Mortality from malignant tumors remains high, despite the increased capabilities of modern medicine. Colorectal cancer ranks fourth among cancer diseases in Russia. Thanks to the latest diagnostic equipment, doctors at the Oncology Clinic of the Yusupov Hospital conduct screening tests to identify the disease at an early stage of the tumor process.
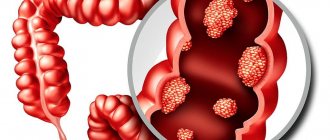
The large intestine has five sections. The tumor can form in the cecum, rectum, sigmoid, ascending and descending colon. The most common type of colorectal cancer is rectal cancer. If there is a small colon tumor, patients may not be bothered by any symptoms for several months. As the tumor process progresses, patients turn to proctologists or gastroenterologists. After a comprehensive examination, patients are advised by oncologists at the Yusupov Hospital. If the malignant nature of the neoplasm is confirmed, the doctors at the oncology clinic collectively determine the tactics for managing the patient.
Causes of colon tumor
Researchers have identified the following main causes of colorectal cancer:
- Genetic predisposition;
- Elderly age. After 55 years of age, the likelihood of developing a malignant tumor in the colon increases;
- Chronic inflammatory diseases in the large intestine;
- Excessive consumption of fatty foods, foods with refined carbohydrates;
- Metabolic diseases;
- Polyps in the colon;
- Low physical activity. When the balance between physical activity and the amount of calories consumed is disturbed, excess body weight occurs;
- Urbanization. Colorectal cancer is typical for industrialized countries, which experts associate with the nature of nutrition;
- Tobacco smoking;
- Chronic alcoholism.
A malignant tumor of the large intestine develops over 12-15 years. This disease is characterized by late detection, which reduces the likelihood of a favorable outcome. Modern high-precision diagnostic equipment used by oncologists at the Yusupov Hospital allows the patient to quickly identify the pathological process.
Microsatellite instability in colorectal cancer
Oncologists have proven that microsatellite instability in colorectal cancer is the cause of the development of the disease in 5% of cases. Microsatellite instability is characterized by the tendency of DNA to mutation under the influence of various factors. The medical literature describes two pathways for the development of genetic instability. The first mechanism for the development of colorectal cancer is associated with chromosomal abnormalities.
Malignant tumors of the colon, when the second pathway is activated, are associated with disruption of the repair process. Mutations occur spontaneously in the body; damage to DNA molecules can be caused by chemical reagents or physical factors. During the repair process, enzymatic systems contribute to the restoration of DNA sections.
Microsatellite instability in colorectal cancer is characterized by the presence of several genes in the DNA, mutations of which cause phenotypic abnormalities. The medical literature describes in detail the mechanism of development of colorectal cancer under the influence of mutations, which allows specialists to determine the most effective methods of therapy.
Difficulties in diagnosing colon cancer are due to the fact that the disease in different parts of the large intestine is due to different reasons. Treatment of colorectal cancer is based on the results of comprehensive diagnostics, which is a mandatory element of care for patients with colon cancer at the Yusupov Hospital. The oncology clinic employs highly qualified specialists. They provide assistance even to those patients who were abandoned by other medical institutions.
Cancer of the rectosigmoid junction, treatment stages 1, 2, 3. Symptoms, signs, metastases, prognosis.
The rectosigmoid junction is a transition zone between the sigmoid and rectum at a distance of 13 to 17 cm from the anal line during rigid rectoscopy.
Epidemiology
In civilized, economically developed countries, colorectal cancer is one of the most common malignant tumors.
In the structure of cancer incidence in the world, colorectal cancer currently ranks fourth. Every year, about 800 thousand newly diagnosed patients with colorectal cancer are registered in the world, more than half of them (440 thousand) die. Colorectal cancer causes death in approximately 3.4% of the general population and is the second leading cause of death in the United States.
In the European population, the risk of developing colorectal cancer is 4–5%. This means that one in 20 people will develop cancer of this location during their lifetime.
Although all economically developed countries have seen a steady increase in the incidence of colorectal cancer, nevertheless, this indicator is not a fatal companion to civilization. Thus, in some US states, a slight decrease in the incidence of colorectal cancer has been observed among the white population over the past decade, while among the non-white population this figure has been steadily increasing.
This is due to a number of preventive measures taken:
- changing the nature of nutrition as a result of enhanced sanitary propaganda (reducing the consumption of animal fats, increasing the consumption of fresh fruits and vegetables, combating excess weight);
- early diagnosis of colorectal cancer.
Types of metachronous cancer
Symptoms of rectal cancer depend on the location of the tumor and its structure. Determining the nature of the tumor is necessary to determine treatment tactics, the rate and nature of tumor growth. Based on the nature of their growth, the following types of malignant neoplasms of the colon are distinguished:
- Exophytic colon cancer manifests itself in the growth of the tumor outward;
- Endophytic colon cancer is characterized by inward growth of the tumor;
- Mixed form (combines both types of tumor, in some cases it is an ulcer).
In oncology, the International Histological Classification of Cancer is used. Epithelial tumors are divided into several types:
- Tubular adenoma of the sigmoid colon;
- Tubular villous adenoma of the colon;
- Villous tumor of the rectum or other parts;
- Adenomatous polyp.
These neoplasms are benign, but colon cancer can develop against their background. In this regard, tubular adenoma of the colon requires regular monitoring. The following histological types of colon cancer are distinguished:
- Adenocarcinoma;
- Squamous cell carcinoma;
- Solid cancer;
- Melanoma;
- Scirrhous cancer;
- Signet ring cell carcinoma.
