Types of atresia of the anus and rectum
Depending on the length of the rectum, which ends blindly (with a gas bubble), atresias are divided into: low (sublevator, anal) - its closed end does not reach the skin by less than 2 cm; average (intermediate); high (supralevator, anorectal) - the blind end is deeper than two centimeters from the surface.
There are fistula and non-fistula (complete) forms of the pathology. 90% of cases belong to the first of them. Fistula deviations are characterized by the presence of passages that open into: the groin area; reproductive system; urinary organs.
Variants of fistula-free atresia: abnormality of the anus and rectum; defectiveness of the anal canal, its absence or covering with a translucent layer of skin (meconium pigmentation); underdevelopment of the intestinal canal with the correct structure of the anus. It is necessary to distinguish atresia from stenosis.
Diagnostics
Photo: dvizhenie.com
Many people and parents wonder: how does a doctor diagnose various forms of atresia?
Making a diagnosis of obstruction of the anus and esophagus is not difficult. Even in the maternity hospital, newborns are immediately carefully examined. If the first stool, meconium, is not excreted, then the doctor immediately diagnoses it as atresia. When examining the anus, the skin may be too thin, which indicates the form of the disease. In the presence of biliary atresia, the doctor pays attention to the symptoms: the presence of a yellow tint to the skin. A pregnant woman may have polyhydramnios during an ultrasound scan. If the stomach of the fetus is not visible on ultrasound, doctors make a diagnosis of atresia in advance.
Diagnosis of esophageal atresia can be carried out using:
- Purposes of abdominal fluoroscopy. View the chest. Fluoroscopy is divided into non-contrast and contrast. In the first option: the inserted catheter is visible in the blind segment of the esophagus. If there is a fistula, then the stomach and intestines are filled with air. With contrast fluoroscopy, the blind end of the esophagus is clearly visible;
- Using a catheter. It is administered through the nasal cavity. If the catheter rests against the wall of the esophagus without further advancement or enters the trachea, this means the presence of pathology;
- "Elephant's test" Air is introduced through a probe into the blind end of the esophagus, which exits through the nose. Probing of the esophagus is quick, but the method is not 100% accurate.
After the birth of a newborn, gases accumulate in the intestines within a couple of hours. During fluoroscopy, the child is turned upside down. The resulting gas bubble allows you to examine the position of the intestine and establish an accurate diagnosis. This is necessary to know for a quality operation. If complete atresia is not detected in time, the newborn does not survive even a week.
Esophageal atresia can be diagnosed if the patient already has established diseases:
- Atresia of the anus;
- Heart disease;
- Prematurity;
- Pathologies of the upper extremities;
- Spine pathologies;
- Polyhydramnios in a pregnant woman.
When diagnosing intestinal obstruction, the doctor pays attention to the following symptoms:
- Mathieu-Sklyarova. It is carried out by palpation. When the abdominal wall is shaken, a splash of fluid that has accumulated in the intestine is heard.
- Shimana-Danza. It is carried out by palpation. The right iliac fossa appears empty.
- Chugaeva. If you pull the child's legs towards the stomach, a noticeable transverse stripe appears on the stomach.
- Hose. When palpating the abdomen, increased bloating and gas formation are noticeable.
- Krivulya. When palpating the abdomen, a metallic sound is heard.
- Obukhovskaya. The rectum and anus are dilated.
- Golda. Determined by palpation. The loops of the small intestine are distended.
- Tsege-Manteuffel. When introducing water into the rectum, more than half a liter cannot be introduced.
If intestinal obstruction is suspected, the doctor checks the hernial orifice for the moment of pinching. An x-ray of the abdominal cavity is taken. If dynamic intestinal obstruction is detected, then it is imperative to immediately identify the cause; it may be the presence of: appendicitis, pancreatitis, blood clots and other pathologies.
Atresia of the colon and small intestine is detected through an abdominal x-ray. If the presence of a number of distended loops of the small or large intestine is detected, the diagnosis is confirmed. The x-ray shows volumetric formations due to the accumulation of gases.
The doctor may prescribe additional examination:
- Echocardiography of the heart;
- Screening using amniocentesis;
- X-ray of the kidneys;
- Sweat chloride concentration test.
