Rectum
The rectum is a tube with muscular walls consisting of longitudinal and transverse layers, it is fixed in the pelvis by ligaments and has a length of about 15 cm. The rectum then passes through the rectosigmoid junction into the sigmoid colon. The rectosigmoid junction has the appearance of a bend of 70-120 degrees. For 10-15 cm from the anus, the rectum has practically no painful endings and does not contact the small intestine located in the abdomen. Due to these features, when performing sigmoidoscopy, discomfort occurs only when it is necessary to examine the rectosigmoid section and the final segment of the sigmoid colon and is caused by passage through the rectosigmoid junction and contact through the wall of the sigmoid colon with the small intestine, on the surface of which there are many pain receptors, while diagnosis of the rectum itself is practically painless.
Total mesorectal excision
The TME technique is the method of choice in the treatment of colorectal cancer, provided there is a free tumor margin. The rectum with the tumor is removed “as a single block” along with the mesorectum under visual control to the level of the anal canal using an acute method in the avascular zone. The native fascia remains intact. The outwardly located presacral layer of adipose tissue, the parietal fascia of the lateral walls of the pelvis, the prostate gland in men and the vagina in women along with the nerve plexuses are preserved intact. This minimizes the likelihood of incomplete tumor removal.
In the schematic image on the left, a tumor of the rectum with invasion into the perirectal tissue and changes in single lymph nodes. The resection margin is along the mesorectal fascia without signs of invasion, therefore TME can be performed. Note the upper edge of the anal canal (notched line - blue arrow).
On MR images, perirectal tissue has high signal intensity on T1 and T2 weighted images. The perirectal tissue is delimited by the mesorectal fascia, which is visible as a thin line with low MR signal intensity (red arrows).
The role of mesorectal fascia in TME planning. The shortest distance from the edge of the tumor or lymph nodes is called the circumferential resection margin (CRM/circular resection margin/proximal, distal and lateral resection margins). It is one of the main risk factors for local relapse. The involved lateral resection margin is a separate prognostic factor for overall and disease-free survival, a distance of >2 mm suggests that the mesorectal fascia is intact, 1-2 mm with possible invasion, and is involved in the process if this distance is ⩽1 mm.
The rectum is surrounded by pararectal tissue, delimited by mesorectal fascia, marked with red arrows. P - prostate V - seminal vesicles
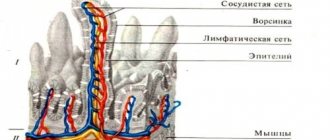
Anal canal
The anal canal is the terminal part of the rectum, it ends with the anus and has a pronounced muscular wall - the anal canal sphincter complex. This complex consists of external and internal sphincters, which are responsible for voluntary and involuntary retention of feces and gases. In the anal canal, the rectal mucosa transitions into the epithelium (anodermis) of the anal canal, which then passes into the skin of the perianal area. In the skin part of the anal canal there is a very large number of pain receptors, and on the mucous membrane they are practically absent. When an anal canal fissure develops, it is located on the skin part, its bottom is the subcutaneous/superficial portion of the sphincter (constituting no more than 1/10 of its total volume), and with mechanical irritation (bowel emptying), a pronounced spasm of this muscle develops, and intense pain syndrome. That is why performing a drug blockade or dosed sphincterotomy in the case of a fissure with pain that is not amenable to conservative treatment leads to its rapid healing.
Introduction
Paraproctitis - acute or chronic inflammation of the peri-rectal tissue - is a very common disease. In the structure of proctological diseases, it ranks fourth after hemorrhoids, anal fissures, and colitis. Among people with diseases of the rectum, patients with acute paraproctitis account for an average of 15.1%. Paraproctitis is more common in males, mainly in working age (from 20 to 50 years).
Mention of this suffering dates back to the era of Hippocrates, but the treatment of paraproctitis has its own characteristics and remains a difficult task even today.
Patients with acute paraproctitis often end up in hospitals on duty with general surgeons, so their competence in diagnosing and treating this pathology is extremely important.
In this publication, we have tried to present modern methods of diagnosis and treatment of paraproctitis in an accessible manner.
N-stage
The presence of N-stage is an important risk factor for the development of locoregional relapse. Unfortunately, MRI, like most other imaging modalities, has low sensitivity and specificity for detecting lymph node metastases. Lymph nodes with short axis dimensions > 5 mm, changes in shape, radiant contours and unclear boundaries or a heterogeneous structure are considered affected. However, not all affected lymph nodes meet these criteria. The TNM5 classification is more commonly used to determine the N stage. The N stages in TNM7 are similar to TNM5, but the N1 and N2 stages are more differentiated.
Even in T1 and T2 stages of the tumor process there is a significant risk of metastatic damage to the lymph nodes (see table).
The low sensitivity of use for assessing size alone may be explained by the fact that in colorectal cancer the presence of malignant changes even in small lymph nodes is widespread, up to 9% in nodes measuring 1-2 mm nodes and up to 17% in nodes measuring 2-5 mm (11). As shown in the table on the left, most changes are detected in lymph nodes measuring 1-5 mm. In order not to underestimate the stage, all visualized lymph nodes can be considered as malignant.