Depending on the degree of differentiation of the cells that make up the tumor, the following types of rectal cancer are distinguished:
- Highly differentiated formations, which contain more than 95% glandular structures;
- Moderately differentiated tumors - have from 50 to 90% glandular structures in the cells;
- Poorly differentiated tumors - glandular elements occupy from 5 to 50% of cells;
- Undifferentiated - contain less than 5% glandular cells.
Determining the type of colon cancer is necessary to select further treatment tactics, therefore, highly accurate diagnostics are carried out at the Oncology Clinic of the Yusupov Hospital.
Make an appointment
Treatment of intestinal cancer in the department of thoracoabdominal surgery and oncology
Treatment in the department is carried out according to the compulsory medical insurance, voluntary medical insurance, high medical insurance programs, as well as on a paid basis. Our department has highly qualified surgeons, modern equipment, comfortable hospital conditions and attentive staff. Read how to get treatment at the Department of Thoracoabdominal Surgery and Oncology of the Russian Scientific Center for Surgery.
To schedule a consultation, call:
+7 (499) 248 13 91 +7 (903) 728 24 52 +7 (499) 248 15 55
Submit a request for a consultation by filling out the form on our website and attaching the necessary documents.
Colon Cancer Symptoms
There are no signs of cancer of the rectum and other parts of the large intestine at the initial stage of development, so the disease is discovered accidentally during an intestinal examination or medical examination. Symptoms of colon cancer in women coincide with the general manifestations of the disease. In order to successfully treat colorectal cancer, symptoms in the early stages should not be ignored by the patient.
Comprehensive diagnostics using high-precision equipment allows specialists at the Yusupov Hospital to determine the causes of the problem and identify problems at an early stage. At the initial appointment, the oncologist carefully examines the symptoms of colorectal cancer in women, as well as hereditary predisposition.
In men, a rectal tumor, which may have no symptoms, develops in 60% of cases. Signs of rectal cancer and the first symptoms cause patients to turn to oncologists at a stage when the likelihood of a favorable prognosis is reduced. Experts note that colon cancer has signs and symptoms that are the same for women and men.
A tumor in the large intestine of a small size at the initial stage of formation does not cause pain or discomfort. As colon cancer increases in size, it manifests itself with the following symptoms:
- Pain in the abdominal area;
- Feeling of heaviness;
- Increased formation of gases in the abdomen;
- Irregular bowel movements.
If colon cancer develops, the first symptoms may not cause concern to the patient for a long time and may be mistaken for an upset stomach. At the Yusupov Hospital, colon cancer is diagnosed and symptoms are studied in the early stages to develop the most effective treatment program.
Symptoms of colorectal cancer in the early stages in women include decreased performance and intense headaches. In the later stages of the tumor process, damage to internal organs occurs, so general symptoms arise:
- Anemia – develops due to a lack of iron in the body as a result of regular bleeding. It manifests itself as pale skin, weakness, dizziness, brittle hair and nails. Leads to dysfunction of internal organs;
- Loss of body weight for no apparent reason. The development of a tumor always causes weight loss. Weight loss occurs due to dysfunction of the digestive system and metabolism.
Appetite worsens during chemotherapy or due to depletion of all the body's resources.
Ascending colon cancer
Cancer of the ascending colon is often characterized by the development of anemia in the early stages of the disease. This is associated with a neuroreflex effect on the part of the ileocecal segment of the intestine, which leads to impaired hematopoiesis. Malaise, fatigue, and body temperature rise. All these symptoms indicate the development of negative processes in the colon.
Metachronous colon cancer
Metachronous colon cancer most often develops after age 50. In first place is metachronous (multiple) sigmoid colon cancer, in second place is metachronous rectal cancer. Manifestations of primary multiple forms of cancer are diverse, symptoms are characteristic of a solitary tumor. There is weakness, severe pain, discharge with blood and mucus from the rectum, loss of appetite, rapid weight loss, constipation. Less commonly, the patient complains of bloating, tenesmus and loose stools.
Local manifestations of colon cancer
If sigmoid colon cancer develops, the first symptoms of the disease are similar to the pathological process in other parts of the intestine. Local manifestations of colon cancer are:
- Discomfort in the abdominal area resulting from microflora disturbances;
- Alternating constipation and diarrhea;
- Mucus and blood in stool. If sigmoid colon cancer develops, these symptoms differ in that inclusions envelop the stool. In case of cecal cancer, symptoms are characterized by mixing of blood and feces.
At the Yusupov Hospital, every person who applies receives help, regardless of the severity of the disease, so the first signs of rectal cancer do not go unattended.
Tests and diagnosis of colon cancer
Speaking about how to check the intestines for oncology, it should be noted that the optimal diagnostic method should be chosen by the doctor. As a rule, early diagnosis is carried out during a preventive examination or during studies related to other diseases.
To check the small intestine for the presence of a tumor, most often, if the development of intestinal cancer is suspected, a colonoscopy with biopsy . It is colonoscopy that makes it possible to conduct a detailed examination of the large intestine (rectum, colon, sigmoid, cecum).
To check the condition of the intestines without a colonoscopy, MRI is used. The most informative method, which makes it possible to obtain answers to a number of important questions, is PET-CT. In particular, this study makes it possible to determine what stage of the patient’s disease, whether he has metastases , whether surgery is advisable, etc.
