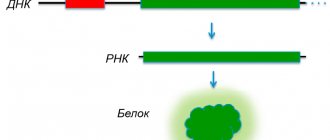
Gastrointestinal diseases often cause a feeling of abdominal discomfort, nausea, unpleasant belching and other symptoms, in addition, there are several factors that can cause poor health, and one of them is Helicobacter pylori.
Helicobacter pylori is an infectious bacterial disease that develops in the cavity of the stomach and duodenum. The infection can cause complications in the form of gastritis, ulcers and other diseases that are even life-threatening.
For what reasons does bacteria appear in the body?
Helicobacter is a bacterium
The bacterium does not develop in the open air, but passes from an infected person to a healthy person through household items, for example, plates, cups, spoons, etc., personal hygiene items, and also, importantly, the bacterium can be transmitted during a kiss.
The bacterium survives well in an acidic environment, so it easily enters the stomach and its mucous membrane, beginning to destroy all healthy tissue.
As a result of infection with this bacterium, a person may experience erosions, gastritis and all end with an ulcer, and if the disease is not detected early and treatment is not started, stomach cancer may develop.
People who do not take care of personal hygiene, lead a dirty lifestyle, etc. are susceptible to infection. Also at risk are those who live in dormitories, boarding schools, orphanages, and medical workers.
Next, you will learn about the symptoms of this disease, how helicobacteriosis is diagnosed and treated.
Modern treatment of Helicobacter pylori-associated peptic ulcer in children
T
An alarming fact is the increase in peptic ulcer disease in childhood. In addition to the significant improvement in diagnosis already in the early stages of the disease, there is, of course, a true increase in peptic ulcer disease, its complications and relapses.
Recognition of Helicobacter pylori (Hp) as one of the leading etiological factors in the development of destructive gastroduodenal pathology changes ideas about the pathogenesis of the disease and radically changes the tactics and strategy of treatment measures [1]. The experience gained over the past 10 years in treating peptic ulcers with anti-Helicobacter drug combinations has shown that after destruction (eradication) of HP in the gastric mucosa, peptic ulcer no longer recurs, i.e. “chronic recurrent suffering” itself disappears [2]. Numerous data obtained in many countries of the world indicate that relapses of peptic ulcer disease within 5 years occur in 5-10% of treated patients, usually due to Hp reinfection, and among patients who have not received anti-Helicobacter therapy, ulcers recur within 2 years in 100% [3].
It was these studies that contributed to the fact that in 1994 the American College of Gastroenterologists officially recommended the use of anti-Helicobacter therapy for the treatment of peptic ulcers. Significant progress has been made in the development of treatment regimens for the infection, a number of which are generally accepted and recommended at national and European levels [4]. However, anti-Helicobacter therapy remains to a certain extent individual and requires careful consideration when prescribing to each specific patient, especially if we are talking about a child.
The main list of drugs with anti-Helicobacter activity by WHO experts includes metronidazole, tinidazole, clarithromycin, amoxicillin, tetracycline and colloidal bismuth subcitrate
.
Bismuth preparations
were used to treat gastroduodenal diseases already in the 16th century; they became especially widespread in Germany and England for the treatment of dyspeptic disorders in the 19th century. When studying the effect of bismuth preparations in the treatment of peptic ulcers, it was discovered that their bactericidal activity against Hp is of decisive importance. This property is apparently associated with the bismuth cation and is found in various compounds: citrate, salicylate and bismuth nitrate [5]. Bismuth tripotassium dicitrate is a basic drug for anti-Helicobacter therapy, binds Hp, leads to a change in the structure and destruction of the microbe, weakens the action of Hp enzymes, which helps to increase the effectiveness of the body’s defenses against the bacterium. Existing strains of HP are not resistant to the drug, so bismuth tripotassium dicitrate solves the problem of primary and acquired resistance of HP to antibiotics. The bismuth drug forms a protective layer on ulcerated areas of the mucosa, protecting it from the effects of aggressive factors, promoting ulcer healing, and also inhibits the activity of pepsin. To date, it has been proven that the frequency of HP destruction with monotherapy is 30% [6]. This is due to the fact that bismuth, due to its physicochemical structure, is almost completely bound by gastric mucus, which is why, in the depths of the gastric pits, where a significant part of Hp is located, a high concentration of the drug is not created.
Ranitidine bismuth citrate is a new chemical compound, a blocker of histamine H2 receptors with a bactericidal effect on Hp. Suppresses basal and stimulated secretion of gastric juice, thereby reducing the volume and content of hydrochloric acid and pepsin in the secretion. Has a protective effect on the gastric mucosa. When sufficient clinical experience had been accumulated, it turned out to be advisable, given the established synergism, to combine therapy with a bismuth drug and antibiotics.
For effective treatment of gastroenterological diseases associated with Helicobacter pylori infection, the use of specific antibacterial drugs is necessary. Considering the ecological niche occupied by Helicobacter pylori, the antibacterial therapy must meet certain requirements, namely: the drugs used must have an effective effect on HP, be resistant to the aggressive acidic environment of the stomach, be able to penetrate under the layer of gastric mucus, and act locally in the mucosal area membranes, quickly excreted from the body without accumulating in other tissues and organs.
It has been established that the effect of antibacterial drugs on Hp is limited by the ability of this microorganism to live in the submucosal space. An antibiotic, entering the stomach, remains there for a short time, which, as a rule, is not enough for its activity against HP to manifest itself, and this often leads to HP resistance to this antibacterial drug.