Symptoms of atresia of the anus and rectum
The clinical picture depends on the pathology. With a fistula-free nature, 10-12 hours after birth, the newborn begins to show anxiety, does not suckle the breast, does not pass meconium, symptoms of obstruction (ileus) appear, namely bloating and asymmetry of the abdomen, vomiting of gastric contents, then bile and feces, toxicosis and dehydration of the body. The baby may push, and when the gas bubble is low, the skin in this area bulges. Ileus also develops in the fistulous form, since narrow fistulous lumens have poor patency for feces. In this case, it can be released through the urethra, genital opening or openings in the perineum. As a result, concomitant diseases arise - cystitis, pyelonephritis, vulvitis, urosepsis, which can cause death. Therefore, when the first warning signs appear, you should immediately make an appointment with a pediatrician.
Symptoms
Photo: grud.guru
Symptoms of atresia of the esophagus, large and small intestine depend on the degree and type of intestinal damage. The more advanced the disease, the more pronounced the symptoms.
Intestinal obstruction is a severe pathology. Some symptoms can help identify the disease and begin timely treatment. The main signs of atresia in newborns:
- Spasmodic pain;
- Bloating;
- Absence of defecation;
- Foamy discharge from the mouth;
- Heavy salivation;
- Vomiting when feeding;
- Cough;
- Moodiness, restlessness;
- Difficulty breathing;
- Refusal of milk.
The pain with atresia is sharp, growing in the navel area. With partial obstruction or fistulas, diarrhea may occur. Bloating is characterized by asymmetry of the abdomen, the child is restless and constantly tightens his legs. When feeding, choking, coughing and vomiting begins. The vomit contains an admixture of bile; in advanced cases, fecal discharge appears. With obstructive and adhesive forms, vomiting becomes continuous. Such symptoms are often complicated by pneumonia.
With obstruction of the large intestine, the symptoms are less pronounced than with pathologies of the small intestine. If the obstruction of the small intestine is partial, doctors can prescribe conservative treatment methods; in case of complete obstruction, surgical intervention is mandatory.
Symptoms of atresia can be classified according to the location of the pathology:
- Anus. The posterior opening is closed completely or partially. There is a depression no larger than 5 mm in size, the child cannot defecate. The rectum may become fused with the bladder. In this case, the urine becomes dark and unusual in color.
- Microtia. Partial or complete closure of the ear canal. The child becomes deaf or has no hearing at all.
- Biliary atresia. A newborn develops jaundice. The bile ducts are either completely absent or partially obstructed. The skin tone becomes greenish-yellow, bilirubin increases, and the thrombus index decreases. The urine becomes darker and the liver enlarges.
- Esophagus. White foam and a copious flow of saliva are released from the child's mouth and nose. Cardiac and gastrointestinal defects often occur with esophageal atresia.
- Small intestine. The newborn is missing a significant part of the intestine. The parts of the intestine are connected by a cord. The child vomits during feeding. Bile and feces may be released from the mouth.
- Follicular atresia. Sometimes it develops unnoticed and leads to infertility.
- Pulmonary artery. At birth, the child acquires a bluish tint that does not disappear. Frequent shortness of breath, suffocation when feeding.
- Vagina. Vaginal fusion. Frequent spasmodic pain in the lower abdomen, menstrual irregularities. Inability to be sexually active.
- Choanal atresia. The back area of the nose is narrowed, the passage is covered with fabric. Breathing problems appear. The child needs immediate assistance at birth. Because newborns cannot breathe through their mouths.
- Tricuspid valve. The blood circulation process in the heart is disrupted. Cyanosis, loss of consciousness, and shortness of breath develop. This leads to blockage of blood vessels.
With atresia with fistulas, the child defecates in small quantities. If the fistula is wide, then feces come out as usual, and pathology may not be immediately suspected. Partial obstruction develops with variable pain and bloating.
Diagnosis of atresia of the anus and rectum
To make an accurate diagnosis, consultation with a pediatrician, gynecologist, proctologist, urologist and surgeon may be required. The absence of the anus is detected during the initial examination by a neonatologist; other defects are recognized within the first 24 hours. In this case, the examination is carried out in a short time, including: invertography according to Kakovich-Wangensteen-Rice - when the anus is formed, a radiopaque marker is placed in it, the child is placed upside down in front of the X-ray machine. The distance from the mark to the gas bubble determines the height of the atresia; digital examination; rectoscopy; proctography; fine-needle puncture according to Sitkoevsky - the skin in the groin is pierced towards the intestine, a needle is inserted with a gradual pull of the piston. When meconium appears in the syringe, the analysis is considered complete; Ultrasound, MRI, electromyography; diagnostic laparoscopy.