To establish a diagnosis, a pathomorphological examination of the tissue is required. It makes it possible to distinguish between benign and malignant tumors. At the same time, it is important to conduct such a study qualitatively, since errors can be fatal for the patient.
An analysis is also carried out for the presence of occult blood. A special test is used for this.
An important stage of the examination is laboratory tests, in particular a blood test, during which tumor markers and other blood test indicators are determined. Speaking about which tumor marker indicates the presence of a malignant process in the body, it should be noted that only a specialist can correctly decipher the data obtained.
Other indicators (ESR, etc.) are not decisive during diagnosis, since the ESR level is not elevated in all such patients.
If necessary, other examinations are also practiced: rectosigmoidoscopy , irrigoscopy , etc. During the examination, laboratory tests, etc. are also carried out.
Stages
Oncologists distinguish several stages of rectal cancer according to the TNM classification.
T indicates the extent of the primary tumor in the colon:
- TX – insufficient data to assess the primary tumor site;
- T0 – the primary tumor in the intestine cannot be determined;
- Tis – the tumor grows within the mucous membrane;
- T1 – tumor grows into the submucosa;
- T2 – the tumor grows into the muscle layer of the intestinal wall;
- T3 – the tumor grows through all layers of the intestinal wall;
- T4 – the tumor grows into neighboring organs.
N characterizes the presence of cancer cells in regional (located next to the tumor) lymph nodes;
- NX – insufficient data to evaluate regional lymph nodes;
- N0 – lymph nodes are not affected;
- N1 – metastases were found in 1-3 regional lymph nodes;
- N2 – metastases were found in 4 or more regional lymph nodes.
M indicates the presence of distant metastases in various organs:
- M0 – no distant metastases;
- M1 – there are distant metastases.
When making a diagnosis, oncologists also use another classification, according to which colon cancer goes through 4 stages:
- The first stage is characterized by tumor growth into the wall of the organ, but it does not spread beyond its boundaries. At this stage, there are no metastases in regional lymph nodes, so the five-year survival rate exceeds 90%. Tubular adenoma of the colon with grade 1 dysplasia can develop in a patient asymptomatically;
- The second stage - the neoplasm extends beyond the intestine, metastases are not detected in the lymph nodes. Stage 2 rectal cancer has a survival rate of up to 75%;
- The third stage is characterized by tumor growth into the serosa and metastasis to the lymph nodes. Stage 3 rectal cancer has a favorable prognosis in 50% of cases;
- The fourth stage is terminal. The tumor affects nearby organs, and the formation of metastases is noted. If stage 4 rectal cancer is diagnosed, life expectancy is reduced: only 10% of patients survive the first five years.
Stage 4 sigmoid colon cancer brings patients pain and worsens psychological health. When treating patients with stage 4 rectal cancer, an experienced psychologist works with patients every day.
Symptoms of cancer by stage
Symptoms of the first stage of colon cancer appear in the form of periodic intestinal discomfort, constipation or stool disorders. At this stage, the primary tumor of the intestinal mucosa and submucosa grows. Streaks of blood and mucus may appear in the stool.
Signs of stage 2 colon cancer are also inexpressive: periodic constipation, stool upset, flatulence, abdominal pain, belching, heartburn, streaks of blood and mucus in the stool may appear.
Manifestations of the third stage of colon cancer include:
- Pain in the abdomen, stomach;
- Copious discharge of blood and mucus in the stool;
- Flatulence;
- Constipation that cannot be treated;
- Frequent nausea, occasional vomiting.
A tumor is often detected during palpation, depending on its location. The examination reveals regional lymph nodes affected by metastases.
Symptoms of the fourth stage of colon cancer are characterized by severe pain in the abdomen, blood in the stool, the appearance of purulent discharge caused by inflammation of the tumor itself, and the development of an abscess. The patient loses a lot of weight, loses appetite, develops iron deficiency anemia, and intestinal obstruction.
Make an appointment
Classification
The concept of “bowel cancer” combines a number of malignant diseases that affect different parts of the intestine. However, the colorectal form of the tumor is most common.
There are several different classifications of stages of this form. The simplest classification is considered to be:
- The first stage - the tumor spreads exclusively to the inner layers of the intestine. At this stage, about 90% of cases of the disease are cured.
- The second stage - the tumor actively increases and spreads through the intestinal wall to neighboring organs and structures.
- The third stage - the pathological process spreads to local lymph nodes (metastasis is observed).
- Stage four – the tumor spreads to the liver, lymph nodes, and lungs located remotely from the tumor.
Taking into account the clinical course of the disease, the following forms of oncological process of the colon are determined:
- Toxic-anemic – general symptoms ( anemia , fever ) dominate.
- Dyspeptic - discomfort in the gastrointestinal tract predominates, similar to the symptoms of gastritis or cholecystitis .
- Enterocolitic – intestinal disorders predominate.
- Obstructive – intestinal obstruction is noted, which progresses.
- Pseudo-inflammatory - manifestations of inflammation of the abdominal cavity are observed, in which pain, fever, and leukocytosis .
- Atypical - the presence of a tumor is determined by palpation, while adverse symptoms practically do not appear.
Metastases
Movement of the pathological focus is a common phenomenon in colon cancer. Stage 4 rectal cancer with metastases is difficult to treat; the efforts of oncologists are aimed at improving the patient’s quality of life and reducing the negative impact of the decomposition of damaged tissues.
