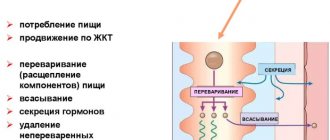
The smallest and most “famous” section of the large intestine. Almost every patient knows where his “appendicitis” is located, pointing to the lower part of the right abdomen. Appendicitis is not the name of an organ, but the name of acute inflammation of the appendix. This is the disease that is most often encountered in emergency surgery.
When it comes to the anatomical location of the appendix, they say that “usually” it is located in the right abdomen, below, in the iliac region. What then is “unusual”? Very rarely, but there is a mirror arrangement of internal organs, “visus vescerum inversus”. In this case, everything will be like in a mirror - the organ located on the right will be on the left, and vice versa. There is also an anomaly in the development of the large intestine, when the dome of the cecum is located under the liver. These are the so-called rotation anomalies. During intrauterine development, the large intestine grows and moves peripherally in the abdominal wall, as if counterclockwise. With an anomaly, the cecum simply does not reach its given point and remains in the right hypochondrium. Fortunately, for surgeons, this is very rare in the clinic. Even more rarely, but cases of the presence of two and even (!) three appendixes have been described. But it happens... It happens that the appendix does not come from the cecum, but from other parts of the large intestine, or the appendix may not be there from birth.
Let's talk about the “usual” thing. The anatomy of the appendix cannot be discussed in isolation from the cecum, since evolutionarily the appendix is part of the cecum. The vermiform appendix began to attract doctors over the last 130-140 years. Before this, a purulent process in the right iliac region was not associated with anything, but the “worm” was not perceived as a source of infection. Then for a long time it was believed that this was an “extra” organ, a useless atavism that caused nothing but problems. For some time there was even a boom in preventive appendectomy (the not yet inflamed appendix was removed as a “prevention”). This mainly affected European countries.
Anatomy of the ileocecal region
In general, the concept of “ileocecal region” includes the ileocecal valve, the final section of the small intestine and the cecum with the appendix. The small intestine is connected to the large intestine through the ileocecal valve (valva ileicaecalis). There are many symptoms in the literature: it is named after the authors who studied it. Tulpa valve (N.Tulp), fallopian valve (G.Falloppio), or Bauhinian valve (C.Bauhin). These are all the same anatomical formation.
The shape of the valve resembles the mouth opening and has an upper and lower lip. Both the small and large intestines are involved in its formation. The upper and lower lips, connecting, form angles from which high folds extend - the frenulum of the ileocecal valve. Actually, these frenulums anatomically divide the cecum from the ascending colon. The most common cause of rumbling in the stomach is the ileocecal valve “speaking” (“ileocecal valve song”). Anatomically, the Bauhinian valve performs an important function: it separates the contents of the small and large intestines. When the function of the valve is impaired, the contents of the large intestine, richly contaminated with bacteria, flow back into the small intestine, which is not normal. This leads to bacterial overgrowth in the small intestine.
How to find the ileocecal valve?
This is Künz's point - 2 cm below and to the right of the navel
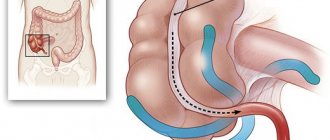
A series of folds are formed in the ileocecal region: cecal folds, superior and inferior Guillot folds. The important thing is that these folds form pockets covered with peritoneum, into which loops of the small intestine can enter (albeit rarely). This leads to symptoms of internal hernias that are difficult to diagnose.
Places of possible paracecal hernias are circled with ovals.
Now about the “worm” The appendix is a hollow organ extending from the dome of the cecum and usually looks like a thick pencil. At the base of the process, three muscle bands (“crow’s foot”) converge - taenia. This is a good guide for surgeons: we go down to the area where the muscle bands converge. Like many abdominal organs, the appendix is covered on the outside by peritoneum and has a mesentery, which contains blood vessels and nerves that supply it.
