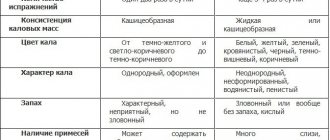
The role of normal microflora in protecting the reproductive tract of women
The study of the microflora of the female reproductive tract has a long history.
The pioneers in the study of vaginal microflora were V.V. Stroganov, A. Doderlein, it was they who showed its importance in protecting the reproductive tract of women from potential infection. V.V. Stroganov, in his doctoral dissertation “Bacteriological studies of a woman’s genital canal at various periods of her life,” wrote: “The anatomical features of the female genital canal create conditions for the development of bacteria... Pathogenic bacteria are weakened in their infectious power while in the vagina... Vaginal microbes destroy them.”
In the process of evolution, an optimal and well-coordinated system for protecting the female reproductive tract from pathogens has been formed. One of the key roles in this system belongs to colonization resistance - a set of mechanisms that impart individual and anatomical stability to normal microflora, ensure the prevention of colonization of the host organism by foreign microorganisms and include specific factors of local immunity and normal microflora [1].
Resident flora is usually divided into obligate and facultative. Obligate microorganisms play a significant role in protecting the reproductive system from pathogens of infectious diseases and are constantly present in the vagina of a healthy woman [1, 2]. Facultative microorganisms are found quite often, but not always. Transient flora introduced from the outside include non-pathogenic, opportunistic microorganisms and obligate pathogens. Lactobacilli predominate in 96% of healthy women and are the main representatives of obligate microflora; they perform a protective function, which is associated with colonizing ability and direct antimicrobial activity [2, 3]. Lactobacilli, being tightly adhered to the epithelial cells of the vagina, are an integral part of the environmental barrier, blocking the receptors of mucosal cells necessary for the adhesion of pathogenic microorganisms [3]. Lactobacillus spp.
are low virulent, but recent studies show that under certain conditions they can cause an infectious process.
The literature describes a few cases of association of Lactobacillus spp.
with the development of lesions of the lower and upper parts of the reproductive tract [4].
Lactobacilli must be functionally active, i.e., have the ability to produce hydrogen peroxide. Only in this case can we talk about the full stabilizing function of the microbiocenosis in the vagina [5, 6]. The level of acidity of vaginal discharge is affected not only by the concentration and functional activity of the lactobacillary flora, but also by the presence in excess of other facultative and transient microorganisms. The presence of anaerobic flora, such as Gardnerella vaginalis
,
Bacteroides spp., Peptococcus spp., Mycoplasma hominis, Mobiluncus spp.,
can lead to a sharp decrease in vaginal acidity and the development of a dysbiotic process [6, 7]. For example, a comparison of clinical picture data with the results of cultural diagnostics and the state of the vaginal microcenosis revealed a condition characteristic of cytolytic vaginosis in 36.54% of the examined women, while only lactobacilli were identified [8]. Microbiological studies in patients with various clinical diagnoses have shown that cytolytic vaginosis most often accompanies cervical ectopia [8].
Stages of dysbiosis
Depending on the degree of development of the disease, dentists distinguish four stages of dysbiosis:
- Latent. The first, latent stage is characterized by subtle changes in the number of microorganisms of one strain. The patient feels well and does not experience any symptoms of inflammation.
- Subcompensated. The number of lactobacilli decreases, the disease has a blurred picture. The patient may feel discomfort in the oral cavity, but does not always understand that this is dysbacteriosis.
- Pathogenic. Lactobacilli are observed in minimal quantities in the oral cavity. The oral cavity begins to be populated by a facultative pathogenic environment.
- Decompensated. In addition to severe inflammation in the mouth, uncontrolled growth of yeast-like fungi occurs. The functioning of the salivary glands is disrupted, and an unpleasant taste and burning sensation occurs in the mouth.
Advanced forms of dysbiosis are characterized by symptoms such as:
- inflammation of the gums and mucous membranes;
- plaque on the teeth and surface of the tongue;
- bleeding gums;
- ulcers and blisters on mucous membranes;
- increased body temperature;
- swelling and soreness of the tongue;
- dry skin, sticking in the corners of the mouth.
The role of obligate pathogens in the development of vaginal dysbiosis
According to WHO data updated in 2015, every day 1 million people acquire sexually transmitted infections (STIs); Every year, 357 million are infected with one of four pathogens: Chlamydia trachomatis
(131 million),
Trichomonas vaginalis
(143 million),
Neisseria gonorrhoeae
(78 million),
Treponema pallidum
(5.6 million) [9].
