Infiltrative gastric cancer is a morphological form of carcinoma, which is characterized by infiltrative growth (growth through the wall of the organ) and the absence of clear tumor boundaries.
- Causes
- Who is at risk
- General clinical manifestations
- Forms of pathology
- Stages of the disease
- Diagnostics
- Treatment options
- Forecast
- Prevention measures
Features of infiltrative cancer:
- It is characterized by a high degree of malignancy - it grows quickly and metastasizes early.
- May occur in young people.
- The hereditary factor is clearly visible.
- As a rule, it manifests with symptoms of dyspepsia.
Causes
The causes of the infiltrative form of gastric cancer are not fully known. The risk factors are believed to be similar to other forms of gastric carcinoma:
- Chronic atrophic gastritis. More than half of patients with stomach cancer were diagnosed with atrophic gastritis. In this case, its localization matters. If the body of the stomach is affected, the risk of cancer increases by 3-5 times, the antrum - by 18 times, and if signs of atrophic gastritis are found throughout the stomach, the risk of developing a malignant neoplasm increases by 90 times.
- Poor nutrition and eating unhealthy foods. This includes constant overeating, frequent consumption of marinades, smoked meats, dried, salty and spicy foods, an excess of animal fats and heat-treated fats in the diet.
- Hereditary predisposition. For infiltrative gastric cancer, the hereditary factor can be traced much more clearly than for other forms of malignant neoplasms of the stomach. This is also supported by the fact that the tumor is often diagnosed in young patients.
- Drunkenness and alcoholism.
- Smoking.
- Helicobacter pylori infection.
Book a consultation 24 hours a day
+7+7+78
Features of infiltrative tumors
The diagnosis of infiltrative stomach cancer (adenocarcinoma) is made when a malignant neoplasm is detected that has grown into the wall of the organ. The distinctive features of this form of oncopathology are the rapid growth of altered tissues and the early spread of metastases.
This type of stomach cancer has other characteristics.
Among them:
- high concentration of aggressive malignant cells (foci are located at a distance of about 7 cm from each other);
- pronounced density of the neoplasm;
- clear dependence on heredity.
The infiltrative formation consists of clusters of malignant cells independent from each other. They do not have clear boundaries, spread easily, and “capture” healthy tissue completely. The stomach walls harden, peristalsis is disrupted, and the organ falls out of the digestive process.
Who is at risk
The following patients are at increased risk of cancer:
- With chronic atrophic gastritis.
- With a chronic stomach ulcer, especially if it is large. Malignant transformation can occur at any stage of peptic ulcer disease.
- People with a family history of stomach cancer.
- Patients who have undergone gastric surgery within the last 10 years.
- Patients with congenital and acquired immunodeficiencies.
- Workers employed in hazardous working conditions, in particular in nickel, asbestos production, rubber, chrome production, etc.
- Patients with sessile polyps.
The above categories of people are recommended to undergo timely medical examinations with fibrogastroduodenoscopy and taking a biopsy from pathological lesions. A morphological examination of the biopsy specimen determines the presence of morphological changes: cell atypia, structural changes in the tissue of the mucous membrane, etc. Such changes should be regarded as precancer and appropriate treatment should be carried out.
General clinical manifestations
Stomach cancer in the early stages does not have typical manifestations. If there are symptoms, they are nonspecific and can be present in a huge number of other diseases:
- Changes in the patient’s general condition—increased fatigue, unknown weakness, decreased performance.
- Mood disturbances, even depression - apathy, alienation, loss of interest in life.
- Perversion of appetite, for example, aversion to certain foods (most often meat and fish).
- The phenomena of “gastric discomfort” are a feeling of heaviness or fullness in the stomach, belching, lack of physiological satisfaction from eating.
- Pain in the epigastrium or under the breasts.
In common forms of infiltrative gastric cancer, the clinical picture is more typical and detailed:
- Stomach pain. In 70% of patients, pain is constantly present, or occurs for no apparent reason, and intensifies after eating.
- Anorexia is loss of appetite.
- Sharp weight loss.
- The symptoms of anemia are pallor and pasty skin.
- Satiety from eating a small amount of food. A common symptom in diffuse cancer, as it impairs the ability of the stomach wall to stretch.
- Nausea and vomiting. The infiltrative form of stomach cancer disrupts the motility of the organ and prevents the passage of the food bolus. Food accumulates, rots and ferments, causing nausea and vomiting. In some cases, patients themselves induce it to relieve painful symptoms.