Metastasis of malignant tumors in the large intestine occurs in the following organs:
- The liver receives blood that nourishes the internal organs. Stage 4 sigmoid colon cancer with liver metastases manifests itself in patients with accumulation of fluid in the abdominal cavity, nausea and vomiting, jaundice and general exhaustion of the body;
- The peritoneum is a thin film that lines the internal organs; after the tumor grows into the organs, foci of the pathological process appear in the peritoneum;
- When cancer metastasizes to the lungs, patients experience severe chest pain, coughing attacks, shortness of breath, and bleeding occurs when coughing.
Modern diagnostic equipment allows oncologists at the Yusupov Hospital to quickly identify metastases in colon cancer and provide adequate therapy. Stage 4 colon cancer with liver metastases has an unfavorable prognosis, however, experienced oncologists at the Yusupov Hospital provide palliative care to patients.
Diagnostics
Diagnosis of sigmoid colon cancer is performed at the Yusupov Hospital. Patients undergo a comprehensive examination. Early diagnosis improves the survival rate of patients with cancer. The diagnosis of rectal cancer is made based on data from numerous studies. The proctologist performs a digital examination of the rectum.
If the rectum and sigmoid colon are affected, sigmoidoscopy is performed. The main method for diagnosing colon cancer is colonoscopy. This is an endoscopic examination that allows the doctor to examine all parts of the colon and collect material for histological examination. Colonoscopy has the following advantages:
- Determining the exact location of the tumor;
- Clarification of the extent of the lesion;
- Detection of synchronous precancerous or cancerous lesions;
- Removal of polyps during the study.
At the Yusupov Hospital, to improve diagnostic accuracy, functional diagnostic doctors use the chromoendoscopic method - the mucous membrane is stained with special dyes. This makes it possible to identify pathological changes at an early stage and select areas for targeted biopsy. If for anatomical reasons it is not possible to examine the right parts of the large intestine and patients have multiple adenomas, irrigoscopy is used in addition to colonoscopy.
Radiologists at the Yusupov Hospital use the following methods for examining the intestines:
- Computed tomography. This method is highly accurate; it is based on obtaining many layer-by-layer images of a certain area of the body. Colorectal cancer, the symptoms and diagnosis of which are quite complex, can metastasize, so computed tomography is used to determine secondary lesions;
- Irrigoscopy with contrasting barium suspension. The method is based on the introduction of barium sulfate into the intestines, after which an x-ray examination is performed. This substance has the ability to absorb x-rays. A barium enema allows radiography to visualize the affected area of the colon;
- Magnetic resonance imaging - used to visualize the area under study. This method is the safest, since it is based on the use of electromagnetic radiation;
- Positron emission tomography – allows you to clarify the boundaries of tumor spread using labeled radioisotopes;
- Chest X-ray - used to detect metastases in distant organs.
X-ray diagnostic methods are used to determine the presence of a tumor in the large intestine and its location. In medicine, there are also methods for determining the origin of a neoplasm, its histological structure and the nature of disorders in the body.
The likelihood of developing colorectal cancer is high in those people whose relatives have this disorder. There is medical evidence that describes the presence in DNA of genes responsible for the development of colon cancer. Activation of these genes occurs when the body is exposed to negative factors, therefore, to identify the likelihood of cancer, it is necessary to undergo genetic testing. Oncologists at the Yusupov Hospital tell patients how to undergo screening for colorectal cancer. Genetic research is aimed at identifying genetic disorders that can trigger the pathological process.
If colon cancer is suspected, several laboratory tests are performed:
- A blood test is necessary to detect anemia, which develops as a result of bleeding from cancer. The presence of a pathological process is confirmed by violations of antigen receptors located on the surface of the cell membrane. A blood test allows you to accurately determine the degree of development of the lesion;
- Examination of feces. With colon cancer, blood enters the stool; in small quantities it may be invisible to the patient. Before the diagnosis, the patient requires special preparation, including avoiding eating fish, meat, and beets. Occult blood in stool can be present in various diseases, so other methods are used for accurate diagnosis;
- Biopsy - taking tissue samples from the tumor and lymph nodes.
To confirm the diagnosis of colon cancer and verify the tumor, a morphological study of the material obtained as a result of a biopsy is performed. At the Yusupov Hospital, the examination is performed by highly qualified histologists.
Description of the microslide in the presence of colon adenocarcinoma includes:
- Histological type of tumor;
- Degree of malignancy;
- The level of tumor growth into the intestinal wall and neighboring organs;
- The presence of atypical cells in the area located between the tumor and the resection margin;
- The presence or absence of vascular or perineural invasion;
- The number of removed lymph nodes and their damage to cancer cells.
Ultrasound examination allows you to visualize the tumor and describe in detail its size, location and determine whether it has invaded nearby organs. This method is highly informative, but screening allows you to determine whether colorectal cancer is developing.
Colon Cancer Screening
Screening studies conducted by oncologists at the Yusupov Hospital help improve patient survival. These tests allow you to identify the pathological process at an early stage, when there are no symptoms. Colon cancer screening is carried out using three main tests:
- Colonoscopy;
- Analysis of feces for occult blood;
- Visual examination of the mucous membrane using a sigmoidoscope.
Additional studies are:
- Injection into the intestinal lumen in cases of suspected tubular adenoma or colon adenocarcinoma of a contrast agent, followed by X-ray examination;
- Genetic analysis of feces;
- Virtual colonoscopy.
Diagnosis of rectal cancer and pathological processes in other parts of the large intestine at the Yusupov Hospital has a number of advantages:
- Use of European equipment, guaranteeing high accuracy of results;
- No queues and visiting specialists at a convenient time;
- Friendly and respectful attitude of the staff towards each patient;
- Fast processing of results and diagnosis in the shortest possible time.