Currently, inflammatory diseases of the genital organs are classified as mixed polymicrobial infections, the most important pathogens of which, according to WHO, are anaerobic-aerobic associations (25–60%), N. gonorrhoeae
(25–40%),
C. trachomatis
(25–30 %),
Mycoplasma spp.
(up to 45%). According to a number of authors, acute inflammatory diseases of the uterine appendages are accompanied by severe dysbiosis of the genital tract and often occur latently [2].
According to the American Association of Obstetricians and Gynecologists, discharge accompanies no more than half of the episodes of gonococcal or chlamydial cervicitis and up to 35% of trichomonas vaginitis, which indicates a reversal of clinical symptoms and can complicate timely diagnosis and therapy. It is possible that changes in the composition of facultative microflora may also play a certain role in changing the clinical picture of diseases.
Thus, metagenomic analysis showed that C. trachomatis
significantly more often associated with a microbiota, which is dominated by anaerobic bacteria, such as
G. vaginalis, Prevotella amnii
,
Prevotella buccalis, Prevotella timonensis
,
Aerococcus christensenii
and
Variovorax guangxiensis
; the presence of these microorganisms can act as a potential biomarker of chlamydial infection [10].
It has also been established that during chlamydial infection, the production of lactoferrin, interleukins IL-6, -1α, interferons IFN-α and -β significantly increases with a very low level of IFN-γ, which contributes to the formation of chronic inflammation, characterized by increased production of immune mediators responsible for damage fabrics. Moreover, RT Fortner et al. indicate a potential risk of developing ovarian cancer in patients who are seropositive for C. trachomatis
[11].
Trichomonas infection occupies a leading place in the structure of STI incidence and most often represents a mixed infection [9]. Simultaneously with T. vaginalis
Genital mycoplasmas are detected quite often.
Analysis of data from 1257 women showed that the prevalence of M. hominis
was 57.4%,
Ureaplasma urealyticum
- 54.9%.
Of 50 patients with trichomoniasis, 76% were coinfected with M. hominis
, respectively, patients with
T. vaginalis
had an increased risk of infection with mycoplasmas [12].
Trichomonas infection is accompanied by a change in the species composition of resident microflora with an increase in the number of microorganisms such as G. vaginalis
,
Atopobium vaginae
and
Prevotella bivia
. This clinically significant interaction between these microorganisms may require systematic screening of mycoplasmas among patients with trichomoniasis for optimal treatment of STIs [13]. It is also obvious that Trichomonas, being obligate pathogens, contribute to the initiation and implementation of a cellular immune response involving a cascade of cytokine-mediated reactions, induction of cytotoxicity, and the nature and outcome of inflammation will depend on the spectrum and level of produced cytokines and the activity of multiple proteinases [14].
Obligate pathogens that can infect the urogenital tract include Mycoplasma genitalium
.
This microorganism was identified by D. Taylor-Robinson in early 1982. M. genitalium
is the smallest and most mobile bacterium, has a flask-shaped shape and an elongated terminal structure used to ensure gliding movement, penetration into the mucus layers covering epithelial cells, for attachment to cell surfaces and penetration into them.
The ability of M. genitalium
to attach to the surface of eukaryotic cells is determined by receptors containing neuraminic acid, which causes a pronounced cytopathogenic effect and the formation of a cellular inflammatory response [15].
In a 2022 publication, M.R. Mahlangu et al. indicate a relationship between M. genitalium
and human immunodeficiency virus (HIV), which was determined by examining 4731 patients [16].
Among persons screened for STIs, the relative prevalence of M. genitalium
in men and women was 8.9% and 10.6%, respectively, while in HIV-infected patients the detection rate of
M. genitalium
reached 48.9%. This significant difference in HIV seroprevalence is particularly pronounced among women [16].
For patients with HIV infection, any pathogens and pathobionts can play a critical role in the development of the infectious process, including new microsporidia pathogens that cause urinary tract infections, which often occur in a subclinical form. M. Wesołowska et al. indicate that microsporidiosis can cause severe complications or death in immunosuppressed patients, and suggest that testing for microsporidiosis should be included in routine screening of HIV-positive patients, even in asymptomatic patients [17].