Clarithromycin
- an antibiotic from the macrolide group. Blocks protein synthesis at the ribosomal level in bacterial cells, is active against HP. Refers to acid-fast antibiotics. The level of primary HP resistance to clarithromycin in Europe is 5-15%, which is apparently associated with the active use of this drug in the treatment of respiratory tract infections. In Russia, clarithromycin-resistant strains of Hp have not been identified, which is a consequence of the limited use of the drug in Russia.
Amoxicillin
belongs to the group of betalactam antibiotics, disrupts the synthesis of glycoproteins in the bacterial wall, has a bactericidal effect against HP, which increases significantly in a neutral environment. The level of HP resistance in Russia is 11%.
Tetracycline
has a bactericidal effect on HP due to the suppression of bacterial cell protein synthesis. HP resistance to the drug does not occur. Contraindication to the use of tetracycline is age less than 8 years. Given the pronounced side effects, it is used extremely rarely in pediatrics.
Metronidazole
, damaging the DNA of bacteria, inhibits their replication. It is the basic drug of various eradication schemes. Primary HP resistance to metronidazole in Europe is 50%, in Russia - 36%. The advantage of the drug is that its activity is not affected by the pH of the stomach.
Furazolidone
- a nitrofuran drug with anti-Helicobacter activity. Its use in combination with other antibiotics is justified by its synergism with respect to Hp. No Hp strains resistant to furazolidone have been identified. Most antibacterial drugs are able to exhibit maximum activity only at a neutral pH value. It has been proven that the minimum inhibitory concentration of furazolidone practically does not change when the pH of the environment changes.
The treatment program for patients with peptic ulcer disease associated with HP includes:
• teaching patients about diet and taking medications;
• assessment of the severity of the disease;
• development of an individual plan for a course of combination therapy;
• selection of drugs to prevent exacerbations and complications of the disease.
Therapy involves solving the following main tasks:
• eradication of HP;
• high-quality repair of the mucous membrane of the stomach and duodenum, including scarring of the ulcer;
• reducing the risk of relapse.
The experience we have accumulated in eradication therapy allows us to recommend the following regimens of anti-Helicobacter therapy.
In order to ensure effective eradication of HP in peptic ulcers, we use drug combinations of three drugs: bismuth-containing, metronidazole and furazolidone. We give preference to a short 7-day course of treatment, because with this duration, no side effects are observed and no situation arises requiring discontinuation of prescribed drugs.
For children under 7 years old we prescribe: bismuth tripotassium dicitrate 120 mg + metronidazole 250 mg + furazolidone 50 mg 2 times a day for 7 days.
For children over 7 years of age, the dosage of the drugs increases accordingly: tripotassium bismuth dicitrate 240 mg + metronidazole 500 mg + furazolidone 100 mg 2 times a day for 7 days.
If it is necessary to prescribe quadruple therapy, along with furazolidone, we use amoxicillin or clarithromycin in an age-specific dosage 2-3 times a day.
In cases where the patient is over 12 years old and has a high acid-forming function of the stomach, a regimen consisting of two drugs was used for eradication: ranitidine bismuth citrate 400 mg 2 times a day and clarithromycin 250 mg 3 times a day for 14 days.
In these regimens, instead of the listed antibiotics, spiramycin can be used at a dose of 1,500,000 IU 2 times a day; it is characterized by higher safety, has immunomodulatory and post-antibiotic properties. Cross-resistance Hp with erythromycin does not develop to spiramycin, as occurs with clarithromycin.
After completion of eradication therapy, to achieve high-quality healing of the ulcer and reduce inflammation of the mucous membrane of the stomach and duodenum, it is necessary to prescribe dual therapy with tripotassium bismuth dicitrate and metronidazole (for 14 and 7 days, respectively).
For duodenal ulcer in children, according to P.L. Shcherbakov, the most effective was the combination of the proton pump inhibitor omeprazole
(10 mg 2 times a day in children under 10 years of age and 20 mg 2 times a day in children over 10 years of age) and 2 antibiotics - amoxicillin 250/500 mg 2 times a day and clarithromycin 250 mg 2 times a day in within 7 days. As maintenance therapy after scarring of ulcers, bismuth tripotassium dicitrate 120 mg 2 times a day and metronidazole 250 mg 2 times a day for 10-14 days [7]. This regimen has no disadvantages, but to date there has been no approval from the Pharmacocommittee for the use of omeprazole and H2-blockers in pediatric practice. However, with a high acid-forming function of the stomach, a complicated course of chronic gastroduodenitis, recurrent acute erosions of the mucous membrane, the threat of transformation of erosive gastroduodenitis into a peptic ulcer, a complicated course of a peptic ulcer, the use of histamine H2 receptor blockers is indicated, in short courses with mandatory gradual withdrawal of the drug. It is necessary to know and take into account a wide range of side effects of antisecretory drugs - this is the “rebound” phenomenon, depletion of the periulcer zone and “immature” scar, lack of functional restoration of the mucosa, leading to increased relapses, etc.
In foreign publications, data have appeared that allows us to recommend omeprazole in pediatric gastroenterology for gastric and duodenal ulcers [8, 9]. The use of omeprazole (0.6 mg per 1 kg of body weight 2 times a day) for 2 weeks in combination with amoxicillin (30 mg/kg 2 times a day) and clirithromycin (15 mg/kg 2 times a day) led to eradication NR in 92% of patients. Ulcers healed in 100% of patients. Adverse reactions were mild and were observed in 23% of patients. There are no data on the use of lansoprazole or pantoprazole in children.
