Authors: Marco Di Serafino, Valerio Vitale, Rosa Severino, Luigi Barbuto, Norberto Vezzali, Federica Ferro, Eugenio Rossi, Maria Grazia Caprio, Valeria Raia, Gianfranco Vallone
Functioning of the pancreas
The pancreas, or more precisely the islets of Langerhans, which are clusters of endocrine cells, contribute to the production of insulin and glucagon. These hormones regulate metabolic processes in the body and have completely opposite functions. Insulin lowers glucose in the body, while glucagon increases this level.
The pancreas has a special structure and consists of the following parts:
- Head: It protrudes slightly from behind the stomach.
- Body: the main part of the organ, has a triangular shape and is located behind the stomach, separated from it by the omental bursa.
- Tail: The posterior pear-shaped part of the organ that rests on the spleen.
The length of the pancreas in an adult ranges from 14 to 22 cm, and its average weight reaches an average of 70-80 grams. For children, other normal indicators apply. The size of the pancreas in children directly depends on how old the baby is.
Dimensions of the pancreas in a child
The pancreas is difficult to diagnose; due to the peculiarities of its anatomical location, it is absolutely impossible to determine its size using the palpation method, so doctors resort to ultrasound examination.
The organ begins to develop in the womb, after the fifth week of pregnancy. The size of the pancreas in a newborn baby often reaches 4.5-5 cm; during the first 6 months, after the baby is born, the organ increases in size by about 10 mm. The most dramatic jump in the growth of the pancreas occurs during adolescence and puberty.
During the first year of life, the child is recommended to undergo an ultrasound of the pancreas; there are also a number of medical indications for this examination. Using this diagnostic method, the doctor can find out the size of this digestive organ. If the indicators differ from the norm, this does not always indicate pathological diseases. Doctors use special tables that indicate the sizes for the pancreas in children, which are considered normal.
| Age | Head size | Body size | Tail size |
| Up to a month | 10-14 | 6-8 | 10-14 |
| 4 weeks - year | 15-19 | 8-11 | 12-16 |
| year-5 years | 17-20 | 10-12 | 18-22 |
| 6-10 years | 16-20 | 10-13 | 18-22 |
| 11-18 years old | 16-20 | 11-14 | 20-24 |
Difficulties in diagnosing chronic pancreatitis in children
About the article
3215
0
Regular issues of "RMZh" No. 6 dated March 29, 2006 p. 483
Category: General articles
Authors: Kornienko E.A. 1, Zaichkina A.A. , Fadina S.A. 1 Federal State Budgetary Educational Institution of Higher Education St. Petersburg State Pediatric Medical University of the Ministry of Health of Russia, St. Petersburg
For quotation:
Kornienko E.A., Zaichkina A.A., Fadina S.A. Difficulties in diagnosing chronic pancreatitis in children. RMJ. 2006;6:483.
Diagnosis of pancreatic pathology is one of the most complex areas of gastroenterology. Symptoms characteristic of pancreatitis are detected in approximately 10–12% of children with chronic gastroduodenal diseases. However, as a rule, they are not accompanied by hyperamylasemia, steatorrhea, and do not have pronounced structural changes according to ultrasound data, and therefore are interpreted by practitioners as functional disorders of the pancreas. Favorite diagnoses in this case are “dyspancreatism” and “reactive pancreatitis”, and these terms are used as equivalent without sufficient substantiation of the essence of their underlying pathology. At the same time, it should be taken into account that in ICD-10 there are no diagnoses of “dyspancreatism” or “reactive pancreatitis”. However, there are “dysfunctional biliary tract disorders” (K82.8), which are divided into 2 subtypes: gallbladder dysfunction and sphincter of Oddi dysfunction. The latter, in turn, are divided into 4 options, three of which correspond to biliary dysfunction, and the fourth to pancreatic dysfunction. The pancreatic variant of sphincter of Oddi dysfunction is characterized by “pancreatic” abdominal pain, and sometimes a slight increase in the level of amylase in the blood is possible. In this case, structural changes in the parenchyma of the gland and a decrease in its function are not typical. Thus, in the absence of signs of pancreatitis and the presence of characteristic complaints, the diagnosis of “dysfunction of the sphincter of Oddi, pancreatic variant” can be used in pediatric practice as the most acceptable.