What causes bacterial infections in women
If we look at the classification of bacteria that cause vaginitis and cervicitis, we can distinguish:
– aerobic, which are diagnosed in 30% of patients. However, recently doctors have been talking about an increase in the number of patients with anaerobic infections, for example gardnerella;
– intracellular mycoplasmas – ureaplasma.
With all the diversity of pathogens, it is worth noting that almost all of them are opportunistic. Associations of pathogens are common; every third woman with problems of the urogenital tract has from 6-10 pathogens. A bacterial urinary tract infection in women can have a latent and/or asymptomatic course, when a woman may not experience the characteristic ailment for a long time: vaginal discharge, itching, discomfort, and so on. At the same time, there is an increase in the resistance of pathogens to antibiotics, which makes some previously adopted regimens ineffective.
Inflammatory processes caused by opportunistic microorganisms
Research in recent years has brought significant changes to our understanding of the role of opportunistic microorganisms in the development of inflammatory processes in the urogenital tract.
In the conditions of modern society, there is a clear tendency towards a change in the etiological structure of infectious diseases, namely a decrease in the proportion of infections caused by traditional pathogens and the increasing role of opportunistic microorganisms, an increase in cases of reversal of clinical signs, a combination of a mild clinical course with damage to the ascending parts of the genitourinary tract, cases of a complicated course with the formation of a complex of pathological symptoms and/or syndromes, an increasing frequency of mixed infections, when the etiological role of each participant in the inflammation is difficult to identify [18–22].
The symptoms of inflammatory diseases of the reproductive tract are determined not only by microorganisms present in the vagina, but also by a variety of functional disorders. According to the literature, chronic inflammation causes changes in the morphological structure of tissues, leads to disruption of microcirculation, ischemia and a decrease in its functional activity, thereby exacerbating microecological disorders of the reproductive system [23–25].
Violation of the immunological balance of the macroorganism leads to uncontrolled growth of microflora and its spread beyond a certain biotope. Only a massive accumulation of microorganisms in the source of infection can cause the development of an infectious process. According to some authors, the number of 103 CFU/ml of microorganisms can become such a critical mass. A significant antigenic load contributes to increased virulence of microorganisms and the formation of antibacterial resistance [24, 26].
It is obvious that opportunistic microorganisms, being an integral part of the vaginal biotope, will interact differently with the human immune system than obligate pathogens, which is accompanied by a change in the clinical picture when, in the absence of obvious signs of acute inflammation, the upper parts of the genital tract are involved in the pathological process and there is a real the threat of disruption of the endometrial receptor apparatus and the formation of adhesions [19, 20, 23].
The share of vaginal infections of nonspecific etiology is at least 40% among all infections of the reproductive system of women, and the most common participants in the combined process are microorganisms associated with bacterial vaginosis (BV): M. hominis
G. vaginalis, A. vaginae Prevotella bivia
(73.9% ), fungi of the genus
Candida
(32.5%), human papillomavirus (31%) [19, 24].
Quite often one has to deal with the condition of aerobic vaginitis, when there is a decrease in the number of lactobacilli and inflammation develops with the participation of aerobic microorganisms, in particular Escherichia coli, Enterococcus faecalis, Streptococcus viridans, Staphylococcus epidermidis, Streptococcus agalactiae, Staphylococcus aureus
[25].
It is a change in the number of a particular type of microorganism or the appearance of bacteria unusual for a given habitat that serves as a signal for adaptive or irreversible changes in the vaginal biocenosis [25, 26, 28]. A 2014 study involving 1817 women showed that in 432 different combinations of U. urealyticum, Ureaplasma parvum, M. hominis
,
Candida, G. vaginalis, A. vaginae
were clinically significant.
In addition, the microbial associations included microorganisms such as S. epidermidis, Staphylococcus saproрhuticus, Streptococcus spp., Corinebacterium xerosis, E. coli, E. fecalis
[27].
Disturbance of oral microflora: causes
Oral dysbiosis can be caused by a variety of diseases and problems. Violation of opportunistic microflora of the oral cavity most often causes problems such as:
- Diseases of the gastrointestinal tract. Malfunctions of the digestive organs lead to a slowdown in metabolic processes in the body. The absorption of vitamins and nutrients deteriorates, the balance of the intestinal bacterial environment is disrupted, which provokes problems in other organs and systems.
- Decreased immunity. If the body's resistance deteriorates, the oral cavity automatically becomes more vulnerable to pathogenic microflora.