After scarring of the ulcers and successful eradication of HP, treatment is stopped. It is very difficult at present to talk about preventive treatment of various forms of chronic destructive gastroduodenal pathology associated with helicobacteriosis. Many gastroenterologists believe that high-quality eradication of HP will save the child from the disease forever. At the same time, the results of our studies indicate the need to use preventive treatment, primarily due to the risk of relapse of the disease.
Considering that endogenous intoxication of the body is a universal link in the pathogenesis of various diseases, and in the case of peptic ulcer disease it also affects the persistence of remission, therefore the prognosis of the disease depends on the effectiveness of detoxification. We have developed the following regimen: SUMS-1 at the rate of 0.5-1.0 g per kg of body weight in 2-3 doses 1.5 hours before meals daily (or algisorb 5 g 3 times a day) + derinat 3-5 ml intramuscularly every other day, duration of treatment is 10 days. Then de-nol 120 mg + metronidazole 250 mg 2 times a day for 10 days. In general, preventive course therapy lasts 20 days.
SUMS-1 is carbon deposited on a mineral matrix, an enterosorbent, developed in Russia and has no analogues abroad. SUMS-1 predominantly sorbs medium- and high-molecular toxins, microbial cells, and works effectively in all parts of the gastrointestinal tract. Unlike active carbons, it does not remove potassium, sodium, calcium ions, as well as vitamins and hormones from the body.
Algisorb is an enterosorbent created on the basis of a natural polysaccharide from seaweed, does not affect the balance of calcium in the human body, and is not absorbed in the gastrointestinal tract. Can be used for therapeutic and prophylactic purposes for a long period of time.
Derinat (sodium deoxyribonucleate) stimulates reparative processes, cellular immunity, leukopoiesis, phagocytic activity of neutrophils, nonspecific defense factors, and indirectly affects antiviral immunity. It is well tolerated by patients and has no side effects.
Imperfection of the digestive organs in children leads to the fact that true organic pathology is accompanied by severe multiple functional disorders. Most often, gastroesophageal and duodenogastric reflux are recorded with peptic ulcer disease, the modern correction of which involves several strategies. “Step up” is a step-by-step therapy with a transition from less strong to more powerful antisecretory drugs. They start with non-drug methods, then prescribe antacids. If symptoms of the disease persist, prokinetics are added. If there is no effect, H2 blockers or proton pump inhibitors are used [10].
“Step down” - treatment is immediately started with the most powerful antisecretory drugs, and when a clinical effect is achieved, they move on to antacid drugs for a course of 3-4 weeks, while maintaining recommendations for adherence to diet and lifestyle.
The problem of reducing the risk of relapse of the disease in children is very relevant, because HP reinfection can occur quickly in families where parents and immediate relatives suffer from various chronic diseases of the upper digestive tract, or are carriers of HP without clinical manifestations of the disease. In such cases, an endoscopic examination of all members of the child’s family living in the same apartment is indicated. If Hp carriage is detected in other family members, it is necessary to prescribe dual therapy with tripotassium bismuth dicitrate and metronidazole for 10-14 days, and if signs of a chronic gastroenterological disease are detected - the three-component regimen indicated above, in an age-appropriate dosage.
Commenting on the research results, I would like to emphasize once again that for the treatment of destructive lesions of the stomach and duodenum of Helicobacter etiology in children, there are various schemes with different durations of course combination therapy [11,12].
Treatment with the above drugs is sufficient for eradication of HP, persistent relief of clinical manifestations of the disease and the most complete restoration of the morphological structure of the mucous membrane. Literature:
1. Ivashkin V.T., Lapina T.L. Helicobacter pylori - from scientific research to clinical practice. Diagnostics and treatment.-1996.t.11 (12).-P.3-10.
2. Van der Hulst RWM, Keller JJ, Rauws EAJ, Tytgat CNJ Treatment of Helicobacter pylori infection: A review of the World Literature. Helicobacter. — 1996. -v.1. - p. 6-19.
3. Penston JGReview article: clinical aspects of Helicobacter pylori eradication therapy in peptic ulcer disease. Aliment. Pharmacol. Ther. -1996. -v. 10. - p. 469-486.
4. National Institute of Health. Consensus conference. Helicobacter pylori in peptic ulcer disease. JAMA. -1994. — v. 272. - p.65-69.
5. Marshall BJ, et al. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet .-1988:2 (8626-8627): 1437-1442.
6. Rauws EAJ, Tytgat GNJ Campylobacter pylori. - Amsterdam.- 1989.
7. Materials of the 7th session of the Russian group for the study of Helicobacter pylori. Nizhny-Novgorod.- 1998.-S. 31-33.
8. Dohil R., Israel DM & Hassal E. Ejective 2-Wk Therapy for Helicobacter Pylori Disease in Children. Am. J. Gastroenterol. 1997:92:244-47.
9. Kato S., Takeyama J., Ebina K & Naganuma H. Omeprazole-based Dual and Triple Regimens for Helicobacter Pylori Eradication in Children. Pediatrics 1997: 3: 124-25.
10. Tytgat GNJ., Janssens J., Reynolds JC & Wienbeck M. Update on pathophysiology and management of gastro-oesophageal reflux disease the role of prokinetic therapy. European Journal Gastroenterology & Hepatology 1996: 8: 603-1.
11. Zlatkina A.R. Pharmacotherapy of chronic diseases of the digestive system. M.: medicine, 1997.-240 p.
12. Zokirov N.Z. The role of Helicobacter pylori in gastroduodenal pathology of childhood. Pediatrics.-1.-1998.- From 76-82.
Omeprazole –
Losek (trade name)
(AstraZeneca)
How is Helicobacteriosis diagnosed?