Oncologists tell the patient what rectal cancer looks like and what the prognosis is for this disease. During the examination, the doctor informs patients how to distinguish hemorrhoids from rectal cancer, offers to undergo diagnostics and begin treatment for the disease.
Risk factors in the development of colorectal cancer.
1. Nutritional patterns of the population
Dietary factors that increase the risk of colon cancer include:
- excessive consumption of animal fats;
- eating food with insufficient plant fiber content;
- excess nutrition;
- drinking alcohol (especially beer).
- A diet high in red meat and animal fats and low in fiber is an important causative factor in the development of colorectal cancer.
A diet high in fruits, vegetables, and fiber-rich foods low in saturated fat is designed to protect the colon lining from the aggressive effects of bile acids and food carcinogens.
Reduce the risk of colorectal cancer:
- eating foods high in plant fiber;
- vitamins D and C;
- calcium.
Genetic factors
Most cases of colorectal cancer are sporadic, meaning they are not associated with any currently identified hereditary factors.
The role of a hereditarily determined mutation has been proven in two syndromes: total (familial) adenomatous polyposis (FAP) and hereditary nonpolyposis colon cancer (Lynch syndrome).
Familial adenomatous polyposis is a less common pathological process than hereditary colorectal cancer. The risk of developing colorectal cancer in patients with familial adenomatous polyposis is almost 100%.
Familial adenomatous polyposis is usually characterized by:
- hundreds of colorectal adenomatous polyps at a young age (20-30 years);
- adenomatous polyps of the duodenum;
- multiple extraintestinal manifestations (block 2-6);
- mutation in the tumor suppressor gene for adenomatous polyposis of the colon (APTC) on chromosome 5d;
- inheritance in an autosomal dominant manner (descendants of those affected have one of two chances of inheriting FAP).
The second (after familial adenomatous polyposis) syndrome with a significant contribution of hereditary predisposition is hereditary nonpolyposis colon cancer (HNPCC).
This syndrome is characterized by the following criteria:
- three cases of colon cancer (one of which occurred before the age of 50) in 2-3 different generations;
- two morphologically verified cancers of the colon in 2-3 different generations and one or more cases of cancer of the stomach, endometrium, small intestine, ovaries, urethra, renal pelvis (one of the cases of any cancer must be under the age of 50 years);
- young age of onset of colon cancer (up to 50 years) in both relatives in two different generations;
- the presence of synchronous, metachronous colon tumors in one relative and a case of colon cancer in a second relative (one of the cases of any cancer must be before the age of 50 years).
The molecular genetic cause of NNRTC is hereditary mutations in a number of genes, but 95% of these mutations are concentrated in 2 genes - MLH1 and MSH2. If a mutation in these genes is detected in a patient, it is recommended to search for this mutation in his relatives.
Dynamic monitoring of those relatives who are carriers of mutations is also recommended to identify the possible occurrence of colon cancer at an early stage, which will undoubtedly lead to more effective treatment.
Other risk factors
- single and multiple adenomas (polyps) of the colon;
- nonspecific ulcerative colitis;
- Crohn's disease;
- history of female genital or breast cancer;
- immunodeficiencies.
Identifying polyps is extremely important in preventing cancer, since colon cancer most often develops from polyps rather than de novo. The risk of a colon polyp degenerating into cancer is high: for a polyp less than 1 cm in size - 1.1%, 1-2 cm - 7.7%, more than 2 cm - 42%, on average - 8.7%.
Although most polyps remain benign, some, if not removed, can degenerate or transform into malignant (cancerous) tumors. The process of transformation of polyps is most likely caused by genetic mutations in the cells.
There are different types of polyps, but only one type is thought to develop into cancer. This type of polyp is called adenomatous polyp. Until you have a special examination (colonoscopy), you cannot be sure that there are no polyps in your intestines, because polyps do not cause any symptoms. Large polyps or tumors may cause symptoms such as bleeding, blood in the stool, anemia, or bowel obstruction. These symptoms are quite rare and only begin to appear when the polyps become very large or cancerous.
Modern principles of colorectal cancer screening
Timely detection of colorectal cancer involves diagnosing it in the early, preclinical stages, when there are no clinical manifestations of this disease. Screening, or early detection of colorectal cancer, is carried out using digital examination, hemoccult test and endoscopic method. Digital examination of the rectum can detect up to 70% of rectal carcinomas.
The basis for performing a hemoccult test is that colorectal adenomas and carcinomas bleed to varying degrees.
When screening among a formally healthy population, from 2 to 6% of those examined have a positive hemoccult test. Upon further examination of patients who have a positive hemoccult test, colorectal cancer is detected in 5–10% of cases, and glandular adenomas in 20–40% of cases.
In 50–70% of cases the test is false positive.
Sigmoidoscopy and total colonoscopy are important components of colorectal cancer screening. Using modern flexible sigmoidoscopes 60 cm long, it is possible to detect 55% of adenomas and carcinomas of the sigmoid and rectum that develop de novo. The sensitivity of this method is 85%. (The American Medical Association currently recommends sigmoidoscopy every 3 to 5 years, starting at age 50, in individuals who do not have any complaints of bowel dysfunction).
Symptoms of cancer of the rectosigmoid junction
In the early stages of development (no growth into the muscular layer of the intestine, no regional and distant metastases), rectal and colon cancer is almost 100% curable.