- Chronic diseases. Often, small caries or stomatitis, if left untreated, can spread from the source of inflammation to the entire oral cavity.
- Bad habits, such as systematic drinking of alcohol and smoking, inevitably affect the quality of the salivary glands. Prolonged drying out or too much moisture in the oral cavity has a detrimental effect on the composition of the microflora.
- Poor nutrition and lack of vitamins worsens the quality of saliva and makes the microflora of the oral cavity more vulnerable.
- Taking antibiotics and certain medications, such as hormones;
- Wearing dentures.
The role of biofilms in the development of pathological processes in the reproductive tract
Today, the fact that 99% of microorganisms are contained in biofilms is proven. From a biological point of view, a biofilm is a special ecosystem that ensures the viability and preservation of its constituent species of microorganisms and increases their overall population stability [29]. Microorganisms in a biofilm, without changing their individual sensitivity, survive better when exposed to antibacterial drugs and carry out electrical communication, which ensures their metabolic relationship in the biofilm [29–31]. Five years ago, one of the mechanisms of interaction between microorganisms in a biofilm was described. The researchers found that a wave of depolarization triggered by metabolic stress in centrally located bacteria limits the ability of peripheral cells to take up glutamate and retain ammonium ions, making these metabolites more available to central microorganisms. The high rate of diffusion of potassium ions in the aqueous environment contributes to the synchronization of metabolic activity even at a distance [32]. The formation of biofilms at the site of inflammation leads to the development of chronic inflammation and the ineffectiveness of the therapy [28, 30, 31]. Candida seems interesting
and vaginal epithelial cells.
In the work of A. Swidsinski et al. Candida
was detected in 26 of 35 biopsies obtained from women with vulvovaginal candidiasis (VVC), but
Candida
was not detected in any of the cases.
Histopathological lesions were exclusively invasive and were accompanied by invasion of Gardnerella and Lactobacillus. The authors concluded that the histopathological lesions of VVC are predominantly invasive and polymicrobial in nature and do not resemble biofilms; the clinical significance of Candida
is unknown [33].
In the same study, it was possible to establish that the ultrastructure of vaginal epithelial cells after VVC is damaged, the local immune response is impaired, and antifungal drugs can significantly restore the damaged structure of the vaginal epithelium after VVC and enhance the protective immune function of the vaginal epithelium [33].
Of particular importance in the development of infectious and inflammatory diseases of the urogenital tract belongs to anaerobic microflora, in particular G. vaginalis
, which, having unique adhesive abilities, do not limit their location to the vagina alone, but very successfully colonize the upper parts of the genital tract [33].
Just 5–7 years ago it was believed that this microorganism was not sexually transmitted. However, a 2022 study showed that the putative profile of sexually transmitted BV derived from epidemiological studies may be consistent with its biofilm nature, the spread of scattered cells or cellular aggregates between hosts, i.e. it is not transmitted by G. vaginalis
. but a fragment of the biofilm into which this microorganism is included.
De novo
biofilm formation in response to prolonged pressure from the vaginal ecosystem should be considered a pathogenetic model. This circumstance will allow us to reconsider therapeutic approaches, which have so far been limited to inhibition of biofilm formation. Perhaps an innovative clinical trial incorporating a combination approach (using metronidazole and a surfactant specifically designed to disrupt biofilm) will provide significant advances in the treatment of recurrent BV [34].
The outcome of any inflammatory process, regardless of its etiology, is the result of the interaction of macro- and microorganisms. A number of pathological conditions leading to dysfunction of innate immune factors contribute to the activation of opportunistic flora, provoking inflammatory processes of varying localization and severity. Dysfunctions of innate immune structures usually manifest themselves in a decrease in the functional activity of phagocytic cells: inhibition of biocidal functions, suppression of their secretory activity, leading to a decrease in the production of biologically active messengers, which ultimately leads to persistent disturbances in the anti-infective defense system. A feature of inflammatory processes caused by opportunistic microorganisms is their long-term, chronic, sluggish course [18–20, 27]. On the one hand, opportunistic microorganisms in the process of evolution have developed a number of adaptive properties that allow them to evade the protection of the host’s immune system, and on the other hand, dysfunctions in the anti-infective defense system contribute to the development of chronic inflammation. In the chronic course of the disease, along with exudative ones, proliferative changes are also detected, manifested by inflammatory infiltrates in the subepithelial layer. Columnar epithelium in some areas transforms into multilayered squamous epithelium, often into keratinizing epithelium, which can result in scar tissue atrophy [23].