To make a final diagnosis of helicobacteriosis, doctors prescribe the following studies of the patient’s body:
- Non-invasive tests;
- Blood tests;
- Exhaled air analysis.
- Biopsy. This analysis is done during endoscopy of the affected areas of the mucosa. Thanks to this procedure, doctors obtain information about the presence (absence) of bacteria in the patient’s mucosa. This procedure is accurate if tissue samples were taken from several inflamed areas at once.
These studies are inexpensive and quick to obtain results. But it should be noted that non-invasive tests often show false positive results.
And in order for the result of the analysis of exhaled air to be as truthful as possible, 14 days before the test you should not take antisecretory, anti-inflammatory and antacid drugs, also 3 days before the procedure you should not drink alcohol or eat legumes, and 3 hours before you should not smoke or chew chewing gum.
Problems of treating Helicobacter pylori infection
Once in the stomach, the bacterium produces urease, which breaks down urea in the gastric contents, resulting in the formation of ammonia and CO2. Ammonia helps protect the microbe from hydrochloric acid and causes damage to the gastric mucosa. By releasing the enzyme mucinase, H. pylori destroys the mucin protein contained in the gastric mucus, which creates conditions for the bacterium to penetrate through the mucus layer and adhere to the epithelium of the gastric mucosa. H. pylori also secretes other enzymes: catalase, oxidase, protease, phospholipase and vacuolating cytotoxin, which has a direct damaging effect on the epithelium of the gastric mucosa, increasing cell apoptosis. Enzymes stimulate lipid peroxidation, which contributes to the inflammatory process in the gastric mucosa. Inflammation of the mucous membrane is accompanied by infiltration of the lamina propria by neutrophils, plasma cells, lymphocytes, and macrophages. Neutrophil infiltration is stimulated by the secretion of interleukin-8, which is produced by epithelial cells in response to H. pylori. This effect is most pronounced in the pathogenesis of chronic atrophic gastritis and ulcer in Cag A and Vac A strains of the bacterium [2, 4, 7]. Therefore, anti-inflammatory and anti-Helicobacter therapy is justified for any disease associated with H. pylori. The main principle of treatment of the above diseases is eradication therapy, the indications of which are determined by the Maastricht consensus in 1996 and its revisions in 2000 (“Maastricht II”), 2005 (“Maastricht III”) and 2010 (“Maastricht IV” ) [16]. In addition to the indications for eradication therapy, according to Maastricht III, in addition to the main diseases, there are conditions after gastric resection for stomach cancer, as well as the prescription of treatment for persons who are first-degree relatives of patients with stomach cancer, and persons infected with H. pylori without clinical manifestations, at the request of the patients. In addition, it is possible to carry out anti-Helicobacter therapy for diseases such as gastroesophageal reflux disease, functional dyspepsia, long-term use of non-steroidal anti-inflammatory drugs and unexplained iron deficiency anemia with the obligatory presence of H. pylori [11, 20, 21, 24]. Depending on the degree of Helicobacteriosis identified during histological examination of a biopsy specimen from the antrum of the stomach during gastroduodenoscopy, various eradication therapy regimens are recommended: 3- or 4-component for 7, 10 or 14 days [6, 8, 11, 21]. The first line of anti-Helicobacter (eradication) therapy includes several options. The first option is a proton pump inhibitor (PPI): omeprazole 20 mg twice a day or esomeprazole 20 mg twice a day, or lansoprazole 30 mg twice a day, or pantoprazole 40 mg twice a day, or rabeprazole 20 mg 2 times/day; amoxicillin 500 mg 4 times/day or 1000 mg 2 times/day in combination with clarithromycin 500 mg 2 times/day. The second option includes PPIs in the same doses, antibiotics amoxicillin and clarithromycin in the above doses and tripotassium bismuth dicitrate 120 mg 4 times / day or 240 mg 2 times / day. The third option - in the presence of atrophic gastritis with achlorhydria, the regimen does not contain a PPI, and includes amoxicillin 500 mg 4 times / day in combination with clarithromycin 500 mg 2 times / day + bismuth tripotassium dicitrate 240 mg 2 times / day. The fourth option is recommended for older people for whom standard anti-Helicobacter therapy is limited. The regimen includes a standard dose of PPI + amoxicillin + tripotassium bismuth dicitrate or a short course of PPI + tripotassium bismuth dicitrate – 28 days (IV Moscow Agreement) [7]. The second line of anti-Helicobacter therapy includes: the first option - PPI in standard doses, tripotassium bismuth dicitrate 240 mg 2 times / day, metronidazole 500 mg 3 times / day and tetracycline 500 mg 4 times / day. The second option is PPI in a standard dosage, amoxicillin 500 mg 4 times / day or 1000 mg 2 times / day, bismuth tripotassium dicitrate 240 mg 2 times / day and furazolidone 100 mg 4 times / day. The Maastricht III recommendations suggest prescribing quadruple therapy as the first line of treatment for helicobacteriosis and extending the treatment period to 14 days. At the same time, the effectiveness of eradication increases by 12% [4, 8]. In our country, there is increasing resistance to clarithromycin and metronidazole due to the fact that the above drugs are widely prescribed for other inflammatory diseases. This has led to the search for new alternative regimens, as well as to an increase in the duration of therapy [9, 14]. However, the Maastricht guidelines suggest retaining clarithromycin in 3- and 4-drug regimens if the incidence of clarithromycin-resistant H. pylori is less than 15–20%. In case of resistance in a larger percentage of cases, it is recommended to replace the drug with another antibiotic - levofloxacin 500 mg 2 times / day. According to the standards for the diagnosis and treatment of acid-dependent and H. pylori-associated diseases (IV Moscow Agreement), clarithromycin can be replaced with rifaximin 400 mg twice a day or josamycin 1000 mg twice a day [4, 7]. If resistance to metronidazole occurs in less than 40% of cases, the Maastricht recommendations suggest leaving metronidazole in any of the regimens or replacing it with furazolidone. If the percentage