Usually the length of the vermiform appendix is 7-10 cm, its thickness is 5-8 mm. The literature describes rare cases when the appendix has a much larger size: 20-30 cm. In 1968, M. Rudnetsky and N. Rabinovich described a vermiform appendix 40 cm and 8 cm thick. The smallest length of the appendix - 0.5 cm was described in 1903 year Huntington. A freely located appendix in the abdominal cavity is usually located straight, with a slight bend in the middle - Reid's bend. The shape is most often stem-shaped (of the same thickness). But it can also be conical (like it is in newborns - tapering towards the end) or cone-shaped (on the contrary, tapering at the base). By the way, this is why appendicitis is extremely rare in newborns, because their appendix looks like a funnel, tapering towards the top.
The vermiform appendix opens into the intestinal lumen as the orifice or opening of the appendix. Here the mucous membrane forms a kind of fold that covers the opening - the Gerlach valve, or Gerlach valve (not always detected). This valve from the fold of the mucosa prevents intestinal contents from entering the appendix cavity. Therefore, it is reasonable to explain to children the dangers of eating fruits (mainly cherries) with seeds, as well as seed husks. The risk is very small, but a seed or sunflower husk can get into the lumen of the appendix and block its lumen.
The position of the appendix in the abdomen itself depends on the position of the cecum. This is usually the right iliac fossa. In men, the lowest part of the dome of the cecum is at the level of the anterior-superior iliac spine. This is the same protruding pelvic bone on the left and right. We draw a horizontal line: we get the place where the dome of the cecum is projected. The vertical coordinate is the middle of the inguinal ligament. In women, the height of the dome of the cecum is usually slightly lower than in men, but during pregnancy (starting from 4-5 months) it moves higher and in the 3rd trimester the dome can rise to the right hypochondrium.
One of the most important components of the digestive tract is the ileocecal region, which includes the cecum with the appendix, the terminal ileum and the ileocecal valve (ICV; bauhinian valve). This section is often affected by inflammatory processes and serves as the site of the most frequent occurrence of adhesions [1].
One of the leading places in the structure of urgent abdominal pathology is occupied by complications of colorectal cancer [2]. The most common complications of colon cancer are intestinal obstruction [3, 4] and gastrointestinal bleeding, which are localized in the ileocecal region in 8.3–14.5% of cases [5].
At the Department of Operative Surgery and Clinical Anatomy named after. S.S. Mikhailov Orenburg State Medical University conducted studies that obtained data on the macro- and microanatomical structure of the ileocecal junction, variant x-ray anatomy of the entire ileocecal region, and its changes in tumor lesions of the cecum [6]. These studies formed their own basis for studying the intravital endoscopic anatomy of the ileocecal intestine.
The relevance of studying the ileocecal region is due not only to the high frequency of its pathological conditions, but also to the development of microsurgical operations on the organs of the digestive system [7, 8]. Sphincter-preserving and sphincter-modeling operations are being actively developed [8, 9].
An analysis of the literature on endoscopic anatomy revealed the insufficiency and fragmentation of the available data on the endoscopic anatomy of the ileocecal region and its changes in ulcerative colitis and Crohn's disease.
The purpose of the study is to obtain a set of new data on the endoscopic anatomy of the ileocecal region in mature and elderly people to improve diagnosis and surgical treatment.
This study was carried out on 182 patients who were examined and treated in the clinic and hospital of the Orenburg Regional Clinical Hospital. The age of all those examined ranged from 18 to 75 years. All those examined were divided into two age groups: mature age (men from 18 to 60 years old, women from 18 to 55 years old), elderly (men from 61 to 75 years old, women from 56 to 75 years old).
Among the 182 people examined, there were 84 men and 98 women. In addition, two groups were identified: 1st - 97 apparently healthy patients, i.e., without diseases of the colon and terminal ileum, 2nd - 85 patients with ulcerative colitis and Crohn's disease. Based on the results of the examination of patients in these groups, the endoscopic anatomy of the ileocecal region was described and analyzed, and for patients with an intact ileocecal junction (group 1) - taking into account age and gender differences.
In this study, the following set of methods was used to solve the problems: endoscopic (video colonoscopy, video ileoscopy, examination of the mucous membrane in white light and in NBI mode, methods of taking material for histological examination); morphometry; morphological examination of biopsy specimens - histological examination technique; X-ray (irrigoscopy, irrigography); variational-statistical data processing.
Individual differences in endoscopic anatomy of the ileocecal region.