Rectal cancer can be manifested by the discharge of blood, mucus from the anus, and disruption of the usual stool pattern. You may experience bloating and abdominal pain. The development of cancer can lead to weight loss, anemia, pain in the anus, and painful urge to defecate.
Most people are uncomfortable discussing the functioning of their bowels, however, unless you tell your doctor about unusual symptoms, such as changes in the shape of your stool, he will never know about it and most likely will not even ask!
Here's a quick rundown of what to look for (most of these symptoms affect many people and are not cancer-related, but let your doctor decide):
- change in the mode and nature of bowel movement - one-time or chronic diarrhea or constipation, discomfort during bowel movement, change in the shape of the stool (pencil-thin or thinner than usual), a feeling of incomplete bowel movement;
- unusual sensations associated with the intestines, such as increased gas formation, pain, nausea, bloating, a feeling of fullness in the intestines;
- bleeding (light red or very dark blood in the stool);
- constant fatigue;
- unexplained weight loss;
- unexplained iron deficiency;
- unexplained anemia.
However, in the early stages, cancer can develop asymptomatically. The only way to detect cancer or a precancerous disease (adenomatous polyp) in such cases is preventive colonoscopy.
Even very developed healthcare systems are unable to perform a colonoscopy on all residents of the country without exception; in addition, the instrumental examination is invasive in nature, which means there is a minimal risk of complications. Therefore, in Belarus, as in most socially oriented countries, so-called stool occult blood screening tests are carried out. If a positive reaction is detected, such a patient is advised to undergo a colonoscopy.
Diagnosis of cancer of the rectosigmoid junction
The main method of making a diagnosis is morphological: the so-called biopsy, when a fragment of tumor tissue is removed for microscopic examination.
It is possible to reach a tumor in the intestinal lumen using endoscopic examinations:
- sigmoidoscopy (insertion of a rigid tube into the anus to a depth of 28 cm);
- colonoscopy (elastic optics for the entire length of the intestine).
Medical imaging techniques are used to determine the extent of the tumor:
- Ultrasound (including through the lumen of the rectum - transrectal ultrasound);
- computed tomography;
- magnetic resonance imaging.
Treatment of cancer of the rectosigmoid junction
The main method of treatment for cancer of the rectosigmoid junction is surgical - resection of the rectosigmoid junction.
When resection of the rectosigmoid junction of the colon, the distal and proximal edges of the colon should be at a sufficient distance from the tumor: at least 5 cm on an unfixed specimen. All regional lymph nodes from the mouths of the lower mesenteric vessels are removed in a single block with the tumor.
Resection of the rectosigmoid junction according to Hartmann (with the formation of an end colostomy) is performed in case of complications of the tumor process (intestinal obstruction, tumor perforation) and the patient’s condition is decompensated for concomitant diseases.
In cases of tumor spread to adjacent organs and tissues, combined operations are performed with removal of the drug in a single block, and in the presence of distant synchronous metastases (in the liver, lungs, ovaries, etc.) - their simultaneous or stage-by-stage removal (as determined by a council of doctors ).
The feasibility of other treatment methods (radiation and chemotherapy) is determined after staging the disease, based on the receipt of the final morphological report of the pathologist (approximately 7-10 days after surgery).
Dispensary observation
Surgical removal of the tumor is the most effective treatment for colorectal cancer. Even after all the cancer is removed, cancer cells may remain in other organs and parts of the body. These clusters of cancer cells may be so small at the time of the first surgery that they cannot be detected. However, after some time they may begin to grow.
The possibility of developing a recurrence of colorectal cancer (return of the disease) depends on the stage and characteristics of the course of the disease. The occurrence of tumor recurrence may complicate subsequent treatment with chemotherapy and/or radiation therapy.
With early diagnosis of recurrent colon and rectal cancer, patients have a greater chance of successful treatment, including surgery.
Periodic monitoring of patients can detect the formation of new polyps in the colon in patients who have previously had colon cancer (after surgery, new polyps form in approximately every fifth patient who has previously been diagnosed and treated for colon cancer).
Since polyps can degenerate and become malignant over time, it is very important to detect and remove them without waiting.
Most relapses of cancer are detected within the first two years after surgery, so the intensity of monitoring is maximum during this period of time and the purpose of the examination is primarily to exclude the development of recurrence of the disease.
The likelihood of cancer recurrence after the first five years after surgery is sharply reduced. The main task of observation during this period is to detect new polyps of the colon and rectum.
During the follow-up examination, your health status is assessed and an examination is prescribed: once every six months for the first two years after surgery and once a year for the next 3-5 years and includes:
- physical examination;
- blood test for the tumor marker CEA or CEA (an abbreviation for carcinoembryonic antigen or cancer embryonic antigen) is a special protein that is found in the blood. With an active tumor process, the level of this protein in the blood of patients with colon and rectal cancer can sometimes increase);
- colonoscopy (examination of the lumen of the colon and rectum);
- chest x-ray;
- CT scan;
- examination of the abdominal and pelvic organs using ultrasound.
Treatment
Treatment of colorectal cancer with conservative methods is impossible, so surgery is performed to remove the tumor. If a neoplasm is diagnosed, treatment tactics are determined by the degree of damage to the large intestine. Oncologists at the Yusupov Hospital additionally use radiation therapy or chemotherapy to treat colorectal cancer.
The questions of many patients who turn to oncologists are related to whether colorectal cancer can be cured. Early diagnosis and timely therapy improve the prognosis for this disease; at the initial stages of the development of the pathological process, the probability of a favorable outcome is high.