of resistance is higher, the drug is excluded from all treatment regimens and replaced with drugs of the nitrofuran series - furazolidone or nifuratel (IV Moscow Agreement, 2010). The third line of the Maastricht recommendations is that treatment is selected after determining the sensitivity of H. pylori to antibiotics. "Maastricht IV" offers another eradication option - sequential 10-day therapy: PPI + amoxicillin - 5 days, then the next 5 days PPI + clarithromycin + metronidazole. The remaining eradication regimens are 3-component and quadruple therapy without the drug bismuth tripotassium dicitrate or with it in the same doses with a treatment duration of 7 to 14 days [2]. The quality of anti-Helicobacter therapy is monitored after 4–6 weeks. after completion of treatment. If H. pylori is detected, repeated courses of treatment with replacement of the proton pump blocker and antibiotic are recommended. Properly selected anti-Helicobacter therapy made it possible to reduce the progression of chronic gastritis and the frequency of relapses of gastric ulcers and its complications: bleeding, perforations, penetrations and malignancy of gastric ulcers. However, there are also negative aspects of these eradication treatment regimens. This is primarily an increase in H. pylori resistance to antibiotics, the appearance of hypersensitivity reactions to antibiotics and other drugs in treatment regimens, and disruption of the intestinal microbiocenosis. Problems associated with the treatment of H. pylori infection include unsatisfactory eradication rates and/or the development of side effects of treatment [9, 14]. Antibiotic-associated diarrhea (AAD) is one of the most common complications. According to statistics, AAD is observed in 5–30% of patients receiving antibiotics. The term “antibiotic-associated diarrhea” refers to otherwise unexplained diarrhea that developed in connection with the prescription of antibiotics (during their use or in the first 2 months after the end). The range of clinical manifestations of AAD is wide: from pseudomembranous colitis to mild diarrhea. Complications of pseudomembranous colitis can include toxic megacolon, intestinal perforation, sepsis, which in some cases requires colectomy. The greatest risk of developing AAD is observed when taking amoxicillin with clavulanic acid and cefixime. Ampicillin, amoxicillin, clindamycin, lincomycin, cephalosporins of the second and third generations are the drugs that most often cause AAD associated with Clostridium difficile [18]. In addition, Clostridium perfringens, Staphylococcus aureus, Candida spp., Klebsiella oxytoca, Salmonella spp. are discussed as etiological factors of AAD. Unfortunately, not only antibiotics play an important role in the development of diarrhea syndrome when H. pylori eradication therapy is prescribed. In recent years, a direct relationship has been proven between the suppression of hydrochloric acid and the increasing risk of intestinal infection. Despite the undoubted positive role of PPIs and other antisecretory drugs in the treatment of pathology of the esophagogastroduodenal zone, there is also a flip side to the coin - the possibility of developing complications of this therapy, one of which is the risk of bacterial infections (pneumonia, Clostridium difficile AAD and other variants of infectious gastroenteritis). It has been proven that hypochlorhydria caused by long-term use of PPIs can lead to bacterial colonization of the upper gastrointestinal tract and thereby affect the composition of the eubiotic microflora of the small intestine [19, 25]. The vegetative form of Clostridium difficile survives in the stomach when pH levels increase, which explains the high risk of bacterial colonization of the small intestine in patients taking PPIs. This is supported by the finding that the likelihood of developing Clostridium difficile colitis and its severity are similar in animals treated with PPIs or antibiotics. In recent years, given the threat of developing AAD, probiotics have been prescribed during eradication therapy for H. pylori infection for prophylactic purposes and to reduce the symptoms of diarrhea. Data from meta-analyses of studies of the effectiveness of probiotics conducted in 2010–2011 showed that the use of this group of drugs significantly accelerates the recovery of patients in the treatment of diarrhea of various origins, incl. AAD. A reduction in the incidence of AAD occurs when probiotic components are taken at a dose of more than 5 billion CFU/day. An analysis of more than 11 thousand publications and the results of 622 clinical studies confirmed the effectiveness of taking probiotics in adults during treatment with antibiotics, incl. and in eradication therapy regimens for H. pylori infection. The latest revision of Maastricht IV already considers the use of pre- and probiotics as promising: statement 12 of the “Treatment” section: “The use of some pro- and prebiotics as adjuvant therapy has shown promising results in terms of reducing the incidence of side effects.” In clinical practice, in most cases, probiotics containing bifidobacteria, lactobacilli, and Saccharomyces boulardii are used [22, 23]. In dynamics, clinical symptoms and the composition of fecal microflora are assessed mainly. Researchers explain the positive role of probiotics from the perspective of ensuring colonization resistance, an immunomodulatory effect, as well as the possibility of relieving osmotic diarrhea while taking antibiotics, and optimizing the function of the intestinal epithelium. At the same time, the issue of the survival of probiotic microorganisms in the gastrointestinal tract, their biocompatibility with indigenous microorganisms, their effect on the immune system of the body as a whole, and their resistance to antibiotics has not been resolved. In this regard, it seems important to study the safety of probiotics and the contribution of each component of this class of immunobiological drugs. In recent years, evidence has been obtained that the main active component of the restoration of intestinal microflora in dysbiotic conditions is the waste products of probiotic microorganisms - their metabolites. Success in the treatment of recurrent Clostridium difficile diarrhea was also obtained as a result of a new original manipulation - transplantation of intestinal microbiota - administration of a suspension of feces from healthy donors