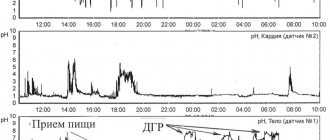
The term “reactive pancreatitis” is often used instead of the recommended ICD-10 “recurrent pancreatitis” (K86) and “chronic pancreatitis” (K87), meaning its secondary nature against the background of existing pathology of the digestive organs (usually gastroduodenal). However, the term “reactive pancreatitis” does not reflect the true mechanism of development of the pathology, nor the degree of damage or the functional state of the gland. Rather, its widespread use in practice is a kind of trick when the doctor, not having sufficient grounds for making a diagnosis of “chronic pancreatitis,” does not want to continue the diagnostic search and makes a non-binding, vague diagnosis, without essentially understanding what is going on We are talking about a functional pathology or an already formed chronic disease. Moreover, both can be accompanied by underlying gastroenterological pathology. These diagnostic difficulties are due to the lack of reliable clinical and laboratory and instrumental criteria for chronic pancreatitis in children in everyday medical practice. If we turn to the definition of “chronic pancreatitis”, most guidelines indicate its 2 main signs - persistent structural changes in the gland (usually fibrosis, less often - changes in the ductal system) and functional failure. Currently, when, along with ultrasound, visualization methods such as computed tomography, magnetic resonance imaging, endosonography, retrograde cholangiopancreatography are increasingly used in practice, the diagnosis of structural changes becomes possible already in the early stages of pathology. In the arsenal of modern medicine there is a reliable non-invasive method for assessing the exocrine function of the pancreas - the determination of elastase-1 in feces. Their wider use can solve the problem of diagnosing chronic pancreatitis in children. The purpose of our work was a comprehensive assessment of clinical, laboratory and morphological signs of pancreatic pathology in children and development of diagnostic criteria for chronic pancreatitis. Material and methods. We observed 47 children aged 9 to 17 years (20 boys, 27 girls) with clinical symptoms characteristic of recurrent pancreatitis. Children were admitted to the hospital with complaints of repeated pain with a predominant localization in the epigastrium and left upper quadrant of the abdomen, accompanied by certain dyspeptic symptoms; An objective examination revealed pain on palpation in the projection of the pancreas. All children had a background gastroenterological pathology: 45 had gastroduodenal pathology (1 had duodenal ulcer, 44 had chronic gastroduodenitis), 3 had cholelithiasis, 10 had giardiasis. Clinical symptoms were assessed using a specially developed questionnaire with a score of complaints, anamnestic data and objective signs of the disease. All patients underwent a study of clinical and biochemical blood tests, a 3-fold coprological study, FEGDS with a biopsy from the stomach and duodenum and subsequent morphological examination of biopsy samples, ultrasound of the abdominal organs with a study of the contractility of the gallbladder and measurement of the size of the pancreas on an empty stomach and postprandially. For a more accurate assessment of structural changes in the gland, patients underwent endosonography. To assess the exocrine function of the pancreas, the level of elastase-1 in the feces was examined in all patients. Considering the similarity of clinical symptoms in all children, they were divided into groups depending on the presence of signs of structural changes in the gland (according to ultrasound and endosonography) and signs of impaired exocrine function of the gland (according to the elastase test). We considered a decrease in the level of elastase-1 in feces below 200 mg/g as a criterion for exocrine insufficiency. In accordance with the selected criteria, we identified 3 groups of patients: the 1st group consisted of 15 children in whom ultrasound signs of gland fibrosis were detected and a decrease in the level of elastase-1 in the feces was detected. In our opinion, children in this group can be considered as patients with chronic pancreatitis (CP). Group 2 included 20 children who had ultrasound signs of structural changes in the