Operations
The main treatment method for rectal cancer is surgery. A malignant tumor is spreading rapidly, so conservative methods cannot stop the pathological process. Preoperative examination includes:
- Examination by an oncologist;
- General and biochemical blood test with assessment of liver and kidney function;
- Determination of the level of tumor marker CEA;
- Performing a colonoscopy;
- Computed tomography of the pelvis, thoracic and abdominal organs.
Several types of operations have been developed depending on the stage of cancer and its location. Surgeons at the Oncology Clinic masterfully perform the following surgical interventions on the colon in the presence of a malignant tumor:
- Laparoscopic resection - this operation is in demand, as it allows you to stop the pathological process with minimal intervention;
- Abdominal-anal resection - characterized by the removal of the affected section of the intestine, after which the surgeon sews both ends and removes the section of the intestine located in the anus;
- Intra-abdominal resection - with this method, the affected area of the intestine is removed; during the intervention, a colostomy can be placed on the anterior wall of the abdomen;
- Obstructive resection, or operation using the Hartmann method, is performed when there is a high probability of prolonged healing of the wound surface. With this method, the surgeon removes the tumor, then removes the colostomy and sutures the other end of the intestine. Subsequently, surgical intervention to suturing the colostomy is possible.
Adenocarcinoma of the sigmoid colon, which is treated surgically, can be successfully treated at the initial stage of development. Oncologists at the Yusupov Hospital provide high-quality medical services and provide psychological support to each patient.
Doctors at the Yusupov Hospital perform the following operations for colon cancer:
- Resection of the ileocecal angle, in which part of the small intestine and the cecum are removed, a primary anastomosis is performed (connection of the small and large intestine);
- Right hemicolectomy, during which the terminal small intestine and ascending colon with the hepatic flexure are removed;
- Resection of the transverse colon with adjacent lymph nodes;
- Left-sided hemicolectomy, when the splenic flexure of the colon and the descending part of the colon are removed;
- Anterior resection of the rectum with removal of the sigmoid colon and the upper ampullary part of the rectum;
- Low anterior resection of the rectum - removal of the upper and middle ampullary sections of the rectum with resection of the sigmoid colon.
Most often, in a planned situation, oncologists form primary anastomoses. Surgeons sew together the two ends of the resected intestinal fragments. During an emergency operation, the intervention consists of additional placement of an ileostomy or colostomy on the anterior abdominal wall.
When a patient undergoes preoperative neoadjuvant chemotherapy or radiation treatment with signs of partial intestinal obstruction, surgeons place intestinal stents using colonoscopy to preserve excretory function. After neoadjuvant treatment, at a meeting of the expert council, the possibility of radical surgery is considered.
In the case of the initial presence of distant metastases, the primary tumor is removed during surgery. Then adjuvant treatment is carried out (chemotherapy, radiation therapy, or a combination of these methods). This approach helps prevent the breakdown of tumor tissue or the development of intestinal obstruction.
Make an appointment
Radiation therapy before surgery
Radiation therapy is one of the components of treatment for rectal cancer. Ionizing radiation promotes the destruction of tumor cells, and healthy cells are also susceptible to its influence. Radiation exposure before tumor removal surgery helps eliminate symptoms. If sigmoid colon cancer is diagnosed, treatment using this method after surgery improves the prognosis.
Colostomy
Treatment of rectal cancer in some cases requires the creation of a colostomy, which is an opening through which gases and feces are removed from the colon. An artificial anus is removed if the following indications are present:
- Damage to a large part of the intestine;
- Inflammatory process after radiation therapy;
- Suppuration and fistulas in the large intestine;
- Impossibility of surgical removal of the tumor;
- High probability of complications when removing a fragment of the colon;
- Germination of formation into organs.
Patients with a colostomy use special containers to collect stool.
Palliative chemotherapy
Chemotherapy treatment is carried out with drugs that have a detrimental effect on atypical cells and reduce the likelihood of metastases. Chemotherapy for rectal cancer is carried out before surgery or after surgery. Chemotherapy is used as the main treatment for tumors that cannot be removed by surgery.
This treatment method has side effects such as nausea, hair loss, diarrhea, inflammation of the mucous membranes and neutropenia. Before the procedure, oncologists warn patients about the possible consequences. Constant laboratory monitoring of the level of formed elements allows doctors at the Yusupov Hospital to timely adjust doses and medications.
Diet
Nutrition for colorectal cancer should be balanced. The cooks at the Yusupov Hospital include foods high in plant fiber in the patient’s diet. This measure is aimed at preventing constipation and removing toxins. The therapeutic diet for rectal cancer is an addition to the main therapy.
General dietary recommendations for colon cancer:
- Small meals 5-6 times a day;
- Use of fresh products when preparing food;
- Eating boiled or steamed food;
- Refusal of fatty meats, smoked and pickled foods;
- Exclusion from the diet of carbonated drinks and foods that increase gas formation.
The diet for radiation therapy of the rectum requires the exclusion of coarse, salty foods, which irritate the oral mucosa. Nutrition for colon cancer for patients at the Yusupov Hospital is developed by a nutritionist taking into account individual preferences. The diet includes fresh foods
Causes and risk factors
family history influences the occurrence of colon cancer —approximately 25% of people with colorectal cancer have it. In the presence of hereditary nonpolyposis colorectal cancer (HNPCC), progression to colorectal cancer occurs in 80% of cases.
Hereditary syndromes are taken into account :
- familial adenomatous polyposis: 100% of people develop colorectal cancer by the age of 40,
- Gardner syndrome,
- Turco syndrome,
- Peutz-Jeghers syndrome,
- juvenile polyposis syndrome.