Possible complications of dysbiosis
It is important for each patient to closely monitor the state of the oral microflora. Lack of treatment for dysbiosis can lead to such unpleasant diseases as:
- pathological halitosis – bad breath caused by an imbalance of the oral microflora;
- caries – destruction of hard tooth tissues;
- pulpitis - inflammation of the pulp - the internal tissues of the tooth;
- periodontitis – inflammation of the tooth root membrane and adjacent tissues;
- gingivitis – inflammation of the oral mucosa;
- stomatitis – damage to the oral mucosa;
- periodontitis is a deep lesion of the periodontal tissue.
In addition, the close relationship between the state of the oral microflora and the state of the cardiovascular system has been scientifically proven. In 2008, it was proven in the USA that periodontal disease, as a source of chronic inflammation, is an independent risk factor for coronary heart disease (CHD).
So, now you know the role of normal oral microflora in the human body. Treat yourself carefully, and your healthy body will delight you every day.
Principles of therapy
All these circumstances force us to fundamentally change the approach to the treatment of chronic inflammatory process. It is important not only to influence the etiological component of the inflammatory process, to eliminate disturbances in the local immunological status, but also to prevent the formation and increase in the mass of biofilm [7, 8, 19, 27]. And in this aspect, a combination of drugs acting locally on various groups of agents is very promising [35]. Taking into account the fact that the most common participants in microbial associations leading to the development of an infectious-inflammatory process are anaerobes and fungi of the genus Candida
, drugs containing metronidazole and an azole derivative may be relevant.
In the Procedure for the provision of medical care in the profile of “dermatovenereology”, Clinical recommendations of the Russian Society of Dermatovenereologists and Cosmetologists 2022, drugs of the 5-nitroimidazole group are called the drug of choice for the treatment of urogenital trichomoniasis and BV [36].
The mechanism of action is the biochemical reduction of the 5-nitro group of metronidazole by intracellular transport proteins of anaerobic microorganisms and protozoa. The reduced 5-nitro group of metronidazole interacts with the DNA of microbial cells, inhibiting the synthesis of their nucleic acids, which leads to the death of bacteria and protozoa. The spectrum of action is wide: against T. vaginalis, G. vaginalis, Giardia intestinalis, Entamoeba histolytica,
as well as obligate anaerobes (
Bacteroides spp., Fusobacterium spp., Veillonella spp., Prevotella spp.)
and some gram-positive microorganisms (
Eubacter spp., Clostridium spp., Peptococcus spp., Peptostreptococcus spp.
). Most aerobic microorganisms and facultative anaerobes are insensitive to metronidazole, but in the presence of mixed flora (aerobes and anaerobes), metronidazole acts synergistically with antibiotics effective against aerobes.
For the treatment of inflammatory diseases of the urogenital tract associated with fungi of the genus Candida
, the drug of choice is azoles, in particular miconazole.
Miconazole is an effective antimycotic agent that acts primarily against dermatophytes and yeast fungi. When used intravaginally, it is active mainly against Candida albicans.
Miconazole suppresses the biosynthesis of ergosterol in fungi and changes the composition of other lipid components in the membrane, which leads to the death of fungal cells, while not changing the composition of normal microflora and vaginal pH [37]. The effectiveness and safety of the fixed combination of metronidazole and miconazole have been noted in a number of studies [35, 38].
The modern pharmaceutical market offers various drugs for the treatment of anaerobic and mycotic infections, but medical practitioners prefer combination drugs with a wide spectrum of action. One of the drugs that successfully combines two active ingredients - metronidazole and miconazole - is Ginocaps, containing 100 mg of metronidazole and 100 mg of miconazole. This vaginal drug can be used successfully for BV and VVC in combination with oral metronidazole. According to the Clinical Guidelines of the Russian Society of Dermatovenerologists and Cosmetologists (2017), it is preferable to use topical drugs for the treatment of such conditions. When trichomonas and mycotic infections are combined in the case of severe exudation and inflammation, it is also recommended to use topical protisticidal drugs simultaneously with oral medications ,
but systemic enzyme therapy, immunomodulatory therapy and therapy with local antiseptic drugs are not recommended [30]. It should be noted that the excipients included in the vaginal capsules, such as glycerin, titanium dioxide, lecithin, are a donor of phospholipids and help reduce exudation.