pancreas, but the elastase-1 level was normal. Considering the recurrent nature of the pain syndrome and the absence of functional pancreatic insufficiency, we considered these patients as patients with recurrent pancreatitis (RP). Group 3 included 12 children who had no ultrasound changes in the structure of the gland and no signs of a decrease in its function, but since they had pain in the area of the projection of the gland, we diagnosed them with the pancreatic variant of sphincter of Oddi dysfunction (SDO). Results The age composition of the three compared groups did not have significant differences, but in group 1 there were only children over 12 years old. There were no gender differences; girls predominated only slightly in all groups. The structure of the background pathology in patients of all compared groups was represented predominantly by chronic gastroduodenitis. It was diagnosed in 80% of children in group 1, 86% in group 2 and 92% in group 3. In 80–83% of all three groups it was associated with H. pylori infection. One patient of group 3 was diagnosed with duodenal ulcer. Gallstone disease was detected in 1 child of group 1 and 2 children of group 2; in the same group, 2 patients had gallbladder anomalies (kinks). Impaired contractile function of the gallbladder was diagnosed according to echocholecystography in all patients we observed; the PDF of the gallbladder in groups 1, 2, 3 was 0.94, 0.92, 0.9, respectively. Giardiasis was detected in 30% of children in groups 2 and 3 and 14% in group 1. Thus, a similar background pathology occurred in all patients of the compared groups, all showed signs of dysfunctional disorders of the biliary tract, it should only be emphasized that cholelithiasis and gallbladder anomalies were identified only in groups of patients with pancreatitis. Clinical symptoms in all compared groups were represented predominantly by pain (Fig. 1). In the majority of children in group 1, pain had an average (57%) duration, in 28% it was long-lasting. They were in 70% aching, moderate in intensity (43%) with a predominant localization in the epigastric region (71%), less often in the left hypochondrium (28%). Children of group 3 had a similar pain syndrome, in which aching (84%) pain in the epigastric region (84%) of average duration (66%), moderate intensity (100%) also dominated. The most pronounced pain syndrome was observed in patients of group 2, 70% of whom had prolonged pain, intense cramping in 40%, severe pain in 50%, with predominant localization in the left hypochondrium (60%). In the same group, there was a more clear connection with food intake; pain occurred after eating, especially after errors in the diet (62%). In group 1, such a connection was noted in 43% of patients, in group 3 – only in 16%. The pain index was also maximum in children of group 2 (20.2±2.3), in group 1 it was slightly lower, but had no significant differences (18.5±2.5, p>0.05), and in in group 3 was significantly lower than in patients with pancreatitis of groups 1 and 2, and amounted to 13.1 ± 3.4 (p) In assessing the duration of the disease, we were guided by anamnestic indications of the onset of abdominal pain. However, taking into account the presence of background gastroenterological diseases in all children , it is very difficult to assess the onset of development of pancreatopathy. Most patients of all compared groups had an average duration of the disease of about 3 years, but approximately 1/3 of children indicated a short duration of less than a year, including among patients with CP. These data may indicate the possibility of a latent course chronic pancreatitis at a certain stage.A clear onset in the form of confirmed acute pancreatitis was observed only in 3 children of group 2, but 30% of children from groups 1 and 2 had episodes of severe attacks of abdominal pain, for which patients were hospitalized in surgical hospitals. There were no such episodes in children of group 3. The course of the disease in 70% of children of group 2 and 57% of children of group 1 was characterized by recurrent pain syndrome, at the same time, in group 3 only 43% had such complaints, and in 50% the disease proceeded monotonously, with short-term, changing and not so vivid symptoms. An important indicator, in our opinion, is the trophological status of the