The placement of fistula canals is clarified using urethrocystography, catheterization of the urethra, and fistulography. To establish concomitant abnormalities, ultrasound of the heart, kidneys and other organs, and esophagoscopy are prescribed.
Description
A congenital anomaly accompanied by the absence or overgrowth of a natural opening or canal in the human body is called atresia. Atresia is rarely a consequence of any other pathology. The most commonly recognized types are:
- rectal atresia
- anal atresia
- hymen atresia
- esophageal atresia
- atresia 12 duodenal
- hymenal atresia
- Choanal atresia
- venous atresia
- atresia of the external auditory canal
- lacrimal atresia
- atresia of the internal os
- atresia of the cervical canal, etc.
Congenital atresia
Doctors deal with congenital pathologies from the very birth of a child. They are found during examination of a newborn. The features of such anomalies are easier to group from a simple visible form to a complex, sometimes even unique one. In children, such pathologies most often are not observed in the first hours of their life, unless they are too obvious. But the most common atresia in a newborn - anal atresia - makes itself felt within a few hours. There is a lack of meconium waste, and sometimes even with a superficial examination it is possible to determine the absence of the anus. Since the concept of high and low atresia has not yet been accurately classified when defining them in the intestinal region relative to their location in relation to the levator muscles (above or below), it is believed that the high one is deeper than 2.5 centimeters, therefore, the low one is before that meanings. Newborns experience discomfort, the tummy swells, and vomiting begins: first with the contents of the stomach, and a little later - with an admixture of bile. The child no longer wants to feed, toxicosis progresses, and vomiting becomes more frequent. If the child is not treated surgically, this type of disease very quickly progresses to the acute stage - intestinal perforation and peritonitis. Such atresia has dire consequences, including death.
There are no completely established causes of intrauterine anomalies in children. The causes of atresia are most often congenital.
Esophageal atresia
Such an anomaly is a serious defect. With it, part of the upper segment of the esophagus ends indistinctly, and part of the lower segment may fall into the trachea. This deviation in children is often combined with defects of other organs:
- heart;
- gastrointestinal tract;
- genitourinary system.
Most often, such defects occur when there is a chromosomal disease. Esophageal atresia in children is associated with defects at the early stage of embryogenesis. At an early stage, the trachea is connected to the esophagus and they separate only after a month. If this does not happen, then there is already a threat of miscarriage. If an unauthorized miscarriage does not occur, the child is born with a defect, which is called esophageal atresia. The consequences of such a disease can be fatal if this problem is not surgically solved.
Fetal esophageal atresia – causes:
- alcohol addiction;
- smoking addiction;
- drug addiction;
- conducting an x-ray examination during the first trimester of pregnancy;
- pregnancy after 35;
- use of antibiotics or cytostatics in the first trimester of pregnancy;
- possibility of radioactive exposure;
- poor environmental background;
- the possibility of exposure to chemicals and poisons during work;
- chromosomal disease, etc.
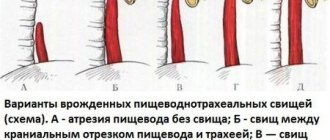
Classification of esophageal atresia
There are several types:
- With isolated type.
- Fistula type - with canals connecting body cavities.
The latter, in turn, is divided:
- the absence of channels that connect the distal esophagus and trachea;
- the absence of channels that connect the proximal esophagus and trachea;
- the absence of channels that connect both ends of the esophagus and trachea;
- for isolated esophageal atresia without fistula.
Abnormalities of the esophagus are the most severe and are often incompatible with life unless surgical intervention is performed first.
Atresia of the ear
Atresia of the auricle is characterized by the complete absence of the ear canal and can be congenital or acquired. The congenital form of atresia occurs simultaneously with an anomaly in the development of the auricle. Diseases that can lead to a sharp narrowing of the ear include inflammatory processes in the walls of the ear. For example, when the skin of the ear canal is irritated by pus that comes from the middle ear. Atresia of the auditory canal occurs due to scarring of its walls after a traumatic injury (gunshot wound, blow) or burn. Ear atresia is clinically manifested by hearing loss due to damage to the sound-conducting apparatus; treatment of this disease consists of artificial restoration of the ear canal using plastic surgery.
