Is an anechoic inclusion in the uterus dangerous and what is it? These are polyps that may have malignant potential, and are essentially localized hyperplasia of the endometrium, that is, the inner lining of the uterine cavity. As a rule, they are located singly, but in 20% of cases there are multiple structures. They can have a wide base or a narrow vascular pedicle and occur in any part of the organ. They often have no symptoms and are an incidental finding during ultrasound diagnostics, for example, during pregnancy. May cause abnormal uterine bleeding.
What is echogenicity?
In order to understand what the anechoicity of the gallbladder may indicate, you need to understand the definition and properties of ultrasound. Some facts that will help you understand the essence of ultrasonic waves:
- Ultrasound is elastic vibrations of particles of a medium that propagate in the form of a longitudinal wave.
- It can exist in liquid, gaseous or solid media, but ends up in a vacuum.
- Some animals use it as a means of communication, but it is not inaudible to the human ear.
It is used in the diagnosis of internal diseases due to its properties. Ultrasound waves are absorbed by soft tissues and reflected from inhomogeneities.
The process of obtaining an image from an ultrasound machine occurs in two stages:
- radiation of a wave into the tissue being examined;
- receiving reflected signals, on the basis of which an image of internal organs is formed on the screen.
Due to the different structure and density of tissues and internal organs, they reflect ultrasound waves differently. In addition, this property also changes in various pathologies, which makes it possible to identify many diseases, including the gallbladder. To describe the resulting image, special terminology is used, which should be familiar not only to ultrasound specialists, but also to general practitioners.
Echogenicity is the ability of a tissue or organ to reflect an ultrasound beam. Different organs appear lighter or darker on the screen, and this property is determined precisely by their echogenicity.
Based on this feature, several types of fabrics can be distinguished:
- hyperechoic objects (bones, gas, collagen) are structures that reflect a large number of ultrasound rays and appear on the screen as bright white foci;
- hypoechoic (soft tissues) - partially reflect the ultrasound beam, are different shades of gray;
- anechoic (fluid) are areas that do not reflect ultrasound and appear as black lesions.
From this we can conclude that the anechoic contents in the gallbladder are liquid. To make a diagnosis, you need to understand how this organ should normally look on an ultrasound and what the presence of fluid in its cavity may indicate.
The accuracy of the results depends on the quality of the equipment and the sensitivity of the sensors
What are the risk factors for the appearance of large tumors in the pelvis?
The list of such factors depends on the nature of the neoplasm. For example, more than 80% of cases of ovarian torsion occur in women with large ovaries (more than 5 cm). The risk of fibroid formation increases with:
- the woman is over 50 years old;
- early onset of menstruation;
- use of oral contraceptives under 16 years of age;
- increase in body mass index.
Malignant neoplasms often have a genetic predisposition, and the likelihood of their occurrence increases if such pathologies are present in the family. In addition, risk factors for cancerous lesions are endometriosis, postmenopausal hormone therapy, obesity, high stature, and old age.
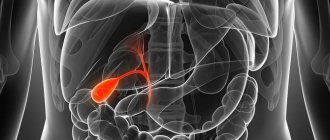
What does the gallbladder look like on an ultrasound scan normally?
The gallbladder is pear-shaped. There are 3 main elements in its structure:
- bottom - a wide edge that protrudes slightly beyond the liver;
- the body is its main part;
- neck - narrowing of the bladder at its exit.
The gallbladder is a hollow organ; it has a wall and a cavity where bile accumulates. Like other similar organs, it is built of muscle tissue, which is lined inside with a mucous membrane with a large number of folds and glands. On the outside, it is partially covered with a serous membrane.
The need for a reservoir for bile arose due to the fact that it does not enter the intestines constantly, but only during the digestion process. Ultrasound diagnostics are carried out on an empty stomach (even drinking water before the examination is prohibited) so that bile accumulates in the bladder and it is possible to examine its contents and walls.
Bile is produced in the liver and flows down the hepatic duct into the gallbladder. If there is an immediate need for it, it moves further along the bile duct into the duodenum. If this is not necessary, the sphincters contract and do not release bile from the bladder. Until food reaches the stomach, it will accumulate in the gallbladder and stretch its walls. As soon as the digestion process begins, the muscles of the bladder walls contract, and the muscles of the sphincter and bile duct, on the contrary, relax. Therefore, during an ultrasound after eating, the bladder will be empty, and it will not be possible to accurately determine its size and the nature of the contents.