patient. In group 1, we noted signs of protein-calorie deficiency in 65% of patients, in group 2 – in 48%, in group 3, all children corresponded to normal physical parameters. When assessing scatological data, it should be noted that there was no steatorrhea with neutral fat in all children, including in group 1. In this regard, we believe that the coprogram cannot serve as a reliable indicator of the functional state of the pancreas in older children. We observed an increase in amylase activity in the blood in 40% of children in group 2, 17% in group 1 and 8% in group 3; in all cases it was small (no more than 1.5–2 times higher than normal) and short-lived. Ultrasound examination of the pancreas showed an increase in its size in approximately 20% of children in groups 1 and 2 and in none of the children in group 3, in 43% of children in group 1 and 30% in group 2, increased echogenicity of the gland parenchyma was noted, in 50% of patients in group 2 and 28% of group 1 had hyperechoic inclusions. These were also detected in 15% of group 3. At the same time, a normal ultrasound picture was described in 30% of the 2nd and 17% of children of the 1st group. In comparison with these data, the results of endosonography turned out to be more informative. Changes in the pancreas were detected in all patients of groups 1 and 2 and in none of the 3 groups. In all patients with CP, focal or linear fibrous changes in the pancreatic parenchyma were detected; in RP, similar changes were detected in 67%; in 33% of children in this group, an increase in the size and a decrease in the echogenicity of the gland was noted, in 2 cases - thickening of the walls of the Wirsung duct and its unevenness. We found a discrepancy between the results of conventional abdominal ultrasound and endosonography in 43% of patients. The average level of elastase-1 in feces in patients of group 1 was 95.8±23.4 mg/g, group 2 – 445±25.3 mg/g, group 3 – 466.2±18.6 mg/g. Discussion Our study showed that CP is not uncommon in childhood. The use of modern diagnostic methods, such as endosonography and examination of the level of elastase-1 in feces, makes it possible to verify with sufficiently high accuracy structural changes in the pancreatic parenchyma and a decrease in its function, confirming the diagnosis of CP (Fig. 3,4). It is important to note that the symptoms of RP, which occurs without a decrease in the exocrine function of the pancreas, are very similar to those in CP, but are distinguished by a greater severity of pain. These data suggest that RP and CP are, in fact, one disease, possibly its stages: with preserved and reduced exocrine function of the gland. Probably, the clinical symptoms at the initial stages of the development of the disease manifest themselves more manifestly, and as fibrous-atrophic changes in the gland progress and its functionality decreases, it loses its severity and becomes more monotonous, without losing some, in particular, dyspeptic, manifestations and often accompanied by trophological disorders. At the same time, the pancreatic variant of DSO is characterized by more modest symptoms, 100% combined with gastroduodenal pathology and biliary dysfunctions, which confirms its secondary nature. In accordance with the data obtained, we propose to use certain criteria for diagnosing CP in children, which are given below. Diagnostic criteria for chronic pancreatitis in children Main 1. Repeated episodes of abdominal pain for at least 1 year with localization: • in the upper left quadrant • deep in the epigastrium • in a stripe from hypochondrium to hypochondrium. 2. Previously diagnosed acute pancreatitis. 3. Signs of a decrease in the exocrine function of the pancreas according to the secretin-pancreozymine test or elastase-1 in the feces (below 200 mg/g) 4. Changes in the structure of the pancreas according to endosonography, computed tomography or magnetic resonance imaging. Additional 1. Changes in the size and structure of the pancreas according to abdominal ultrasound. 2. Steatorrhea with neutral fat. 3. Increased levels of lipase and (or) pancreatic amylase in the blood and (or) urine. 4. The connection of the above-described abdominal pain with errors in the diet (fatty or rich foods). 5. The connection between the above-described abdominal pain and heaviness in the epigastrium and nausea (vomiting). 