When studying the endoscopic anatomy of the ileocecal region in patients without pathology in this area, three directions of the ICC were established (into the dome of the cecum, perpendicular to the axis of the cecum and into the ascending colon) with a predominant direction of the ICC into the dome of the cecum (71.1% of cases). ICC forms are identified depending on the level of inspection. When examined from the ascending colon, flattened, flat and crescent-shaped forms are determined, combined into non-protruding forms, and saddle-shaped and polypoid - into protruding forms. In patients without ICC pathology, non-protruding forms of ICC predominate (67%). During a frontal examination of the ICC, the labiform form predominates among the labiform, transitional and papillary forms (81.4%). The range of length of the upper lip of the ICC was determined to be from 1.6 to 3.9 cm, with a predominance (81.5%) of the average length - from 2.4 to 3.0 cm (Fig. 1).
Rice.
1. Ileocecal valve. Colonoscopy. Endophoto. The thickness of the upper lip of the ICC is more often (56.7%), but without significant differences, from 0.2 to 0.5 cm, in 43.3% - from 0.6 to 0.8 cm, its height - from 0.2 up to 1.6 cm with some advantage (45.4%) of low height 0.4-0.9 cm compared to average (40.2%) 1.0-1.6 cm ( p
>0.05). Of the three options (small, medium and large) lengths, the lower lip of the ICC, like the upper lip of the ICC, had predominantly an average length (80.4%), i.e., from 2.1 to 2.8 cm. Its thickness, as and the thickness of the upper lip of the ICC, slightly more often (52.6%) was in the range of short length, i.e., from 0.2 to 0.4 cm compared with the average length (0.5–0.7 cm) in 47 .7% of cases. The anterior and posterior frenulum had a length of 0.2 to 0.5 cm in 86.6 and 87.6% of cases, respectively.
Among patients with cylindrical, cone-shaped and spherical forms of the cecum, there were mainly individuals with a cylindrical shape (77.3%). The distance from the ICC to the mouth of the appendicular process in 84.5% of cases ranged from 1.8 to 5.9 cm, to the far point of the dome of the cecum in 80.5% - from 4.0 to 8.3 cm. Equally often (in 48.5 and 45.4% of cases, respectively) there are patients with two and one circular folds. 4 (4.1%) had no folds, only 2 (2%) had 3 folds. Their height was uniform throughout the fold from 0.2 to 0.8 cm in 65% of cases and up to 1.5 cm in 35%. Almost all patients had a projection of the free (99%) and omental (92.8%) bands, and their width ranged from 0.4 to 0.8 cm in 77.1% of cases and from 0 in 94.4% of cases. .2 to 0.8 cm, respectively. No projection of the mesenteric band was found.
The proposed method for determining the wall where the final portion of the ileum enters the colon during colonoscopy is confirmed by irrigography data. There was agreement between the data obtained from colonoscopy and radiography regarding the entry of the terminal portion of the ileum into the posterior wall. As for the medial and posteromedial variants of the confluence, in 3 cases, during an X-ray examination, the wall of the confluence was determined to be medial, and during an endoscopic examination in these patients, it was determined to be posteromedial. In this case, the angle according to endoscopy corresponded to the range from 63 to 67.5°, i.e., it was comparable to the angle corresponding to the medial wall. This difference (4.5°) can be attributed to method errors, which cannot have clinical significance.
With colonoscopy, more often than with fluoroscopy and radiography, the maximum height of the cecum is determined, which may be associated with the introduction of air into the intestine to examine it, and irrigoscopy and irrigography provide more reliable information in this case, so it is necessary to focus on radiological data. (determining the height of the cecum is important for operational access during laparoscopy and endoscopic intraluminal operations).
The deviation of the axis of the cecum from the axis of the spinal column can be minimal (from 0 to 25°) and maximum (from 26 to 51°), which occurs approximately equally. The angle of deviation of the cecum axis in relation to the spinal column must be taken into account during laparoscopy to prevent complications.
For the relationship between the axis of the ascending colon and the cecum, the most characteristic is the condition in which the axis of the cecum serves as a continuation of the axis of the ascending colon, therefore a moderate angle between them, and especially a significant one (26-51° in 27.3% of cases) should be taken into account when colonoscopy and laparoscopy.