The likelihood of developing colon cancer is greater in old age, and also in people over 40 years of age.
A number of diseases are also risk factors :
- Colorectal adenomas and serrated polyps.
- Inflammatory bowel diseases: chronic inflammation → hyperplasia → non-polypoid dysplasia → neoplasia.
- Nonspecific ulcerative colitis and Crohn's disease.
- Endocarditis and bacteremia caused by S. gallolyticus.
- Diabetes mellitus type 2.
- Obesity.
- History of abdominal irradiation in childhood.
Lifestyle and diet are of great importance . Promote the appearance of intestinal tumors:
- smoking,
- alcohol consumption,
- high fat, low fiber diet,
- eating processed meat.
Protective factors that reduce the risk of developing colorectal cancer
- Long-term use of aspirin and other NSAIDs.
- Physical activity.
- A diet high in fiber and vegetables and low in meat.
Prognosis and survival
The prognosis for colon cancer depends on the depth of tumor invasion and the involvement of regional lymph nodes in the pathological process. Important prognostic factors are:
- The degree of differentiation of tumor tissue;
- Perineural or vascular invasion;
- Involvement of resection edges in the pathological process.
Unfavorable signs include perforation of the tumor, intestinal obstruction, increased levels of tumor markers CA 19.9 and CEA.
The five-year survival rate after surgical removal of the tumor is 85-95% for the first stage, 60-80% for the second stage, and 30-60% for the third stage. In the presence of single metastases to the liver, surgeons perform partial resection of the organ. After surgery, the five-year survival rate is 40%. After removal of metastases in the lungs, the five-year survival rate ranges from 35 to 45%. When a well-differentiated colon adenocarcinoma is detected, the prognosis is better than with a poorly differentiated tumor.
The prognosis for moderately differentiated colon adenocarcinoma depends entirely on the stage of the cancer. With timely early diagnosis, oncologists at the Yusupov Hospital are able to carry out radical treatment that prevents relapses and metastasis. If the tumor is detected in the last stages, the prognosis worsens.
Treatment of colon cancer in Moscow
Treatment of colon cancer in Moscow is carried out by oncologists at the Yusupov Hospital, who are experts in this field. Experienced specialists at the Oncology Clinic provide patients and their relatives with high quality services. After visiting a specialist and diagnosis, treatment for colorectal cancer in Moscow is prescribed in the shortest possible time.
If a patient is diagnosed with colon cancer, oncologists at Yusupov Hospital develop an individual treatment program. You can make an appointment with an oncologist and find out the cost of services by calling the Yusupov Hospital phone number. Contact center specialists answer all questions from patients and their relatives around the clock.
Statistics
According to statistics, the disease is the third most frequently diagnosed cancer in the world, and there is a constant increase in cases of its detection. It accounts for about 8% of all new cancer cases in the United States. In 2012, approximately 447,000 patients in Europe were diagnosed with this disease. This is approximately 13% of all cancer cases in the region.
Colorectal cancer is more common in men than in women . In Europe, one in 20 men and one in 35 women will develop colorectal cancer at some stage in their lives. In other words, every year in Europe, approximately 35 men out of 100,000 men and approximately 25 women out of 100,000 women are diagnosed with colorectal cancer. The peak incidence is observed between 65 and 74 years . The incidence of colorectal cancer is higher in industrialized and urbanized areas.
Epidemiology of colorectal cancer (morbidity and mortality)
Prevention
Preventing colon cancer is one of the main activities of oncologists at the Yusupov Hospital. The preparation of an individual prevention program is carried out after a comprehensive diagnosis and analysis of the data obtained. Oncologists with many years of experience in treating colorectal cancer offer patients the following areas of prevention:
- Making changes to your diet. One of the provoking factors in the development of this disease is the consumption of red meat, which is cooked at high temperatures, resulting in the formation of carcinogenic substances. Experts recommend minimizing the consumption of these products. In addition, to prevent colon cancer, doctors advise consuming foods rich in fiber, calcium and vitamins A, C, D;
- Quitting drinking alcohol and smoking;
- Timely treatment of inflammatory bowel diseases and prevention of constipation;
- Removal of colon polyps.
Specialists at the Yusupov Hospital draw the attention of patients to the need to undergo annual examinations in case of hereditary predisposition and the presence of provoking factors. In order to undergo an examination using modern equipment if you suspect colon cancer, call the Yusupov Hospital. If doctors rule out the presence of a malignant neoplasm, colon cancer prevention will be carried out.
If a tumor is present, its type and stage will be determined, an individual patient management plan will be drawn up, and adequate treatment will be provided. In the oncology clinic, the patient will be selected for optimal therapy, using the most modern and effective medications with minimal side effects, and will also be provided with dietary nutrition for colon cancer.
Make an appointment
Causes of bowel cancer
The main reasons for the development of tumors in the intestines are as follows:
- Heredity - the tumor is more often diagnosed in people whose close relatives had this type of cancer, or they were diagnosed with intestinal polyps.
- Excessive consumption of red meat - those who eat pork, lamb, and beef too often are at risk.
- Poor diet in general - the likelihood of illness is increased in those who consume few vegetables, fruits, grains and at the same time eat a lot of animal fats.
- Insufficient physical activity.
- Smoking, alcohol abuse.
- Inflammatory bowel disease - the likelihood of the disease increases with Crohn's disease and chronic ulcerative colitis .
- Unfavorable environmental conditions.