6. History of episodes of severe abdominal pain that led to emergency hospitalization with suspected surgical pathology. 7. Diabetes mellitus. 8. Gallstone disease. 9. Anomalies of the common bile duct. 10. Hereditary hyperlipidemia with obesity. 11. Protein-calorie deficiency. To confirm the diagnosis of chronic pancreatitis, 4 criteria (including 1 main one) are sufficient. Establishing a correct diagnosis facilitates the appointment of adequate therapy. With the pancreatic variant of DSO, it is necessary to treat first of all the underlying disease, for example, HP-associated gastroduodenitis or giardiasis. In this case, it is important to eliminate spasm of the sphincter of Oddi, which is best achieved by prescribing smooth muscle antispasmodics. Traditional drugs, such as drotaverine, papaverine, have a fairly short-term effect and, when prescribed repeatedly, can affect vascular tone. Therefore, preference should be given to mebeverine (Duspatalin®), which, by blocking sodium channels and mobilizing calcium stores in cells, relieves spasm of smooth muscles without causing hypotension. The drug has a selective effect on the sphincter of Oddi without causing side effects. Prescribe Duspatalin 2 times a day, 200 mg before meals. Therapy for exacerbation of CP involves functional unloading of the pancreas, primarily reducing the stimulating effects of secretin and cholecystokinin. The first, as is known, is produced in response to duodenal acidification, therefore, the treatment of a patient with CP in the acute stage should include antisecretory drugs: proton pump inhibitors (omeprazole, rabeprazole, esomeprazole) at a dose of 1 mg/kg per day in 2 doses for 30–40 min. before meals. The second is stimulated by peptides, therefore the administration of enzyme preparations that break down proteins in the cavity of the small intestine, according to the feedback principle, helps to reduce the stimulating effects on the pancreas. Against the background of exacerbation of CP, pancreatic enzymes with a higher content of proteinases are optimal. There are no special drugs for this purpose, so in practice the same enzyme preparations are used as for replacement therapy. Smooth muscle antispasmodics are also indicated in this case, as they help facilitate the outflow of pancreatic juice and reduce intraductal hypertension. Treatment of patients with detected exocrine pancreatic insufficiency against the background of CP should include pancreatic enzyme preparations. The choice of drug should be based on the following criteria: • High lipase content in the drug. Lipase is the most vulnerable enzyme because it is destroyed by chymotrypsin and works only in the proximal parts of the small intestine. The dose of the enzyme is calculated based on lipase; for initial therapy, 1000 units is usually sufficient. lipase per 1 kg of body weight per day, if the effectiveness is insufficient, the dose is increased by 2 times, then selected individually. The criterion for dose adequacy is the disappearance of dyspeptic disorders and sufficient weight gain. The daily dose is divided into all meals in accordance with its quantity, usually for main meals the dose is 2 times higher than for snacks. • The ratio of colipase to lipase is higher than 1, it is the highest in Creon® and is 1.9. • The presence of a shell that protects the drug from the effects of gastric juice, since its main enzymes - lipase and trypsin - are destroyed at acidic pH values: lipase - at a pH below 4, trypsin - below 3. For lipase to act effectively, it is necessary to maintain a pH above 4 in the stomach within 60 minutes after taking the drug, in the duodenum - within 90 minutes. The best method of protection is acid-resistant microspheres, which dissolve at a pH above 5.5, that is, in WPC. • Uniform supply of the drug to the duodenum along with food. This ensures the active participation of enzymes in the process of cavity digestion from the very beginning of the entry of chyme into the intestine. The gatekeeper does not allow large particles (more than 1.4 mm) to pass through, so the optimal form of the enzyme is minimicrospheres with a diameter of less than 1.4 mm. Creon® minimicrospheres have the smallest diameter - 0.8–1.0 mm, which allows the drug to freely penetrate the intestines