Normally, the gallbladder indicators will be as follows:
- pear-shaped;
- dimensions: 8-14 mm in length, 3-5 mm in width;
- the location is intrahepatic, only the bottom of the bladder extends beyond the liver;
- the contours are smooth and clear;
- wall thickness - up to 3 mm;
- homogeneous anechoic contents.
Any deviations from the norm indicate the presence of pathology. Thus, the walls of the bladder thicken during inflammatory processes, and the abnormal structure of the bladder will impede the outflow of bile, and it will accumulate in its cavity in large quantities. The contents are examined if gallstones and other diseases are suspected; in such cases it becomes echogenic.
The gallbladder is a kind of bile sac that, when full, has the shape of a pear.
What are the types of neoplasms in the reproductive organs?
- ectopic pregnancy, in which a fertilized egg implants outside the uterus;
- an abscess in the uterine tube or ovary, which occurs with inflammatory and infectious diseases of the pelvic organs;
- endometrioma - benign ovarian cyst;
- leiomyoma (fibroids) is a benign gynecological tumor;
- Ovarian torsion is an acute gynecological situation with impaired blood supply to the ovary;
- cancerous tumors.
Echogenicity of the gallbladder contents
The gallbladder is a reservoir for bile. Apart from this, there can normally be no liquid in the cavity of the bladder. If the contents cease to be echogenic, that is, a uniform black color, this suggests the presence of foreign objects.
According to the nature of changes in echogenicity, they can be:
- focal (helminths, stones);
- diffuse (sediment, pus or blood).
The gallbladder and biliary tract can be a site for parasite infestation. Such diseases are more often diagnosed in childhood. Ultrasound shows thickening and inflammation of the walls, stagnant processes due to blockage of the ducts by helminths, as well as the parasites themselves in the form of light echogenic inclusions. Such studies are carried out on the basis of clinical signs: general deterioration of health, indigestion, yellowness of the skin and mucous membranes. After taking antiparasitic drugs, the picture normalizes, and the contents of the bladder become anechoic.
Stones play a leading role in gallbladder diseases. They can have different origins, chemical compositions, shapes and sizes, and look different on ultrasound. In composition, they can be cholesterol, calcareous, pigmented and complex (of mixed origin). It is impossible to determine this with an ultrasound; tests must be carried out after the stones are removed.
Based on the results of ultrasound diagnostics, several types of stones are distinguished:
- weakly echogenic;
- medium echogenicity;
- highly echogenic;
- stones that provide general acoustic shadow.
Weakly echogenic stones have a loose structure; most often they turn out to be cholesterol. Such formations are easily destroyed by special preparations, and the treatment process is monitored over time using ultrasound. Such stones must be distinguished from gall bladder polyps and cholesterol plaques, so during the procedure the patient changes his body position. If the stones remain in the cavity of the bladder and float in its contents, then the polyps attach to the walls and do not change location.
Stones of medium and high echogenicity are most often pigmented or calcareous. They look like bright light spots in the cavity of the bladder and are not difficult to diagnose. When examined with a highly sensitive sensor, you can find that they cast a shadow.
During the examination, the patient must change body position if foreign inclusions are found in the cavity of the gallbladder
A separate stage of cholelithiasis is the formation of stones that create a general acoustic shadow. This picture is observed in the presence of one large stone or many small ones that completely block the lumen of the gallbladder. The image can be confused with gases, which will also appear as light spots. For a more complete picture, you can give the patient two yolks to drink and repeat the study. When the digestion processes start, the gases will disappear, and the stones will remain in the cavity of the gallbladder.
Diffuse changes in echogenicity are rare. These include various sediments, pus or blood - substances that reflect ultrasound rays and are distributed evenly, mixing with bile. They can be recognized by the following characteristics:
- The sediment is located in the lower part of the gallbladder in an even layer, and above it there is normal anechoic bile.
- If there is pus in the cavity, it will initially look like sediment. The only difference is that when the patient changes position, it mixes with bile. In a chronic purulent process, it can form characteristic partitions in the cavity of the bladder, which are visible on ultrasound.
- Blood also needs to be differentiated from sediment and other diffuse inclusions. Over time, it coagulates and forms weakly echogenic clots that resemble stones or polyps in appearance.