- Increased appetite. This is a casuistic symptom that is characteristic only of infiltrative pyloric cancer. The tumor turns it into a gaping tube through which food quickly leaves the stomach, and the feeling of fullness does not occur.
Kinds
There are the following degrees of differentiation of tumor cells in infiltrative breast cancer:
- Gx – it is not possible to determine the degree of differentiation;
- G1 – highly differentiated malignant tumor;
- G2 – moderately differentiated neoplasm;
- G3 is a poorly differentiated malignant tumor.
- G4 – undifferentiated malignant process.
There are several types of infiltrative breast cancer:
- Infiltrative lobular;
- Edema-infiltrative;
- Ductal;
- Infiltrative nonspecific type.
Infiltrative lobular cancer is found in the upper part of the breast in older women.
It occurs in 10% of cases of infiltrating breast cancer. Oncologists distinguish two types of edematous-infiltrative breast cancer: primary (diffuse) and secondary (nodular). Infiltrative ductal breast cancer affects most older women. The diagnosis of “infiltrative nonspecific breast cancer” is established when the differentiation of neoplasm cells is difficult. The following nonspecific forms of infiltrative cancer are distinguished: mucinous cancer, squamous metaplasia, poorly differentiated tumors.
Make an appointment
Stages of the disease
There are 4 stages of infiltrative gastric cancer, depending on how deeply the tumor has grown and whether it has metastasized.
- Stage 0 is cancer in situ, in which malignant cells are found in the mucous layer of the stomach wall, or there is severe mucosal dysplasia.
- Stage 1 - the tumor grows into the mucous and submucosal layers of the gastric wall, metastases are detected in 1-2 lymph nodes, or the cancer spreads to the muscular layer of the gastric wall, but there is no evidence of metastases.
- Stage 2 - the tumor grows into the wall of the stomach, reaches its serous membrane and can even grow into the tissue surrounding the stomach. Damage to 7 or more lymph nodes is detected.
- Stage 3 - the tumor extends beyond the stomach, affecting the visceral peritoneum, nearby organs (spleen, large intestine, liver, diaphragm, etc.), metastases are detected in 10-15 lymph nodes.
- Stage 4 - distant metastases are detected in internal organs and lymph nodes.
Book a consultation 24 hours a day
+7+7+78
Complications
Infiltrative ductal tumor of the mammary gland quickly spreads to the skin of the affected breast, nearby tissues, and lymph nodes.
In the ductal form of a malignant tumor, the skin over the tumor, the fatty layer of the axillary region, lymph nodes, and surrounding tissues are involved in the pathological process. Atypical cells migrate to muscles and bones. Metastases spread to the liver, lungs, kidneys, adrenal glands, and brain. When the lymph nodes in the axillary region on the side of the tumor are affected, the outflow of lymph from the vessels of the upper extremities to the main lymphatic collectors is disrupted, lymphostasis develops, and the motor ability of the arm is impaired. Often, several years after treatment, relapses of infiltrative breast cancer occur.
Diagnostics
Unfortunately, early diagnosis of infiltrative gastric cancer is often difficult, since the tumor has endophytic growth and does not manifest itself in any way during a visual examination of the mucosa during an endoscopic examination.
To detect a tumor and make a diagnosis, the following research methods are used:
- Fibrogastroduodenoscopy. Allows you to examine the gastric mucosa under magnification and take a biopsy from suspicious lesions. As we have already said, for infiltrative cancer this method has a rather low information content (about 65%). And the presence of a tumor can mainly be suspected by indirect signs.
- X-ray of the stomach with contrast. Infiltrative cancer may not be visually detected on the mucous membrane, however, it affects the wall of the stomach, which leads to a decrease in the volume of the organ, impaired peristalsis, and a change in the density of the walls. These changes will be clearly visible when performing radiography with contrast. This research method allows detecting a tumor in approximately 90% of cases, but it is absolutely ineffective at the initial stage of the disease.
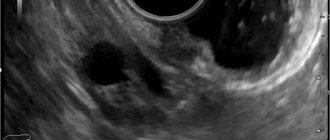
- Ultrasound of the abdominal cavity and retroperitoneal space. This method allows you to determine the degree of invasion of stomach cancer, its spread beyond the stomach wall and detect damage to the abdominal organs, pelvis and regional lymph nodes.