and actively participate in the digestive process from the very beginning. With a decrease in bicarbonates, which can take place with CP, it is possible to acidify the DPP. It can disrupt the activation of enzymes covered with an enthusiastic membrane, inactivate lipase and cause precipitation of bile salts and the formation of calcium soaps of fatty acids, which will ultimately reduce the effectiveness of enzyme therapy and maintain the symptoms of malabsorption. In these cases, the prescription of antisecretory drugs (in particular, proton pump inhibitors at a dose of 0.5–1.0 mg/kg/day) can also be useful, since a decrease in hydrochloric acid products in the stomach will ultimately lead to an increase in pH in DPK And increase the effectiveness of enzyme therapy. To this end, it is unacceptable to use antacid drugs, since they bind pancreatic enzymes and reduce the effectiveness of therapy. In the treatment of CP, it is necessary to avoid drugs containing components of bile, since bile acids lead to excessive stimulation of the pancreas, which can maintain pain. The patient should receive enough protein and calories, the restriction applies mainly to fatty foods and extractive substances. It is necessary to ensure sufficient intake of vitamins and trace elements. The duration of enzyme therapy can vary, with minor degrees of the extension of the pancreas, a partial restoration of its function is possible, so the course of treatment can be limited to 2-3 months with subsequent cancellation and re -evaluating exocrine function. Functional peace against the background of fermented therapy can help improve the morphological and functional state of the pancreas, the question of the need for repeated courses or constant replacement therapy is solved individually. Literature 1. Belmer S.V., Gasilina T.V. Problems of digestive failure: definition, identification and correction. - Ross. Med. Journ. Children's gastroenterology and nutrition, 2003, t.11, No. 3, p.119–121. 2. Okhlobystin A.V. Diseases of the pancreas. - Consilium Medicum, 2002, Appendix, p. 26–31. 3. Sarles H., Adler G., Dani R. The Pancreatity Classification of Marseilles - 88. - Scand.j.gastr., 1989, v.24, P.641–642. 4. Minushkin O.N. Chronic pancreatitis: some aspects of pathogenesis, dagestic and treatment. - Consilium Medicum, 2002, Appendix Issue 1, p. 23–26. 5. Freind G.G., Sokolov Yu.Yu. Morphogenesis of duodenopancreatobiliary anomalies in children. - Perm, 2003, 220 p. 6. Kharitonova L.A. Gallstone -stone disease in children. - M., 2002, 68s. 7. Kornienko E.A., Gonchar N.V., Tkachenko E.I. The controversial and unresolved issues of pancreatology in the practice of a pediatrician and therapist. - Gastroenterology of St. Petersburg, 2005, No. 3–4, p. 29–32. 8. Dimagno EP, Go VLM, Summerskill Whj Relations Between Pancreatic Enzyme Outputs and Malabsorption in the Pancreatic InSufficency. - N.engl.j.med., 1993, v.288, P.813–815. 9. Adler G., Mundlos S., Kuhnelt P., Dreyer E. New Methods for Assessment of Enzyme Activity: Do the Help To Optimize Enzyme Treatment? - Digestion, 1999, V.54, S. 2, P.3–10.
Content is licensed under a Creative Commons Attribution 4.0 International License.
Share the article on social networks
Recommend the article to your colleagues
Indications for ultrasound
Ultrasound examination is prescribed for both children and adults for the following indications or suspicions:
- feeling of discomfort and pain symptoms in the left hypochondrium;
- weight loss in a short period of time, without good reason;
- clarification of the suspected diagnosis:
- possible pathological anomalies in the structure and development of both the organ itself and its tissues;
- diabetes;
- deformation of the posterior wall of the stomach;
- pathological changes identified during x-ray diagnostics;
- hepatitis, yellow coloration of the skin and mucous membranes;
- problems with stool: changes in its color, consistency, frequency;
- causeless vomiting and nausea;
- excessively increased feeling of thirst.
How is ultrasound examination performed on children?
An ultrasound of internal organs takes no more than 10-15 minutes and does not cause any discomfort. To complete the procedure, just follow a few simple steps:
- The child is undressed to the waist and placed on a covered couch next to the apparatus.
