain syndrome; fear of eating may occur due to the possibility of pain occurring or increasing. Decreased appetite and fear of food can lead to significant weight loss for the patient.
Constipation is observed in half of patients with peptic ulcer disease, especially during exacerbation. Constipation in peptic ulcer disease is caused by a number of reasons: spastic contraction of the colon, a gentle diet, poor coarse fiber and the resulting lack of intestinal stimulation, limitation of physical activity, and the use of antacids (Almagel, etc.).
Symptoms depend on the location of the ulcer and the age of the patient . In some cases there may be no pain (painless ulcers). In these cases, ulcers are discovered when complications develop (ulcer bleeding, ulcer perforation - breakthrough of the ulcer wall into the abdominal cavity, penetration of the ulcer). Only about half of people with duodenal ulcers (duodenal ulcers) have typical symptoms. In children, the elderly, and patients taking certain medications, symptoms may be atypical or absent altogether.
Rehabilitation after surgery
Rehabilitation should include three main aspects:
- early patient activation;
- therapeutic and breathing exercises;
- special diet.
All this prevents complications and accelerates tissue restoration processes.
On the first day after surgery, passive and active movements of the legs are allowed. From the very first day you need to do breathing exercises. If there are no contraindications, you can get out of bed already on the 2-3rd day.
If recovery goes well, the stitches will be removed on the 8th day. Usually after 2 weeks the patient is already discharged from the hospital if there are no complications and rehabilitation is going well.
Complications of peptic ulcer
life-threatening complications develop with a peptic ulcer : penetration, perforation (perforation), bleeding and narrowing (stenosis) of the pyloroduodenal part of the stomach.
Ulcers are often complicated by bleeding, even if they did not cause pain. Symptoms of ulcer bleeding may include vomiting bright red blood or a red-brown mass of partially digested blood that resembles coffee grounds, and black, tarry stool. With very intense bleeding, scarlet blood may appear in the stool. Bleeding may be accompanied by weakness, dizziness, and loss of consciousness. The patient must be urgently hospitalized.
Ulcers of the duodenum and stomach can damage the wall of these organs through and through, forming an opening leading into the abdominal cavity. Pain occurs - sudden, intense and constant. It quickly spreads throughout the abdomen. Sometimes a person feels pain, which intensifies with deep breathing. Symptoms are less intense in older people, in people taking corticosteroids or in very seriously ill people. An increase in body temperature indicates the development of an infection in the abdominal cavity. If medical care is not provided, shock (a sharp drop in blood pressure) develops. If the ulcer perforates (perforates), surgery is required.
An ulcer can destroy the entire muscular wall of the stomach or duodenum and invade an adjacent organ, such as the liver or pancreas. This complication is called ulcer penetration .
Swelling of the inflamed tissue around the ulcer or scar from previous exacerbations of the disease can narrow the outlet of the stomach (pyloroduodenal region) or the lumen of the duodenum. With this type of obstruction, repeated vomiting often occurs, and large volumes of food eaten many hours before are released. There is a feeling of fullness in the stomach after eating, bloating and lack of appetite - the most common symptoms of obstruction. Over time, frequent vomiting leads to weight loss, dehydration, and imbalance of minerals in the body. Treatment of the ulcer will relieve the obstruction in most cases, but severe obstruction may require endoscopic or surgical intervention.
Treatment of gastric and duodenal ulcers should only be carried out under the supervision of the attending physician. The fact is that self-administration of various antacids and other drugs that reduce the acidity of gastric juice can alleviate the symptoms of the disease, but this improvement will only be short-term. Only adequate treatment prescribed by a gastroenterologist can lead to complete healing of ulcers.
Preventive actions
To avoid stomach ulcers, you need to follow some important measures. The most important advice is to follow a daily routine, eat right, and give up bad habits. It is important to remember about the quality of food and diet, which is also important for this pathology.