After the diagnosis is made, a clarifying examination is carried out, which is necessary to clarify the stage of the disease and select the optimal treatment regimen. For this purpose, the following procedures are carried out:
- Tests for tumor markers CEA, CA 19-9, CA 72-4. From a diagnostic point of view, determining these markers does not make sense, since they can remain at normal levels even at stage 3 of the disease. However, if initially exceeded, they can be used to monitor treatment and detect relapse of the disease.
- CT and/or MRI with intravenous contrast. They are an alternative to ultrasound and are used to determine the stage of cancer in economically developed countries. The method allows you to detect metastases in the organs of the abdominal cavity, retroperitoneum, pelvis, and also detect changes in the lymph nodes.
- Gynecological examination in women and digital rectal examination in men. This examination allows you to detect metastases of stomach cancer to the ovaries (Krukenberg metastasis), pararectal lymph nodes (Schnitzler metastases).
- X-ray of the chest cavity. It is carried out to detect metastases in the lungs and pulmonary lymph nodes, as well as damage to the pleura.
Individually, according to indications, diagnostics can be supplemented by the following studies:
- Endosonography - transesophageal ultrasound. It is carried out during planning for surgical removal of cancer, when there is evidence of its spread to the esophagus and diaphragm. This study will detect the upper border of the tumor and plan the extent of the operation.
- Ultrasound and biopsy of cervical, supraclavicular and axillary lymph nodes - detection of Virchow and Irish metastases.
- Colonoscopy.
- PET-CT.
- Osteoscintigraphy.
- Bone marrow biopsy if metastases are suspected.
- Diagnostic laparoscopy. It is mandatory for total and subtotal tumor lesions of the stomach, as well as cancer growth beyond the serous membrane of the stomach.
Symptoms of the disease
At the initial stages of adenocarcinoma development, infiltrative oncopathology is asymptomatic. The signs that appear first are nonspecific and are characteristic of many diseases.
Among them:
- fast fatiguability;
- mild pain in the area under the breast;
- apathy;
- belching;
- weakness;
- depressed mood;
- feeling of heaviness in the stomach, fullness of the stomach;
- decreased performance;
- change in food preferences (more often there is an aversion to meat and fish).
A pronounced clinical picture appears when the disease develops into an irreversible stage.
Among the main symptoms of infiltrative oncopathology:
- reducing the acidity of gastric juice to critically low values;
- regular vomiting, nausea;
- bloating;
- flatulence;
- epigastric pain not associated with stomach fullness;
- heartburn;
- yellowness of the skin, mucous membranes;
- the presence of blood in stool, vomit, saliva;
- deterioration of appetite (with pyloric adenocarcinoma, on the contrary, it increases), saturation with a small amount of food against the backdrop of filling the organ cavity with adenocarcinoma tissues;
- anemia;
- sudden weight loss;
After nutritional correction, negative symptoms can be smoothed out. However, the effectiveness of the diet is short-term, the negative manifestations of adenocarcinoma development quickly return.
The diffuse-infiltrative form of cancer is characterized by spasmodic acute pain after eating, which is not relieved by painkillers. A distinctive feature of this type of neoplasm is also difficulty swallowing (dysphagia).
Treatment options
The main treatment method for infiltrative cancer is surgery. For common forms of neoplasm, it is supplemented with chemotherapy. If surgery is not indicated, only chemotherapy is performed.
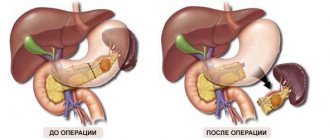
Surgery
When treating infiltrative forms of gastric cancer, the following types of operations are used:
- Gastrectomy.
- Subtotal gastrectomy.
In this case, the affected part of the stomach or the entire stomach is removed en bloc with the surrounding tissues, which includes the greater and lesser omentum, fatty tissue and regional lymph nodes of the 1st-2nd order. The intersection of the organ in case of infiltrative cancer is carried out no less than 7 cm from the defined edge of the tumor. To confirm the radicality of the operation, the removed fragment is immediately examined for the presence of tumor cells at the cutting edges.
If cancer spreads to neighboring organs, the scope of the operation may increase and include resection of the affected tissue.
Chemotherapy
Chemotherapy can be used as part of a combination treatment, in conjunction with surgery, or as a stand-alone treatment for unresectable tumors.