In the cavity of the gallbladder, echogenic inclusions may be detected, which then turn out to be neoplasms. Their difference is that they grow from the wall and do not move when the patient’s position changes. Tumors can be benign and not grow through the walls. If a patient is diagnosed with a malignant tumor, this means that it affects all layers of the gallbladder. Over time, the organ ceases to be detected on ultrasound due to necrosis of its wall.
Concrements (stones) look like light formations of various shapes and sizes
How are such disorders diagnosed?
The doctor makes a diagnosis based on:
- studying medical history;
- thorough collection and analysis of complaints;
- results of the patient's examination;
- general and extended blood and urine tests;
- laboratory and instrumental examinations, among which transvaginal ultrasound plays a leading role;
- specific examinations (computer and magnetic resonance imaging, cytohistological examination of biopsy materials) for the diagnosis of uterine cancer and other malignant lesions.
Not all of these neoplasms pose a danger to a woman’s life. For example, inflammatory lesions and cysts almost never lead to the development of cancer and often require only conservative treatment and careful medical supervision.
On the other hand, it is extremely important to know the signs of acute gynecological pathologies that require immediate medical attention. These include ovarian torsion and ectopic pregnancy. The latter can be suspected if the pregnancy test is positive, and the woman complains of pain in the abdomen or pelvic area and vaginal bleeding. Ovarian torsion is manifested by sudden severe pain on the affected side, which is accompanied by nausea and vomiting.
Rules for performing ultrasound of the gallbladder
In order for the research results to be as reliable as possible, it is better to start preparing in advance. At the initial examination, the doctor will set a date for the examination and tell you how to properly prepare for it. The exception is in emergency cases when there is a risk of blockage of the bile ducts with stones or urgent surgery is required.
For a routine ultrasound, the patient should adhere to a few simple rules:
- a week before the ultrasound, exclude from their diet alcohol, fatty foods and those that cause increased gas production (carbonated drinks, yeast bread, raw fruits and vegetables, legumes);
- It is recommended to start taking medications (Mezim, Espumisan and the like) 3 days in advance;
- Before the test, you should not eat for 8 hours.
If the ultrasound is scheduled for the first half of the day, you should skip breakfast and water. Dinner the day before should be no later than 19.00. If the procedure will be carried out in the evening, you can have breakfast around 7 am.
Anechoic contents in the gallbladder are normal. It means that the bladder is filled with bile, in which there is no sediment or foreign substances. This is an important factor in the diagnosis of helminthiases, cholelithiasis and other pathologies. Ultrasound of the gallbladder is also included in a routine examination of the abdominal cavity. In addition to this indicator, attention is paid to the size and shape of the organ, the thickness and uniformity of its walls. The indicators are written on a form and given to the attending physician, who then interprets them based on clinical signs.
Summary
Not all mass tumors in the pelvic area are malignant, and they do not always require immediate intensive treatment. An important role here is played by high-quality diagnostics, which makes it possible to find out the nature of such a neoplasm and its exact localization.
You should also not neglect regular preventive examinations by specialists. Doctors at the Anadolu Clinic have extensive knowledge in the field of diagnosis and use advanced and effective treatment methods in their practice.
The material was prepared in agreement with Anadolu doctor, professor obstetrician-gynecologist Murat Dede.
results
Of the 92 patients with metastatic malignancies of non-gynecological origin included in this study, 39 (42.4%) were diagnosed surgically and 53 (57.6%) by biopsy. All of them underwent ultrasound examination in our department and raised suspicions about the presence of tumor metastases of non-gynecological origin in 75 (81.5%) of them. The tumor marker CA 125 was elevated (35 Code/L) in 47 patients (51.1%). The mean marker value in these patients was 83.2 code/L (range, 41.2-438.4 code/L).