You must try not to be nervous and avoid stress. As soon as a person finds himself in an unpleasant situation, the stomach begins to work as actively as possible, produces more enzymes, and gastric juice becomes aggressive. Its concentration increases, causing gastric juice to damage the walls of the stomach. For this reason, important preventive measures include meditation, yoga, and taking care of your mental health.
It should be remembered that this pathology more often affects those who smoke. And all because the components of tobacco smoke, dissolving in saliva, negatively affect the gastric mucosa. This leads to suppression of local immunity, which causes a more aggressive effect of acid.
Diagnosis of peptic ulcer
The doctor may suspect the presence of ulcers in the stomach or duodenum if the patient has characteristic complaints. After examining and questioning the patient, the doctor will prescribe a series of studies to confirm or exclude the diagnosis of peptic ulcer.
Endoscopic examination of the stomach and duodenum - FEGDS (fibroesophagogastroduodenoscopy). In this study, the doctor inserts a thin, flexible instrument (fiber optic tube - endoscope) with a light source and a micro-camera at the end into the esophagus and further into the stomach and duodenum (12 pcs) of the patient.
The study is carried out to examine the internal surface of the gastrointestinal tract (to detect ulcers and determine their location, as well as to exclude complications: bleeding, perforation, penetration, stenosis). During the study, the doctor can take tissue samples (biopsies) from the stomach.
The obtained biopsies are examined in laboratory conditions to exclude a malignant disease (for gastric ulcers), detect Helciobacter pylori, and clarify the type of gastritis. An endoscope can also often be used to stop bleeding from an ulcer (cauterization of the ulcer).
X-ray examination . An overview image of the abdominal organs is performed if there is a suspicion of ulcer perforation (perforation of the wall of the stomach or duodenum), while an accumulation of free gas (air) coming from the gastrointestinal tract is determined in the abdominal cavity.
If a tumor, pyloric stenosis or 12 PC is suspected, an X-ray examination of the stomach and duodenum is performed after taking a barium suspension.
Tests to detect H. pylori infection. Currently, there are many methods for diagnosing H. pylori infection, including a urease breath test, determination of antibodies in the blood, PCR diagnostics for the presence of H. pylori in stool, and biopsy of the gastric mucosa for the presence of H. pylori.
Blood test . A complete blood count will not detect an ulcer, but may reveal anemia resulting from ulcer bleeding or an elevated white blood cell count as a sign of complications.
Main indications for surgery:
- ineffectiveness of drug treatment, that is, non-healing of the ulcer, two times a year or more - relapses of ulcerations, early relapses after taking medications;
- severe ulcerative pain that limits the ability to work and does not go away despite drug therapy;
- complicated ulcer – bleeding, perforation, narrowing of the pylorus.
Indications for gastrectomy:
- multiple ulcers, of which one is perforated and the other is bleeding;
- extensive callous gastric ulcers;
- simultaneously a stomach and duodenal ulcer.
The importance of early detection of symptoms
The disease does not always occur in an obvious form. In most patients it is hidden. This is especially true for children and the elderly, whose immune systems respond less well than healthy adults. Therefore, the effect of Helicobacter pylori cannot always be eliminated in time. A person should listen to his body, especially if he knows about the chronic course of peptic ulcer disease.
Even if your appetite decreases slightly and an aversion to food appears, it is better to be examined by a gastroenterologist. It includes gastroscopy, x-ray of the stomach, bacteriological examination for the presence of Helicobacter pylori infection.
It is mandatory to conduct general clinical studies, for example, OBC, OAM, biochemical test, coagulogram.
If the primary formation of symptoms or exacerbation of a chronic process is detected in a timely manner, a person avoids many complications that pose a danger to his life and health. If a patient is diagnosed with a chronic form of an ulcer, it is recommended to undergo laboratory tests every 3-6 months. X-rays and gastroscopy are used every year. This is how they monitor the quality of treatment and the extent of the spread of pathology.