The following types of chemotherapy are used as part of combination treatment:
- Perioperative. This type of treatment involves 3 cycles of chemotherapy for 8-9 weeks before surgery, then diagnostic tests are performed, and if there are no signs of unresectable surgery and 3 cycles of chemotherapy after it. The regimens used are CF - cisplatin fluorouracil, and ECF - epirubicin, cisplatin, fluorouracil. This treatment can increase 5-year disease-free survival and generally prolong the life of patients with advanced gastric cancer.
- Adjuvant chemotherapy. This treatment is prescribed 4-6 weeks after surgery if no complications have arisen. Oral forms of fluoropyrimidine are used for 12 months or the XELOX (CAPOX) regimen for 6 months. If the tumor is HER-2 positive, treatment may be supplemented with trastuzumab.
For unresectable forms of stomach cancer, chemotherapy is the main treatment method. As the first line of therapy, regimens including platinum drugs and fluoropyrimidines are prescribed. Three-drug regimens that are supplemented with docetaxel improve overall survival but are more toxic. Therefore, they are prescribed only to healthy patients. If there are bone metastases, bisphosphonates (zoledronic acid) may be prescribed.
The first line of chemotherapy is carried out for 18 weeks, after which the patient is observed until the disease progresses. If it occurs within 3 months after the end of first-line chemotherapy, second-line drugs (taxanes) are used; if more than 6 months have passed after progression, first-line drugs can be used again. With a positive HER2 status, treatment is supplemented with targeted drugs.
In weakened elderly patients with concomitant diseases, gentle treatment is prescribed, and when their condition improves, they switch to the XELOX regimen. Symptomatic treatment is indicated for severely ill patients.
Radiation therapy
Radiation therapy is not used as an independent treatment method. For some time in the United States, adjuvant chemoradiation therapy was the standard of care for locally advanced forms of infiltrative cancer. But prospective studies have shown that this tactic does not improve the prognosis of patients, and the treatment is more toxic compared to adjuvant chemotherapy. Therefore, this approach is not currently recommended.
The main use of radiation therapy is palliative treatment to relieve symptoms of the disease. For example, it is used in the presence of bone metastases to reduce pain.
Symptomatic treatment
The following categories of patients are subject to symptomatic treatment:
- At stage 4 of the disease.
- Patients with locally advanced unresectable forms of cancer.
- Patients with severe concomitant pathology that makes it impossible to perform surgery or use cytostatics.
Symptomatic therapy is aimed at alleviating the patient’s condition and combating complications:
- Elimination of bleeding - often stomach tumors are complicated by heavy bleeding. Patients, in this case, experience vomiting of bloody or scarlet blood, melena in the stool. Endoscopic operations are performed to stop bleeding.
- Combating tumor stenosis - various technologies are used here, from stenting to bypass anastomoses and gastrostomy removal below the site of the lesion.
- Treatment of pain - drug therapy, regional anesthesia, radiation therapy.
- Treatment of ascites is intra-abdominal chemotherapy, laparocentesis, and installation of drainage.
Treatment
If a mass formation is detected in the mammary gland, the mammologist at the Yusupov Hospital conducts a comprehensive examination of the patient.
The doctor makes the decision on the treatment method after analyzing the results of all studies. Therapy for infiltrative breast cancer consists of several methods. They are used depending on the type and stage of tumor development, the age and general condition of the patient, and the presence of concomitant pathology. Surgeons at the Oncology Clinic take an individual approach to choosing the method of surgical intervention. Oncologists at the Yusupov Hospital prefer minimally invasive operations, after which the mammary gland is preserved. The breast is removed when other methods cannot save the patient's life. Before and after surgery, hormonal, radiation and chemotherapy are carried out.
Prevention measures
Methods for preventing infiltrative cancer are the same as for other malignant neoplasms of the stomach:
- Optimization of nutrition - avoiding overeating, balanced nutrition with sufficient dietary fiber and vitamins.
- Quitting smoking and alcohol abuse.
- Use of personal protective equipment when working with industrial hazards.
- Regular adequate examination of people at risk.
| More information about the treatment of stomach cancer at Euroonco clinics: | |
| Treatment of stomach cancer | |
| Oncologist-gastroenterologist | RUB 5,100 |
| Chemotherapy appointment | RUB 6,900 |
| Emergency oncology care | from 12,100 rub. |
| Radiologist consultation | RUB 11,500 |
Book a consultation 24 hours a day
+7+7+78