As the study of endoscopic anatomy in patients with an intact ileocecal region shows, in terms of gender and age, minor differences were identified in some parameters. Thus, in men, no directions of the mouth of the ICC towards the ascending colon were identified (in women - 5.4%, or 3 people). When assessing the forms of ICC from the ascending colon, non-protruding forms were identified somewhat more often in women, and during a frontal examination, lip-shaped forms were more common in old age. Morphometry of the upper lip of the ICC showed that its average length, as well as greater thickness, are slightly more common in women.
As for the distance to the mouth of the appendix and to the far point of the dome of the cecum, in both cases the average distances were 1.3 times more common in women. In terms of the number of circular folds in the cecum, a slight difference can be seen in the frequency of detection of three circular folds in the age aspect - in adulthood they were identified in 2 cases, and in the elderly - in none. A small width of the free band in the cecum was somewhat more often detected in men and adults.
The identified differences in the endoscopic anatomy of the ileocecal region can only be considered as possible trends, since no statistically significant differences were found.
Endoscopic anatomy of the ileocecal region in patients with ulcerative colitis and Crohn's disease.
In patients with ulcerative colitis and Crohn's disease, among the three directions of the ICC, in 54.1% of cases the direction was found to be in the dome of the cecum and in 35.3% - perpendicular to the axis of the cecum. When examining the ICC from the ascending colon, its flattened forms were predominantly found (81.1%), while frontal examination revealed a labiform form (84.7%). The range of length of the upper lip of the ICC is from 1.5 to 3.1 cm, with a predominance of the average length - from 2.4 to 3.1 cm (78.3%). There were no patients with a large length (from 3.2 to 3.9 cm).
The thickness of the upper lip of the ICC ranged from 0.2 to 1.2 cm, without significant differences between the small (43.4%) and large (56.6%) thickness. Its height was mostly (90.4%) within the range of low (43.4%) and medium (47.0%) values. The lower lip of the ICC in 78.3% of cases had an average length (from 2.1 to 2.8 cm) and in 60.2% - a large (0.5-0.8 cm) thickness, with significant differences with a short length - 39.8%. The length of the anterior and posterior frenulum, with a length range from 0.2 to 1.0 cm, in 71.1 and 78.3% of cases, respectively, has a short length (0.2-0.5 cm). Among patients with cylindrical, cone-shaped and spherical forms of the cecum, patients with a cylindrical shape were most often (67.7%) and patients with a spherical shape were least likely (9.4%). The range of distance from the ICC to the appendix was from 1.9 to 5.9 cm in 90.6% of cases to the far point of the dome of the cecum (from 4.0 to 8.2 cm) in 84.7% of cases. In patients with ulcerative colitis and Crohn's disease, most often (57.6%) there was 1 fold in the cecum, in 1/3 - 2 folds, folds were absent in 6 (7.1%) people. The height of these folds ranged from 0.2 to 0.8 cm in 88.2% of cases, from 0.9 to 1.0 cm in 4.7%. In 89.4% of patients, the projection of the free band and omental band was determined - 83.5%. Their width was predominantly small - from 0.2 to 0.8 cm in 89.5 and 100% of cases, respectively.
Patients with ulcerative colitis and Crohn's disease had varying degrees of severity of inflammatory changes (swelling, hyperemia, erosion, ulcers, granularity, deformation) of the mucous membrane of the cecum, ICC, and ileum. In 2 patients, it was impossible to carry out morphometry of the ICC elements due to severe deformation of the ileocecal region and severe inflammatory process (Fig. 2-4).
Rice. 3. Ascending colon. Colonoscopy. Endophoto.
Rice. 4. The area of the lower lip of the ileocecal valve facing the opening. Colonoscopy. Endophoto.
Rice. 2. Changes in the ileocecal region in ulcerative colitis and Crohn's disease. Colonoscopy. Endophoto.
Patterns of endoscopic anatomy of the ileocecal intestine and their clinical significance.
The first pattern.
ICC is characterized by individual differences in direction with a predominance in the dome of the cecum and forms depending on the level of examination: from the ascending colon (predominantly flattened form) and during frontal examination (predominantly labiform) without significant gender and age differences being studied.