through a duodenal tube, which turned out to be more effective than treatment with vancomycin. In experiments on conventional white mice with experimental AAD, the influence of components of feces of healthy mice when administered per os and per rectum was studied. The most pronounced stimulating effect of restoring intestinal microflora was exerted by an orally administered filtered suspension of feces containing microbial metabolites. Thus, a promising direction in the correction of dysbiosis, prevention and treatment of AAD is the use of drugs – metabolite probiotics [16, 17]. From this perspective, the domestic synbiotic Baktistatin is of interest - a complex combination of pro- and prebiotic components. One of the main active principles of Bactistatin is the composition of Bacillus subtilis metabolites (bacteriocins, lysozyme, catalase), which have a bactericidal and bacteriostatic effect on pathogenic and opportunistic microorganisms. In addition, microbial metabolites have an immunomodulatory effect and optimize the state of the intestinal microbiota. The second component of Baktistatin is a natural sorbent zeolite, which ensures the sorption and elimination of toxins, normalizes intestinal motility, and is an additional source of microelements. Soy flour hydrolyzate as part of the complex is an additional source of protein and amino acids that helps restore the intestinal biocenosis. The effectiveness of the use of Baktistatin in eradication therapy regimens for H. pylori infection has been proven by domestic clinicians [12, 26]. A positive effect of the drug on the intestinal microflora, antibiotic tolerance, as well as the success of eradication therapy were noted [3]. The possibility of prescribing Bactistatin from the first day of antibiotic therapy is also significant, since the drug is resistant to its action. When eradication treatment was carried out without the inclusion of a synbiotic, disturbances of intestinal microbiocenosis were observed significantly more often [12, 13]. Thus, the use of Baktistatin is promising in the prevention of one of the most common complications of eradication therapy - AAD, which allows us to hope for the successful treatment of H. pylori infection. Literature 1. Bugaeva I.O., Grechushnikov V.B. and others. Helicobacter pylori: modern diagnostics and therapy. Saratov, 2008. 105 p. 2. Vyalov S.S. Peptic ulcer and Maastricht-4: implementation in clinical practice // Effective pharmacotherapy. Gastroenterology. 2012. No. 6. pp. 16–23. 3. Zaitseva E.V., Antonenko O.M. The place of dysbiosis correction in the treatment of a number of chronic diseases of the digestive tract // Consilium medicum. Gastroenterology. 2011. No. 1. pp. 60–63. 4. Ivashkin V.T., Sheptulin A.A., Lapina T.A. Chronic gastritis caused by Helicobacter pylori infection: diagnosis, clinical significance, prognosis. A manual for doctors. RGA. M., 2009. 23 p. 5. Isakov V.A., Domoradsky I.V. Helicobacteriosis. M.: Medpraktika-M, 2003. 411 p. 6. Lazebnik L.B., Vasiliev Yu.V. et al. Helicobacter pylori: prevalence, diagnosis, treatment // Experimental and clinical gastroenterology. 2010. No. 2. P. 3–7. 7. Lazebnik L.B., Bordin D.S. and others. Chronic gastritis. Guidelines. M.: TsNIIG, 2011. 34 p. 8. Lapina T.L. Eradication therapy of Helicobacter pylori // Medical Bulletin. 2006. No. 6. P. 9–10. 9. Maev I.V., Vyuchnova E.S. and others. Side effects of modern anti-Helicobacter therapy // Clinical medicine. 2002. No. 6. P. 7–12. 10. National Guide to Gastroenterology / ed. Ivashkina V.T., Lapina T.L. M.: GEOTAR-Media, 2008. 704 p. 11. Samsonov A.A., Maev I.V. Modern standards of diagnosis and treatment of diseases associated with Helicobacter pylori. (analysis of materials of the 3rd Maastricht Agreement) // Medical Bulletin. 2006. No. 4. P. 358. 12. Tkachenko E.I., Avalueva E.B. and others. Eradication therapy including probiotics: consensus on effectiveness and safety // Clinical nutrition. 2005. No. 1. P. 14–20. 13. Uspensky Yu.P., Baryshnikova N.V. Global trends towards expanding the use of probiotics: the relevance of using products based on Bacillus subtilis // Consilium medicum. Gastroenterology. 2012. No. 1. pp. 40–44. 14. Khomeriki N.M., Khomeriki S.G. Some mechanisms for the development of side effects of anti-Helicobacter therapy and ways of correction // Consilium medicum. Gastroenterology. 2005. T. 7. No. 2. P. 12. 15. Tsukanov V.V. Clinical and epidemiological aspects of Helicobacter pylori // Experimental and clinical gastroenterology. 2006. No. 1. P. 24–25. 16. Chicherin I.Yu., Pogorelsky I.P., Darmov I.V. Intestinal microflora: abstracts about the main thing. M., 2013. 21 p. 17. Chicherin I.Yu., Pogorelsky I.P. and others. Transplantation of intestinal microbiota // Journal of Infectology. 2013. No. 2. P. 2–15. 18. Clostridium difficile: an old bug with new tricks? //DDW Clostridium difficile Symposium. 2007. May. 31 p.m. 19. Leonard J. Systematic review of the risk of enteric infection in patients taking acid suppression // American Journal of Gastroenterology. 2007. Vol. 102(9). P. 2047–2056. 20. Malfertheiner P., Megraud F. et al. Current concept in the management of Helicobacter pylori infection: the Maasticht III - 2000 Consensus report // Gut. 2007. Vol. 56. P. 772–781. 21. Scaccianoce G., Hassan C. et al. Helicobacter pylori eradication with either 7-day or 10-day triple therapies, and with a 10 – day sequential regimen // Can. J. Gastroenterology. 2006. Vol. 20(2). P. 113–117. 22. Szajewska H. et al. Meta-analysis: the effects of Saccharomyces boulardii supplementation on Helicobacter pylori eradication rates and side effects during treatment // Alimentary Pharmacology and Therapeutics. 2010. Vol. 32. P. 1069–1079. 23. Simren M., Dore J. Gut microbiota for health – current insights and understanding // European Gastroenterology & Hepatology Review. 2012. Vol. 8. P. 3–7. 24. Vaira D., Zullo A. et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: a randomized trial // Ann Intern Med. 2007. Vol. 146(8). P. 556–563. 25. Yang Y., Metz. D. Safety of proton pump inhibitor exposure // Gastroenterology. 2010. Vol. 139. P. 1115–1127. 26. Baryshnikova N.V. Clinical and microbiological characteristics of intestinal microbiocenosis and correction of its disorders in patients with chronic gastroduodenitis associated with Helicobacter pylori: Abstract of thesis. diss. ...cand. honey. Sci. St. Petersburg, 2006. 24 p.