- The doctor applies a special gel to the sensor and begins to move it over the child’s stomach. If necessary, the patient will be asked to hold his breath, take a deep breath, suck in his stomach, turn on his side or stand up.
- The ultrasound examination is interpreted immediately within 10-15 minutes.
Preparation
Sonography of the pancreas requires special preparation, on which the accuracy of the results depends.
- 72 hours before the planned examination, it is recommended to completely limit the consumption of protein-containing foods, as well as foods that contribute to increased gas formation (for example: fresh fruits and vegetables, carbonated juices or water).
- Fatty, salty, fried foods should be avoided.
- 24 hours before the ultrasound, you need to drink a laxative prescribed by your doctor.
- The patient should not eat 12 hours before diagnosis.
- Before the examination, you should not consume/drink liquids.
- On the day of the examination, you should not give your child antispasmodics or analgesics.
It is important to remember that the key to reliable results is careful preparation for the diagnostic procedure. In emergency cases, diagnosis is carried out without prior preparation.
Ultrasound and its implementation
Today, every child who has reached 12 months of age must undergo an ultrasound examination of the pancreas in order to timely recognize pathology and diagnose the disease.
Sonography is performed on an outpatient basis and does not require hospitalization of the patient. The examination is carried out using special medical equipment and gel, which promote better glide of the sensor.
To determine the size of the head, you need to take a lying position; to determine the size of the tail and body, you need to lie on your side. In some cases, the examination is carried out in a half-sitting position. The duration of the procedure is on average a quarter of an hour.
Important. Using ultrasound, the doctor can assess the size, contours and echogenicity of the organ.
Anatomical options
Anatomical abnormalities of the pancreas are classified as fusion abnormalities (pancreas divisum), migration of an abnormal ring-shaped pancreas (ectopic pancreas), or duplication abnormality (change in number or shape).
Division of the pancreas occurs as a result of disruption of the fusion of the ventral and dorsal primordia. The ventral (Wirsung) duct drains only the ventral bud of the pancreas, while most of the gland drains into the minor papilla through the dorsal (Santorini) duct.
The incidence is estimated to range from approximately 5 to 10% of the population. It is not often identified by sonography, although it can be easily recognized when the ducts are ectatic and also during pancreatitis (Fig. 8).
Figure 8 : Transverse epigastric ultrasound of the pancreas. Pancreas divisum: the dorsal pancreatic duct (arrow) is in direct connection with the duct of Santorini; The ventral canal of Wirsung (arrowhead) opens into the intestinal lumen. Note the enlarged head of the pancreas (dotted double-headed arrow) in acute pancreatitis.
Annular pancreas is a rare congenital anomaly characterized by pancreatic tissue that completely or partially covers the descending duodenum. The prevalence is approximately 1 in 2000 people. It is often associated with other congenital anomalies such as esophageal atresia, imperforate anus, congenital heart defects, midgut malrotation, and Down syndrome.
Two types have been proposed: an extramural subtype, where the ventral pancreatic duct surrounds the duodenum to join the main pancreatic duct, and an intramural subtype, where pancreatic tissue mixes with muscle fibers of the duodenal wall and numerous small ducts empty directly into the duodenum. . It can have a wide range of clinical severity and can affect neonates and the elderly, making diagnosis difficult.
About half of patients with neonatal duodenal obstruction may have a “double bubble” on abdominal x-ray if the obstruction is complete. This condition is difficult to confirm by ultrasound, but the rounded head of the pancreas and the proximal part of the duodenum passing through the head should raise suspicion. Magnetic resonance imaging (MRI) easily confirms the diagnosis; the latter imaging modality is preferred for assessing both the pancreas and ducts (Fig. 9).
Figure 9 : Transverse epigastric ultrasound of the pancreas. Annular pancreas: head of the pancreas surrounding the duodenum with normal peristalsis (top line a–c). The annular pancreas is clearly visible on MRI (bottom line).