Second pattern.
The length, thickness of the upper and lower lips, the height of the upper lip of the ICC, the length of the anterior and posterior frenulum are individually variable with a predominance of length from 2.4 to 3.1 cm and 2.1–2.8 cm, thickness from 0.2 to 0. 8 cm respectively for the upper and lower lips, the height of the upper lip is from 0.4 to 2.2 cm.
The third pattern.
For the endoscopic picture of healthy patients, among cylindrical, cone-shaped and spherical shapes, the most characteristic is the cylindrical shape of the cecum, as well as the distance from the mouth of the ICC to the appendix from 1.8 to 6.0 cm, to the far point of the dome of the cecum - from 4.0 to 8.3 cm, with no significant differences between men and women and age periods.
Fourth pattern.
It is possible to form 3 folds in the cecum, but two (48.5%) and one (45.4%) folds with a height of 0.2 to 0.8 cm are approximately equally common, as well as from three ribbons - free and omental tapes with a width of 0.2 to 0.8 cm, regardless of gender and age periods studied.
Fifth pattern.
The endoscopic anatomy of the ileocecal region undergoes changes in ulcerative colitis and Crohn's disease, the leading signs of which are an increase in the number of cases of ICC direction into the ascending colon and perpendicular to the axis of the cecum and its non-protruding forms, a decrease in the length and an increase in the thickness of the upper and lower lips, the length of the frenulum, an increase the number of patients with a cone-shaped cecum and without folds or with one fold of the mucous membrane with a predominance of low height, as well as a decrease in the width of the bands and the rare detection of a free band, the appearance of inflammatory changes in the mucous membrane, erosions, ulcerations or its cicatricial deformation.
Thus, the endoscopic anatomy of the ileocecal region consists of individually variable factors determined during intravital endoscopy: the shape, external structure and direction of the ICC, the internal relief and shape of the cecum, the projection and width of the bands, intraluminal morphometric parameters of the elements of the ICC and the cecum.
During endoscopy of the ICC from the ascending colon in the phase of its relaxation, non-protruding (flat, flattened, crescent-shaped) and protruding (saddle-shaped and polypoid) forms were identified. The predominant forms are flattened (40.2%) and saddle-shaped (19.6%). Upon frontal examination of the ICC, labiform (predominant - 81.4%), papillary and transitional forms were identified.
The anatomical parameters of the elements of the ICC are in the range of individual differences: for the upper lip, the length is from 1.6 to 3.9 cm, thickness - from 0.2 to 0.8 cm, height - from 0.4 to 2.3 cm, for the lower lip length is from 1.4 to 3.5 cm, thickness is from 0.2 to 0.7 cm, for the anterior and posterior frenulum the length is from 0.2 to 1.0 cm.
Under normal conditions, among the different forms of the cecum: cylindrical, cone-shaped, spherical, the cylindrical shape is predominant (77.3%). The distance from the ICC to the mouth of the appendix varies from 1.8 to 6.0 cm, and to the far point of the dome of the cecum - from 4.0 to 8.3 cm.
Gender endoscopic differences in the ileocecal region are insignificant and are expressed in a slight decrease in the length of the upper and lower lips of the ICC in men and a decrease in the number of folds of the mucous membrane of the cecum in women. Age differences between the mature and elderly groups include a higher frequency of ICC direction towards the ascending colon, a decrease in the length of the lower lip, fewer and flattening folds of the mucous membrane of the cecum, and a decrease in the width of the free and omental bands.
In ulcerative colitis and Crohn's disease, there is an increase in the number of patients with the direction of the ICC towards the ascending colon, crescent-shaped ICC, a decrease in the length and an increase in the thickness of the upper and lower lips of the ICC, a decrease in the height of the upper lip and an increase in the length of the valve frenulum. The diseases are accompanied by edema, hyperemia, erosive and ulcerative changes in the mucous membrane and, if complicated, stenosis, severe deformation of the ileocecal region.