How to treat Helicobacter pylori?
Diagnosis of Helicobacter: blood test
The bacterium Helicobacter pylori is a very living microorganism that is able to survive in acidic conditions, has a disgusting effect on the human immune system, namely, it blocks the ability of white blood cells (leukocytes) to destroy harmful living organisms. And in order to recover from this parasite, it is necessary to undergo a course of antibacterial therapy.
The process of destroying these bacteria in the body has its own name - “eradication”, and consists of several schemes. During treatment, different medications belonging to different groups of action are prescribed. Antibacterial treatment has three lines, which we will tell you about.
Signs of the disease
The content of the article
The main signs of the disease and its symptoms:
- nausea and vomiting;
- heaviness in the stomach;
- belching;
- frequent heartburn;
- pain in the stomach;
- hunger;
- prolonged discomfort;
- diarrhea or constipation.
Most people become infected with this bacterium in the first years of their lives, it is transmitted through dirty hands, hygiene items, even by kissing, the bacteria Helicobacter pylori can be transferred. While this microorganism is inactive, it does not pose a particular threat to human health. But, as soon as some malfunctions appear in the body’s functioning, this bacterium begins to become active and causes a destructive effect, the stomach and duodenum are especially susceptible to its effects. Under its influence, gastritis and stomach ulcers develop. Erosion is formed, which causes pain and discomfort to a person.
2.1 how to treat
There is no clear answer to the treatment of Helicobacter pylori. Some are inclined to believe that it needs to be treated, others are against its complete elimination from the body. But, of course, self-prescribing medications is out of the question.
Treatment should be prescribed by a doctor, after a full medical examination, with all the necessary tests, and based on the complete picture, the doctor must make a decision on treatment. Basically, treatment involves the prescription of antibiotics, in combination with other drugs that will have a healing and restorative effect on the walls of the stomach. Diet is also a necessary condition for successful treatment; food should be light so as not to cause sudden changes in increase or decrease in acidity. At the end of treatment, a second full diagnosis is carried out to ensure the correctness of the treatment and its success.
Often, having discovered a bacterium, it is suggested that all family members be tested in order to exclude this bacterium from them. If a microorganism is nevertheless detected in family members, then they are all prescribed complex treatment, mainly with first-generation antibiotics. After 1-2 months, repeat tests are carried out, and based on their results, treatment is stopped or a second course is prescribed using stronger drugs.
2.2 Eradication therapy
The most effective treatment method is eradication therapy, which involves the use of several drugs simultaneously, with different effects. Of course, you can’t do without an antibiotic, but in addition to it, medications are prescribed that have an effect on the body’s digestive system, improve and speed it up, use enzymes to quickly break down food, thereby reducing the load on the digestive organs. There is less reflux of bile into the stomach to break down food, and due to this, the mucous membrane is less irritated. By prescribing drugs that have an enveloping effect, ulcers and erosions on the gastric mucosa are healed, pain and discomfort gradually go away. Naturally, it is necessary to properly restore and strengthen the body’s microflora through the use of probiotics and prebiotics. With their help, the patient's normal stool will be restored.
2.3 tests that must be taken to detect the bacteria:
- blood from a vein;
- breath test;
- stool analysis;
- saliva analysis;
- smear analysis for FGS;
In fact, it is not necessary to take the entire series of tests listed above. Basically, doctors prescribe blood from a vein, a breath test and a test for FGS.
A blood test will only show the presence of antibodies to bacteria of this type, and if its indicators are slightly deviated in one direction or another, then another analysis will have to be carried out to make sure.
The most reliable analysis is a smear, which is taken when examining the stomach from its walls, during fibrogastroscopy (FGS). Another similar method is to break off a piece of mucous membrane during endoscopy and examine it under a microscope for cytology. There can no longer be a mistake; the laboratory assistant sees a bacterium. There cannot be any deviations or errors, such as in a blood or stool test.
What can happen if you ignore this disease?
Antibacterial drugs - against Helicobacter
First of all, it is worth mentioning that it is absolutely forbidden to engage in independent treatment for helicobacteriosis!
The symptoms of this bacterial infectious disease are very similar to a number of other diseases that may be completely unrelated to the gastrointestinal tract.
Medicines, dosage and duration of treatment are determined solely by the results of tests and studies, and exclusively by a qualified doctor.