Among metastatic non-gynecological tumors, colorectal cancer is by far the most common histological type, detected in one third of patients. The types and frequencies of individual tumors are shown in Table 1.
| Diseases | Quantity (%) |
| Colorectal cancer | 32 (34,8) |
| Tumors of the upper digestive tract (pancreas, gallbladder) | 13 (14,1) |
| Lymphoma | 11 (11,9) |
| Krukenberg tumor (gastric cancer metastases) | 9 (9.8) |
| Mammary cancer | 6 (6.5) |
| Gastric stromal tumors | 4 (4,3) |
| Bladder cancer | 3 (3.3) |
| Neuroendocrine tumors | 2 (2,2) |
| Carcinoid tumors | 2 (2,2) |
| Malignant mesotheliomas | 1 (1,1) |
| Malignant Schwannoma | 1 (1,1) |
| Primitive neuroectodermal tumor | 1 (1,1) |
| Liposarcoma | 1 (1,1) |
| Leiomyosarcoma | 1 (1,1) |
| Ewing's sarcoma | 1 (1,1) |
| Thyroid cancer | 1 (1,1) |
| Perimircytoma | 1 (1,1) |
| Atypical retroperitoneal leiomyoma | 1 (1,1) |
| Pseudomyxoma abdominis (malignant) | 1 (1,1) |
Other
Gastrostromal tumors
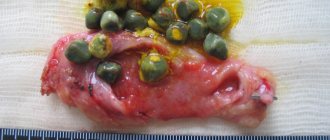
were observed in four (4.3%) patients. The tumor size ranged from 7 to 10 cm. All tumors were located intraperitoneally. In half of the cases the tumor was located in the ovary; in each case there was unilateral localization. In all cases, the structure was multilocular-dense with hyperechoic septa, hypoechoic necrotic areas and anechoic contents of the tumor chambers. The septa were often incomplete and hypervascular. The width of the septa and pseudosepta ranged from 5 to 10 mm (Fig. 7).
Fig.7. Metastases of a tumor of the gastrointestinal tract: visualized as a formation with several hyperechoic incomplete septa (1) and hypoechoic contents (2).
Bladder cancer metastases
were found in three (3.3%) patients. The tumor size ranged from 5 to 10 cm. All tumors were intraperitoneal, intraovarian and unilateral with a multilocular structure and heterogeneous septa. The number of chambers was always less than 10, the width of the partitions varied, with necrotic areas and blurred edges (Fig. 8). The solid component was necrotic with rich peripheral vascularity.
Fig.8. Metastases of bladder cancer: a tumor with blurred edges, with hyperechoic septa of varying widths (arrow).
Metastases derived from neuroendocrine tumors
were seen in two (2.2%) patients. The tumors were 8 and 10 cm in diameter. Both tumors were intraperitoneal, unilateral, and located in the ovaries. The structure was dense, heterogeneous and mostly hypoechoic (Figure 9). Vascularization was of moderate intensity. The tumors had blurred boundaries and were mobile. Both patients had hypoechoic liver metastases; no carcinomatosis or ascites was observed.
Fig.9. Metastases of neuroendocrine tumors: solid heterogeneous structure, mainly hypoechoic contents (calipers).
Two (2.2%) patients had carcinoid metastases
. Tumors are 3 and 5 cm in diameter. Both tumors were unilateral and localized to the ovaries. They were hard (solid) heterogeneous, with multiple small hyperechoic foci (Fig. 10). Subjectively, the tumor was hypovascular.
Fig. 10. Carcinoid metastases: a solid tumor is well defined, with a heterogeneous structure and hyperechoic foci (arrows).
Krukenberg tumor (metastatic gastric cancer only)
Krukenberg's cancer was characterized as an ovarian tumor of heterogeneous echostructure, with predominantly isoechoic and hypoechoic areas, as well as the potential appearance of necrosis (Fig. 5) with an uneven internal contour, but with a smooth surface. Vascularization of Krukenberg tumors (outside the area of potential necrosis) was assessed as hypervascularized.
Fig.5. Krukenberg tumor (gastric cancer metastases): a hard (solid), with an uneven internal surface and a smooth surface, heterogeneous tumor that is mainly isoechoic, but hyperechoic (1) and hypoechoic (2) areas are visualized.
Evaluation of the data obtained
Our assessment was carried out retrospectively by reviewing surviving examination reports. In case of uncertainty or lack of clarity in the report, stored still images or video clips were used for clarification, without knowledge of the histological diagnosis.
Tumors with metastases in the ovaries were designated as ovarian cancer. If the tumor was limited to the ovarian surface only, with no ovarian stroma involved, it was classified as ovarian with carcinomatosis. Tumors that were attached to the pelvic wall and supplied by the external, internal, or common iliac artery or tumors located clearly beneath the parietal peritoneum were classified as retroperitoneal. Heterogeneous, avascular areas of mixed echogenicity with blurred boundaries adjacent to vascularized tissue were classified as areas of probable necrosis (Fig. 1).