The image on the left shows an inferior ampullary rectal cancer with multiple lymph nodes in the perirectal tissue posterior to the ampulla. This has a huge impact on the patient's prognosis based on MRF+ and N+ status, so the patient will receive more aggressive treatment with neoadjuvant chemoradiotherapy.
It is important to pay attention to the lymph nodes of the posterior mesorectal tissue (arrow). These mesorectal lymph nodes are important because they can be the cause of local recurrences. If detected by MRI, radiation therapy and surgical planning will be tailored. On the left is a patient after TME with relapse in mesorectal tissue nodules (arrow). These mesorectal lymph nodes were not resected during standard TME surgery. The identification of malignant mesorectal lymph nodes at a minimum entails a more advanced surgical approach, since it is necessary to remove all tumor nodes or increase the dose of radiation therapy in the risk area.
Axial T2-weighted images on the left show two patients with rectal cancer. These examples illustrate the complexity of determining N-status. A small extramesorectal lymph node is identified on the far left. In the image on the right, numerous large mesorectal lymph nodes are visualized, and a lymph node with unclear boundaries is identified in the right parts of the extramesorectal tissue (red arrow). Although the lymph nodes of these patients had different characteristics in terms of size, borders, and heterogeneous appearance, they were all found to be malignant. Rectal cancer is characterized by metastatic lesions of small lymph nodes.
How to behave after surgery?
After the operation, you will remain in the hospital for 1 to 5 days, depending on the complexity of the operation. You will be prescribed, if necessary, antibacterial therapy and dressings with wound-healing ointments will be performed. After surgery, you may need to hold stool to allow the wound to heal.
Your doctor will teach you how to care for the wound, and it is extremely important to follow these recommendations strictly. One of the important recommendations is to irrigate the wound with a stream of water 3-4 times a day for the purpose of mechanical cleaning and periodic medical monitoring of proper healing in the direction “from the bottom of the wound.” After training, as a rule, you will be able to perform dressings yourself at home.
T3 MRF-
T3 tumors grow through all layers of the intestinal wall and penetrate into the perirectal fatty tissue. At this stage, it is important to determine whether the mesorectal fascia is involved or not. On the left is a tumor with possible invasion into the perirectal tissue, i.e. T3 (arrow). The resection margin is wide and there is no enlargement of the lymph nodes adjacent to the mesorectal fascia. This tumor is classified as T3 MRF-. In the Netherlands, as in most European countries, this patient will receive a short preoperative course of radiotherapy followed by TME.
Perirectal infiltration/invasion
The sensitivity of MRI in diagnosing perirectal tissue invasion is 82%. Visible radiant infiltration of perirectal tissue may be a trap, as it can be the result of either tumor growth or a local desmoplastic reaction. To avoid misinterpretation, tumors with perirectal tissue infiltration are recommended to be staged as T3. The degree of exophytic spread is a prognostic factor. The MR images on the left show two tumors with a similar MR pattern. Image A showed perirectal tissue invasion. In image B, the tumor was delimited by the intestinal wall, stage T2, perirectal infiltration of fiber in this case was the result of a desmoplastic reaction. This feature does not have a significant effect on the choice of treatment tactics when differentiating between T2 MRF and T3 MRF tumors. Both tumors will undergo TME or preoperative low-dose radiotherapy 5x5 Gy followed by TME
Diagnosis of the disease
Colonoscopy is the gold standard for diagnosing the disease. It allows you to examine the entire surface of the intestine using special light filters and vital staining methods.
Detection of serrated adenomas requires a good bowel cleansing. In comparison, a satisfactory level of training is sufficient to diagnose ordinary adenomatous polyps. As we have already noted, serrated neoplasms can easily be mistaken for an ordinary fold of the intestinal mucosa, so this requires not only high-quality cleaning of the intestinal wall, but also special vigilance and research technique. In particular, the likelihood of detecting such formations is influenced by the speed at which the colonoscope is withdrawn. 9 minutes is considered optimal. In addition, various additional options are used:
- Inspection in autofluorescence mode.
- Inspection in white light.
- Narrow spectrum inspection.
- Chromoscopy with indigo carmine, methylene blue, crystal violet.
The final diagnosis is established after a morphological study of the removed polyp or its biopsy material.
Complications in the presence of serrated adenoma
The main danger of serrated adenomas is the possibility of their malignant transformation into cancer. Until a few decades ago, it was believed that colorectal malignancies develop only from adenomatous polyps. Accordingly, it was recommended to simply observe villous neoplasms. But later it turned out that these tumors can also degenerate into cancer, and have their own, unique path of carcinogenesis. The larger the size of the polyp and the longer it exists, the higher the risks of malignant transformation. The most dangerous in this regard are large, long-existing neoplasms on a wide base.