Doctors Cost
Price list Doctors clinic
Cholecystitis is an inflammation of the gallbladder. The inflammatory process disrupts the function of the entire gastrointestinal tract, since bile, which is involved in the digestion process, accumulates in the gallbladder and is subsequently released into the intestine. Therefore, the disease, as a rule, does not go unnoticed, but some of its forms have nonspecific symptoms that can easily be confused with irritable bowel syndrome and signs of other gastrointestinal diseases.
Causes of cholecystitis
The inflammatory process occurs due to the proliferation of pathogenic bacteria. They can enter the gallbladder from the intestines or other organs through the lymph or blood flow. The source of the disease can be pyelonephritis, proctitis, inflammation of the pelvic organs, ENT organs, etc. However, this usually occurs in the presence of “favorable” conditions - stagnation of bile. Stagnation occurs due to one or more reasons:
- cholelithiasis (formation of stones that block the ducts of the gallbladder and impede the outflow of contents);
- congenital deformities of the gallbladder;
- biliary dyskinesia;
- muscle tone disorders;
- parasitosis;
- unbalanced diet – long periods of fasting, overeating, frequent intake of fatty foods, simple carbohydrates;
- sedentary lifestyle;
- previous abdominal injuries, surgeries;
- psycho-emotional stress.
Doctors are more often faced with the treatment of calculous cholecystitis. In this case, stones can form due to impaired motility of the gallbladder and vice versa - the appearance of stones impedes the outflow of bile, which leads to inflammation of the walls of the organ.
In some cases, the cause of the inflammatory process is endocrine and allergic diseases, a general decrease in immune forces, and the use of medications that change the composition and viscosity of bile.
Acute acalculous cholecystitis
Features of diagnostics. Diagnosis of acute cholecystitis is complex and combines data from physical and mental examinations. The purpose of diagnostic measures is not only to establish the fact of cholecystolithiasis and signs of inflammation of the gallbladder wall, which largely determines the urgency of surgery and the duration of preoperative preparation, but also the possibility of a full-scale preoperative examination and selection of an adequate treatment method. The patient's severe general condition, high body temperature, severe chills, tachycardia, severe pain in the right hypochondrium, the presence of neutrophilic leukocytosis with a significant band shift, toxic granularity of neutrophils, increased ESR make it possible to suspect acute cholecystitis. In patients over 60 years of age, the diagnosis of acute cholecystitis is often difficult due to its atypical course. General and local reactions can be mild, purulent and destructive forms are often observed, and diffuse peritonitis develops.
To solve these problems, ultrasound examination of the organs of the hepatopancreatobiliary zone, biochemical blood testing, hepatobiliscintigraphy, laparoscopy, and endoscopic retrograde cholangiopancreatography are performed.
Ultrasound signs of acute cholecystitis are thickening of the bladder walls more than 4 mm, a “double contour” of the wall, an increase in the size of the gallbladder, an impacted stone at the mouth of the cystic duct, the presence of perivesical fluid, a positive ultrasound Murphy sign (local tension of the gallbladder under an ultrasound probe) . Ultrasound data can indicate inflammation of the gallbladder.
It should be noted that in some cases, ultrasound is not as informative in diagnosing choledocholithiasis. Therefore, it is necessary to correctly set the task of the study: it consists not so much in detecting stones in the extrahepatic bile ducts, but in searching for direct and indirect signs of biliary hypertension. Expansion of intrahepatic bile flows, an increase in the diameter of the common hepatic and bile ducts are important signs of impaired bile outflow. However, additional research is needed to clarify the cause of cholestasis.
The role of ultrasound in predicting the nature of the proposed operation is extremely important. Reliable signs of the technical complexity of the planned cholecystectomy are:
- lack of free lumen in the gallbladder;
- thickened or thinned bladder wall;
- large immovable stones in the neck or Hart-Man pocket;
- perivesical fluid collection
Dynamic ultrasound is also used in diagnosis - repeated ultrasound examination against the background of a changing or stable clinical picture of the disease (thickening of the walls, an increase in the volume of the gallbladder, the appearance of paravesically located fluid in the abdominal cavity - signs of irogression of the inflammatory process). Dynamic ultrasound makes it possible to assess the course of the inflammatory process and promptly carry out surgical intervention.