Fig.1. Necrosis: A heterogeneous avascular area with irregular edges (arrow) surrounded by tissue that has a blood supply.
The elasticity of the tumors was assessed by pressure, which was performed using a vaginal sensor with simultaneous pressure on the abdominal wall during palpation (in order to avoid tumor movement), and was classified as elastic or rigid.
The mobility of tumors was assessed by their movement in relation to adjacent structures when the examiner's hand presses on the abdominal wall while scanning with a transvaginal or abdominal ultrasound probe. A tumor is considered mobile when it moves freely along its entire perimeter in relation to neighboring structures. Semi-fixed - if it is securely fixed to at least part of its perimeter or neighboring structures have not shown any slip. Fixed - if it was completely motionless.
Colorectal cancer metastases
Typical signs of colorectal cancer metastases were: the round shape of the caudal part of the tumor, the presence of papillary growths and the presence of necrosis of the solid part. The tumors were predominantly with hyperechoic septa, mainly with hypoechoic or heterogeneous solid parts. Existing papillary growths, from isoechoic to hyperechoic, growing from thin septa and being specific for colorectal cancer metastases, were observed in 5/32 (15.6%) tumors (Fig. 2).
Fig.2. Metastases of colorectal cancer: multilocular solid tumor with a typical round shape (2) with papillary growths from the septa (1).
Wall thickness, calcification and structure
The wall thickness is 2-4 mm, the contours are smooth. Any thickening of the walls indicates pathological changes. It is caused by various reasons.
- A diverticulum (protrusion) of the wall leads to the fact that urine first comes out of the body of the bladder, and only then from the diverticulum. If urine remains in the pouch, the pouch becomes inflamed, leading to local thickening of the wall.
- The bladder is susceptible to a parasitic disease such as schistosomiasis. It is caused by fluke parasites that lay eggs in the walls of the organ. The larvae die, but fibrosis occurs at their location - the proliferation of connective tissue, leading to thickening of the walls.
- If there are problems with the prostate gland, stagnation of secretion occurs, and against this background, foci of calcification form on the walls of the bladder. An advanced infection leads to the fact that the body begins to fight it itself, enclosing it in a calcium shell.
- With age, the structure of the muscular membrane of the organ changes, it becomes deformed and stretched.
Tumors also increase the thickness of the walls. Cancerous tumors have uneven contours, they are abundantly supplied with blood vessels, and are characterized by increased echogenicity. Benign tumors are round or oval in shape and are not supplied with blood.
Ultrasonography
Each patient underwent both transabdominal and transvaginal or transrectal ultrasound examination, which was performed by one of two specialists in the field of ultrasound diagnostics in gynecological oncology, using GE Logiq 9 (USA). Description based on a standard protocol for the evaluation of pelvic masses. Sonograms and video clips created during the examination were stored electronically.
- Location
– ovaries
-outside the ovaries (intraperitoneal, retroperitoneal)
- Localization
-one-sided
-two-sided
-central
- Size (measured in three sizes)
- Size of hardest component (if any) (measured in three sizes)
- Accommodation
-pelvic
-pelvic and extrapelvic
- Structure
-dense
-single-chamber-dense
-multi-chamber-dense
-single-chamber
-multilocular
- WITHOUT papillary growths (yes/no)
- Echogenicity
-anechoic
- hypoechoic
-isoechoic
-hemorrhagic
-mixed
- Heterogeneous solid part (if any) (yes/no)
- Vascular features of the hard part (if possible)
- Subjective flow assessment (1-4) 11
-peak systolic velocity
-pulsation index
-resistance index
- Surface
-smooth
- serrated
- Elasticity
-flexes when pressed
-hard
- Mobility
-mobile
-semi-fixed
-fixed
- Multi-camera (if possible)
-number of cameras (1-5; 6-10; > 10)
-size of cameras
- Partitions (if possible)
-thickness
-uniformity of the thickness of the partition
- Subjective flow assessment (level 1-4)
- Suspicion of necrosis (yes/no)
- Does not extend to the body of the uterus (yes/no)
- NO ascites (yes/no)
- NO parenchymal metastases (yes/no)