On the part of the cecum in ulcerative colitis and Crohn's disease, an increase in variants with a cone-shaped form of the cecum, a decrease in its length, a decrease in the number and flattening of the folds of the mucous membrane was noted. Radiologically it is possible to assess the level of location of the cecum, the relationship of the axis of the cecum with the ascending colon and the axis of the spine, the direction of the ileum before entering the cecum, and the presence of ileocecus.
Information about authors
Shepelev A.N. — Candidate of Medical Sciences, endoscopist, Orenburg Regional Clinical Hospital; e-mail; https://orcid.org/0000-0002-7946-5422
Dronova O.B. - Doctor of Medical Sciences, Prof. Department of Surgery, Institute of Professional Education, Federal State Budgetary Educational Institution of Higher Education "Orenburg State Medical University" of the Ministry of Health of the Russian Federation; e-mail
Kagan I.I. — Honored Scientist of the Russian Federation, Doctor of Medical Sciences, Prof. Department of Operative Surgery and Clinical Anatomy named after. S.S. Mikhailov Federal State Budgetary Educational Institution of Higher Education "Orenburg State Medical University" of the Ministry of Health of the Russian Federation; e-mail: k_topanatom @orgma.ru
Fateev I.N. - Doctor of Medical Sciences, Prof. Department of Operative Surgery and Clinical Anatomy named after. S.S. Mikhailov Federal State Budgetary Educational Institution of Higher Education "Orenburg State Medical University" of the Ministry of Health of the Russian Federation; e-mail
Corresponding author:
Fateev Ivan Nikolaevich — e-mail
Shepelev A.N., Dronova O.B., Kagan I.I., Fateev I.N. Endoscopic anatomy of the ileocecal region and its changes in some inflammatory bowel diseases. Operative surgery and clinical anatomy (Pirogov scientific journal).
2019;3(3):31-37. https://doi.org/10.17116/operhirurg2019303131
Sherren's appendicular triangle, or how to find the projection of the appendix onto the abdominal wall
The projection of the vermiform appendix onto the anterior abdominal wall is localized within the area called Sherren's triangle. We connect the navel, pubic tubercle and the anterior superior spine of the right ilium:
Due to the presence of the mesentery, the appendix itself feels quite free relative to the cecum and can occupy various anatomical locations (in the case of a common mesentery with the cecum - caecum mobile, the displacement of these organs increases even more). As Maingot said: “The vermiform appendix is the only organ in humans that does not have a permanent position, considered the norm.” These different anatomical variants lead to the fact that with appendicitis the clinical picture becomes similar to the clinical picture of inflammation of neighboring organs. It is not for nothing that surgeons call appendicitis the simplest and at the same time the most difficult disease to diagnose. Therefore, do not be at all surprised and always be understanding if the surgeon at the clinic sends you to the hospital. In a hospital setting, laparoscopy may often be required to clarify the diagnosis.
Functions
The main function of the bauhinium valve is to regulate the movement of the bolus of food from the small intestine to the large intestine and to delimit the overlying parts of the organ from the colon populated by bacteria.
The activity of the ileocecal valve has several stages, which depend on the intake of food into the body:
- outside the digestive process, the Bauhinian valve is closed;
- approximately 5 minutes after eating, the valve begins to open and allow small portions of food to pass through - 10-15 ml of chyme;
- the activity of the valve is regulated by peristalsis - a wave of muscle contraction, passing through the ileum, changes the pressure in the cavity of the organ, which leads to the opening of the valve;
- the entry of food into the large intestine leads to an increase in pressure in the cavity of the cecum and closure of the valve;
- throughout the entire digestion period, the valve opens and closes cyclically every minute;
- after all the chyme has passed into the large intestine, the valve closes and remains in this position until the next meal.
On average, the Bauginian valve allows up to 4 liters of chyme to pass from the small intestine into the large intestine per day.
Variants of the position of the appendix relative to the cecum
Information from my favorite library PubMed. Sandro Cilindro de Souza, Journal of Coloproctology, Rio de Janeyro, 2015. Scientists examined the anatomical location of the appendix in 377 cadavers. Here's what happened:
What does this mean? And the fact that in almost half of the cases the appendix “hides” behind the dome of the cecum.