But it is worth noting that in advanced cases, even the most highly qualified and experienced doctor may not help, and especially if the disease was advanced before cancer developed.
Therefore, if you experience symptoms associated with a gastrointestinal disease, consult a doctor, undergo special examinations, and if Helicobacter pylori is present in your body, begin treatment.
Doctors have proven the fact that if one family member is infected, the probability that other family members are also sick is 95%.
Treatment regimen for Helicobacter pylori: all modern methods of eradication therapy
TREATMENT SCHEME FOR HELICOBACTER PYLORI: ALL MODERN METHODS OF ERADICATION THERAPY
To identify Helicobacter pylori, a urease breath test is used, which does not require much time, is harmless and does not cause any discomfort, and is the gold standard for diagnosing the infection. Symptoms and treatment of Helicobacter pylori vary from person to person. The presence of a pathogen in the body is not always accompanied by pathological processes and requires taking medications.
To clarify and agree on the best approaches to identifying and treating Helicobacter pylori infection in Europe, a group of leading gastroenterologists was formed. Periodically, based on conferences and meetings, they publish protocols - the Maastricht Consensus, named after the city where the first meetings took place.
There are currently five of them:
* Maastricht 1 (1996, Maastricht); * Maastricht 2 (2000, Maastricht); * Maastricht 3 (2005, Florence); * Maastricht 4 (2012, Florence); * Maastricht 5 (2016, Florence).
According to the results of the Maastricht 2 consensus, it was found that, unfortunately, none of the eradication regimens being carried out, despite the simultaneous use of several drugs, guarantees complete destruction of the infection. In this regard, it was recommended to treat patients first with a “first-line” regimen, and then, in the absence of a therapeutic effect, with a “second-line” regimen.
The need for repeated courses of anti-Helicobacter therapy is explained by the increased resistance of H. pylori to prescribed antibiotics, which is the main problem of modern gastroenterology in the treatment of diseases associated with the pathogen.
Penetration of the pathogen into the gastric mucosa
The eradication regimens used today to cure Helicobacter pylori infection were approved at Maastricht 4.
The main requirements for them are:
* ensuring at least 80% of cases of cure from infection, healing of gastritis or ulcers, confirmed by repeated research; * duration of therapy is no more than 14 days; * acceptable low toxicity of the drugs used; * safety, side effects in less than 15% of patients; * no serious side effects requiring early discontinuation of the pills; * accessibility and convenience for patients, a small number of doses of medicine for Helicobacter pylori per day; * overcoming the ever-increasing resistance of bacteria to antibiotics used; * the possibility of replacing drugs within the regimen if allergic reactions or other problems are identified.
Interesting: Historically, the first successfully tested Helicobacter pylori eradication regimen was the use of bismuth subsalicylate and Metronidazole. It was tested by scientist Barry Marshall, who together with a colleague discovered Helicobacter pylori in the gastric mucosa. In 1984 he deliberately drank the contents of a Petri dish containing a culture of bacteria, and then, shortly after the appearance of the characteristic symptoms of provoked gastritis, carried out the indicated treatment. After 14 days of therapy, according to the results of a biopsy, no pathogen was found in the stomach.
First line drugs
The goal of first-line eradication therapy is to eliminate H. pylori in as many patients as possible./div> According to the Maastricht 3 recommendations, a so-called three-component regimen (triple therapy) is prescribed, which includes the following drugs and dosages per day:
* proton pump inhibitor (PPI) twice in standard doses; * antibiotic Clarithromycin 0.5 g twice; * antibiotic Amoxicillin 1 g or antibacterial agent Metronidazole 400 or 500 mg twice.
As PPIs that reduce the secretion of gastric juice and the secretion of hydrochloric acid, patients are treated with the following drugs in the indicated dosages per dose:
* Lansoprazole – 30 mg; * Pantoprazole – 40 mg; * Esomeprazole, Omeprazole or Rabeprazole – 20 mg.
The minimum duration of treatment is 7 days. According to a number of clinical studies, it turns out that it is more effective to take these drugs for 10 or 14 days. In order to achieve maximum eradication of Helicobacter pylori and eliminate the likelihood of relapses, triple therapy, in the absence of contraindications and other restrictions, must be prescribed in full, both in dosage and duration of treatment.
The three-drug regimen can be used as first-line therapy in countries where the incidence of clarithromycin-resistant H. pylori strains is less than 15–20%. The development of pathogen resistance to Clarithromycin is explained by the frequent prescription of macrolide antibiotics for bacterial complications of ARVI and respiratory diseases in children and adults. If resistance to Clarithromycin is found on average in 10% of the population, then for Metronidazole this figure is much higher and ranges from 20 to 40%, which significantly limits the possibility of using this antibacterial agent.
As an alternative to three-component eradication therapy, a four-component regimen can be used, additionally including bismuth tripotassium dicitrate (the drug De-Nol) 120 mg 4 times a day. If a patient with a diagnosed Helicobacter pylori infection has atrophy of the gastric mucosa, accompanied by a lack of hydrochloric acid production, then there is no need to prescribe PPIs in this case, so they are excluded, leaving bismuth tripotassium dicitrate.
For elderly patients in whom, due to the high risk of complications when prescribing two antibiotics at once, full first-line anti-Helicobacter therapy is impossible, the following abbreviated treatment regimen for 14 days is recommended:
* Amoxicillin; * any IPP; * bismuth salt preparation.
If indicated in elderly patients, the antibiotic may be completely discontinued.
In this case, bismuth preparations are prescribed for 28 days; in case of pain, a short course of PPI is additionally prescribed. 12/26/2021theadmin