The most significant biochemical indicators:
- hyperbilirubinemia mainly due to direct (conjugated) bilirubin;
- an increase in the level of liver fraction of alkaline phosphatase (ALP) in the blood;
- lack of stercobilin in feces;
- increased content of bile pigments in the urine;
- increased activity of alanine aminotransferase (ALAT) and aspartate aminotransferase (AST), γ-glutamyl transpetidase (GGTP)
Hepatobilis scintigraphy (HBSG) is an important radioisotope method for assessing the condition of the gallbladder and bile ducts. It is one of the radioisotope research methods that record the movement of a radiopharmaceutical through liver cells and bile ducts. Normal indicators of the rate of release of a radiopharmaceutical from liver cells and its movement and evacuation from the bile ducts reliably indicate the absence of a violation of the bile flow into the intestine. If the rate of movement of the radiopharmaceutical through the extrahepatic bile ducts slows down and its release into the duodenal lumen is delayed, the presence of stones or strictures in the ducts should be suspected. To resolve these doubts, X-ray contrast studies (ERCP or intraoperative cholegraphy) are required. The GBSG method also makes it possible to assess the functional state of the gallbladder and liver cells, which is especially important for identifying obstructive forms of acute cholecystitis, reactive and chronic hepatitis. Low invasiveness, high technology and information content of GBSG are the basis for its widespread use in patients with suspected mechanical the nature of jaundice in case of insufficient physical, laboratory and ultrasound examination. Normal indicators of the functional state of the bile ducts according to GBSG make it possible to select patients for isolated cholecystectomy and not resort to X-ray contrast studies both before and during surgery. The gallbladder that was not contrasted during the study in 95% of patients indicates the obstructive nature of its lesion and the futility of continuing conservative treatment.
Laparoscopy is indicated for patients with an unclear clinical diagnosis. In acute cholecystitis, laparoscopy has a high resolution and also provides significant assistance in the differential diagnosis of inflammatory diseases of the abdominal organs and tumor lesions.
ERCP is the most informative method for diagnosing changes in the bile ducts, including choledocholithiasis, stenosis of the major duodenal papilla and extended common bile duct strictures. ERCP is only possible in patients with acute cholecystitis without symptoms of widespread peritonitis.
The absolute indication for ERCP is obstructive jaundice at the time of the study.
Differential diagnosis for acute cholecystitis should be made with acute appendicitis, acute pancreatitis, urolithiasis and pyelonephritis, liver abscess, perforated gastric and duodenal ulcer, right-sided pneumonia and pleurisy.
Signs of cholecystitis
Symptoms of cholecystitis depend on the form of the disease, the presence or absence of stones. In inflammation complicated by cholelithiasis (cholelithiasis), the manifestation of hepatic colic often occurs. Its symptoms include the following:
- sharp pain on the right. The attack occurs suddenly, the pain increases over a short period of time, lasting from several minutes to several days. As the pain subsides, it becomes aching and persists for a long time;
- bitter taste in the mouth;
- nausea, vomiting, after which there is no relief;
- yellowing of the sclera and skin;
- bloating;
- bowel dysfunction (constipation);
- elevated body temperature: up to 37.5–38 ˚С in simple forms and up to 39 ˚С in purulent forms of acute cholecystitis.
Chronic cholecystitis does not manifest itself so clearly, and there may be no stones in the gallbladder. A prolonged inflammatory process can manifest itself with the following symptoms:
- heaviness in the right hypochondrium, weak aching pain;
- pain radiating to the right collarbone, shoulder blade, arm, to the left side of the abdomen after eating fatty, smoked foods, marinades, alcohol, soda, undergoing intense exercise, stress;
- appetite disorders;
- bitter belching;
- nausea;
- bloating, heaviness in the abdomen;
- alternating diarrhea and constipation.
When diagnosing and treating acalculous cholecystitis, it is important to tell the doctor about all symptoms, including those that occur at rest, outside of exacerbations.
Symptoms of cholecystitis
Acute cholecystitis:
- Characterized by paroxysmal pain in the left hypochondrium, which can radiate to the right shoulder, scapula
- Nausea, vomiting
- Increase in body temperature to 38-38.5 C with chills
- The appearance of yellowness of the sclera, skin, itching
Chronic cholecystitis:
- Nausea.