Blood supply to the ileocecal region
The organs of the ileocecal region are supplied with blood from the ileocecal artery, a.ileocolica (departs from the main line - the superior mesenteric artery)
Blood supply to the terminal portion of the small intestine This is always a difficult issue for surgeons, since there is a lack of vascularization here. The last 40 cm of the small intestine is called the “avascular zone of Treves”. In order to preserve anastomoses, when there is a need to ligate the a.ileicolica, the surgeon must retreat from the ileocecal angle by 3-5 cm. The final section of the small intestine can be resected only by retreating from the ileocecal angle by at least 10 cm.
Blood supply of the cecum It is fed by the anterior and posterior cecal artery (a.caecalis anterior and a.caecalis posterior). It is important that a branch can extend from the posterior cecal artery to the base of the appendix, where it connects with the appendicular artery (a.appendicularis).
Blood supply to the appendix
The ileocecal artery (a.ileocolica) gives off a branch - the appendicular artery, which reaches the appendix in the thickness of its mesentery. The tip of the appendix is worst supplied. Why do surgeons often observe a blackened tip of the appendix? Swelling during inflammation partially compresses the blood circulation, which leads to necrosis of the distal part. This is especially common in older people. For them, 5-6 hours are enough for the development of gangrenous appendicitis, again, due to circulatory problems. Another important point for surgeons: the appendix is supplied with blood by the appendicular artery only in half of the cases (according to HAKelly, 1905). In a quarter of cases - by several vessels, and in another quarter - it is fed together with the posterior part of the cecum by branches of the posterior ileo-cecal artery. If the mesentery is ligated at the base of the appendix in this case, this entails necrosis of the cecum. Therefore, it is not recommended to ligate the arteries of the appendix too far from it.
Venous outflow from the appendix is carried out through the veins of the same name. Surgeons need to remember that venous outflow is associated with the venous system of the retroperitoneal space and inflammation can spread to the retroperitoneal tissue. The entire venous system of the intestine is collected in the portal vein, which carries blood to our main “filter” - the liver. A terrible complication of appendicitis (almost always fatal) is pylephlebitis (portal vein thrombosis).
If you find a typo in the text, please let me know. Select a piece of text and press Ctrl+Enter.
Tags: anatomy, appendix, cecum, sphincter, colon
- Related Posts
- Munchausen's disease: what doctors need to remember
- About rare
- Medicine Symbols
« Previous entry
Diseases of the bauhinium valve
Ileocecal valve insufficiency
Bauginian valve insufficiency is a condition that occurs when the valve is unable to delimit the cavities of different parts of the intestine. With this pathology, reflux develops - the reverse reflux of contents from the large intestine into the cavity of the ileum, as well as into higher parts of the digestive system (up to the stomach).
The internal environment of the large intestine is very specific; it differs from other organs in the presence of bacteria. When opportunistic bacteria penetrate the small intestine and stomach, inflammatory processes develop - enteritis or gastroenteritis. Such diseases usually have a chronic course, since new microorganisms from the colon constantly arrive at the site of pathology.
Valve lipomatosis
Lipomatosis is the deposition of fatty droplets in the valve wall. Excessive accumulation defects lead to the valve becoming much denser and limiting the intestinal lumen. Against the background of this condition, the normal passage of food masses through the intestines is disrupted, and signs of partial intestinal obstruction appear.
Be sure to read:
What is anoscopy and how is it performed?
Endometriosis of the ileocecal valve
In rare cases, endometriotic damage to the valve is possible. The disease is characterized by the proliferation of cells similar in structure to the endometrium in the thickness of the valve. The reasons for the return of tissue from the uterus have not yet been fully established. The disease can only affect the ileocecal valve, but more often endometriosis also spreads to the cecum.
Bauginite
Bauginitis is a disease that is characterized by the occurrence of an inflammatory process in the cavity of the ileocecal valve. The disease can also have an isolated course or be combined with inflammation of the small and large intestines.
The occurrence of bauginitis is associated with the entry of pathogenic bacteria into the digestive system, which penetrate the wall of the organ and begin to multiply there, provoking the development of the inflammatory process. In some cases, pathology can be caused by opportunistic bacteria - microorganisms that live in the intestines and normally do not cause harm to the body. They can cause illness if a person has significantly weakened local intestinal immunity.