Other possible diagnostic measures
Often, a doctor will prescribe a computed tomography scan of the pancreas. The procedure is carried out using iodine or a contrast agent to more accurately determine the structure of the organ. This diagnostic method is not recommended for use among patients/children who are allergic to iodine, so the attending physician should be warned about this in order to avoid undesirable consequences.
Important. A blood or urine test is often ordered to check for the presence of pancreatic enzymes (lipase, amylase and trypsin).
How to make an appointment with a doctor at home (details)?
The procedure for calling a doctor at home is quite simple: on the website you click on a special “house call” window, which displays a form for filling out information about the future patient. It includes:
- Patient's name.
- Telephone.
- The service you need to receive (select in the appropriate item). After this, you need to check the box to agree to the privacy policy. Soon you will receive a call from the right specialist.
After filling out the form and calling, the doctor arrives. In addition to the main ultrasound procedure, he will prescribe additional tests and studies for a complete clinical picture.
Ultrasound is an absolutely safe and modern method of examining internal organs. Moreover, it is the most accurate. A timely visit to a doctor will allow you to find out the condition of the internal organs for tumors and pathologies, and prevent the development of more dangerous diseases. Only highly qualified specialists work in the clinic. They will be able to give an accurate diagnosis and prescribe the correct treatment.
Causes of pancreas enlargement
Unfortunately, deviations from the norm are not always harmless; in some cases, an enlarged pancreas is a sign of pathogenic changes in an important organ of the digestive system. The pancreas can become enlarged due to swelling of the organ, pancreatitis, cyst, cancer, viral infection and impaired blood supply.
Pancreatitis
It is an inflammation of the pancreas. There are acute and chronic forms of the disease, and their symptoms are very different from each other.
Acute pancreatitis manifests itself:
- the patient's skin color may change;
- pulse becomes rapid;
- temperature rises to 38 degrees;
- attacks of nausea, vomiting;
- severe pain in the rib area;
- There is no appetite at all.
During an exacerbation of the chronic form of the disease, in addition to pain, vomiting, nausea and heartburn, the following symptoms are observed: bloating, flatulence, deterioration in general condition, weight loss.
Important. Treatment of pancreatitis is possible with the help of medications and diet. Sometimes the patient needs surgery.
Cancerous formations
It is characterized by severe pain, weight loss with normal appetite, nausea, vomiting, and fatty acids and neutral fats are excreted in the stool. Treatment requires surgery and chemotherapy. At the same time, symptomatic therapy is carried out.
Indications for abdominal ultrasound in children
In newborns and children of the first year of life:
- preventive examination to exclude congenital pathologies (especially in the case of difficult births);
- frequent regurgitation after eating;
- poor appetite;
- underweight;
- occasional diarrhea;
- bloating or asymmetry of the abdomen.
In preschool children and adolescents:
- pain or discomfort in the abdominal area;
- attacks of nausea and vomiting (especially with bile);
- frequent constipation or diarrhea;
- rapid weight gain or loss;
- complaints of foreign tastes and a feeling of bitterness in the mouth;
- bad breath.
An abdominal ultrasound can be performed on a child for the purpose of preventing and diagnosing diseases. In addition, the examination is mandatory if the child has suffered an injury to internal organs.
Special food
Often, after diagnosing an enlarged pancreas, the doctor recommends that parents monitor the child’s diet. Fried, smoked and fatty foods should be excluded from his menu. A child can consume vegetables and fruits only after heat treatment. It is necessary to give up sweets and fast food. The child's diet should consist of lean meats and fish. You can eat low-fat cottage cheese, crackers, and stale bread. An oven-baked apple is ideal as a dessert. The average duration of the diet is about six months, then you can gradually switch to a normal diet. Parents should carefully monitor the child’s diet, because the state of his health depends on it.