- Dull aching pain in the right hypochondrium
- Bitterness in the mouth
- Possible prolonged low-grade fever
- Bloating
- Diarrhea
Diagnostics:
- General clinical analysis of blood and urine
- General analysis of stool for coprogram.
- Biochemical blood test (liver tests, cholesterol, alkaline phosphatase, amylase, glucose)
- Ultrasound of the hepatobiliary system
- ECG
- Cholecystocholangiography
- ERCP (endoscopic retrograde cholangiopancreatography)
Methods for diagnosing cholecystitis
At the first appointment with a therapist or gastroenterologist, it is necessary to describe the symptoms, as well as answer the doctor’s questions about your medical history, previous diseases and operations, lifestyle, and diet. If cholecystitis is suspected, the specialist will refer you to the following diagnostic procedures:
- clinical and biochemical blood test;
- duodenal intubation: carried out to differentiate cholecystitis from other gastrointestinal diseases, as well as to take a bile sample for further culture, thus it is possible to determine the type of pathogenic flora that provokes inflammation and assess its sensitivity to antibiotics;
- Ultrasound of the gallbladder: the study makes it possible to determine the condition and structure of the organ, size, wall thickness, identify deformations and congenital defects, bile stagnation, stones, tumors;
- X-ray diagnostics: an image of the abdominal cavity is necessary if perforation of the gallbladder, large stones, calcifications, obstruction of the bile ducts is suspected;
- radioisotope study: makes it possible to assess the patency of the bile ducts, detect acute forms of inflammation, etc.
Comprehensive diagnostics allows you to obtain accurate information and make the right decision.
Treatment of calculous cholecystitis
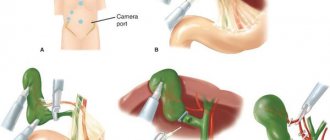
Treatment of calculous cholecystitis and cholelithiasis (cholelithiasis) is radical; if large stones are present, the organ is removed. The operation can be performed urgently or planned. In the first case, the urgency is explained by an acute attack, blockage of the ducts, and a high risk of organ rupture. In the second case, it is possible to perform laparoscopic access - small incisions. The intervention is controlled using a modern optical system, which makes it possible to guarantee the accuracy of surgical manipulations. Laparoscopy allows you to shorten the recovery period and minimize complications.
Acute calculous cholecystitis
The cause of the acute form of calculous cholecystitis is stones that obstruct (clog) the neck of the gallbladder. In this case, the outflow of bile stops, and an infection develops in the bladder itself. The disease manifests itself as sharp pain in the right hypochondrium, nausea, repeated vomiting, and weakness.
An attack of acute calculous cholecystitis has some differences from “ordinary” hepatic colic. First of all, this is an increase in temperature, signs of inflammation in a blood test - neutrophilic leukocytosis, increased erythrocyte sedimentation rate, changes on ultrasound.
If it is not possible to achieve the effect of conservative therapy in the first day or two, the patient has to be operated on. Emergency surgery is more complex and has a greater risk of complications.
Treatment of acalculous cholecystitis
In the absence of complications (calculi), the disease is subject to conservative therapy. Treatment of chronic acalculous cholecystitis includes the use of medications to relieve inflammation, relieve unpleasant symptoms, and restore normal organ function. The basis of treatment is the following:
- drugs to improve the properties of bile;
- medications that normalize bladder tone;
- medications that relieve the inflammatory process.
The doctor selects antibiotics based on the results of bile tests. It is important to influence the cause, namely the bacterial flora that provoked the inflammation.
In 20% of cases, there is no improvement after conservative treatment. Then we are talking about planned surgical intervention.
Therapeutic measures for acute cholecystitis
Exacerbation of cholecystitis requires urgent measures. If surgery is not required, the specialist may recommend the following treatment regimen:
- following a strict diet, avoiding fatty, smoked, spicy foods, alcohol, heavy foods, etc.;
- drug therapy: antibacterial drugs, anti-inflammatory drugs, antispasmodics, medications to normalize the process of secretion and excretion of bile;
- restorative therapy;
- symptomatic treatment: medications to normalize stool, painkillers, etc.