Tracheal atresia
We are talking about an anomaly during its development, where its lumen is completely or partially absent. If a newborn has such a defect, he dies immediately after birth. There is a primary and secondary defect. In addition, they are divided into:
- common type (generalized hypoplasia);
- segmental type (circular) of various lengths, which is located at any level of the trachea;
- funnel-shaped, gradually tapering.
Pulmonary atresia is considered to be the absence of part of the connection between the right ventricle and the pulmonary arterial bed. Pulmonary atresia in newborns occurs due to:
- Formation of the pulmonary trunk during division of the common arterial;
- Formations of the right and left pulmonary arteries from the sixth pair of aortic arches;
- Formation of arterial vessels from the lung primordia.
The pleura is lined along the walls of the chest cavity and the outer surfaces of the mediastinum, which protects the lung and pulmonary arteries, bronchi and nerves. Pleural atresia is also one of the anomalies in newborns that has to be corrected surgically.
Atresia of the rectum and extrahepatic ducts
With an anomaly in the formation of the lower intestine, the organ is characterized by underdevelopment of the rectum. Being a congenital defect, intestinal atresia is also accompanied by the absence of the anus. These intestinal abnormalities belong to the group of congenital defects, such as:
- atresia of the biliary ducts;
- liver atresia;
- biliary atresia of the liver;
- esophageal atresia, etc.
At the birth of a child, other anomalies sometimes appear. When a child is really yellow in color with a greenish tint, and liver failure develops over a short period of time, this is a sign that the baby has biliary atresia or, as it is called, biliary atresia. Extrahepatic ducts are clogged or absent and prevent the liver from functioning normally. If such a child is not treated, his life cycle will not exceed a year.
The same applies to duodenal defects, and renal atresia without surgical intervention will further shorten the life cycle.
Heart defects
Heart defects are considered a severe congenital anomaly, which is characterized by the absence of an internal septum between the right atrium and the right ventricle, or a defective atrial septum, or various types of hypoplasia (tricuspid atresia). It is this defect that actually accounts for a third of all heart defects. According to the International Classification of Diseases (ICD), the following heart defects are also distinguished:
- tricuspid valve atresia;
- mitral valve atresia;
- tricuspid atresia.
Each heart defect is most often accompanied by two main factors - an increase or decrease in the blood flow that the heart pumps through itself. Most often, mortality of patients with these defects occurs from the first week to one year after birth. Therefore, surgical intervention is a necessity.
Follicular atresia
During puberty, follicles form in a girl's ovaries. The number of primordial follicles is more than three hundred thousand. But no more than 400 reach (and ovulate) their full maturity. The stage of development of other follicles is inhibited, although each of them can release an egg. This is follicular atresia. There is also cystic atresia of the ovarian follicles. This is one of the common types of illness in women. Polycystic ovarian degeneration begins. It should be borne in mind that the concept of “ovarian atresia” is incorrect, because in fact we are talking specifically about the follicle.
When discussing the female reproductive system, it should be noted that a woman may be susceptible to other anomalies. The most common:
- urethral atresia
- cervical atresia
- atresia of the cervical canal in postmenopause
Uterine atresia occurs exclusively in women. From a medical point of view, it represents overgrowth and obstruction. During menstruation, this anomaly is accompanied by pain. During a gynecological examination, the doctor can additionally detect the development of hematometra and hematosalpinx, and in more severe cases, pyometra and pyosalpinx. Treatment is exclusively surgical.
At the entrance of the cervix there is a space called the cervical canal. It stretches, but only during reproductive age. During menopause, the opening from the vagina into the sterile uterus decreases in both length and width. This change is caused by a hormonal disorder, which is inevitable during menopause (a natural process), and is called atresia of the cervical canal in postmenopause.
Treatment of anal and rectal atresia
Correction is carried out exclusively surgically, so the child will need to consult a surgeon. The operation consists of artificially forming the anus; its complexity depends on the severity of the defect. Without surgical intervention, the child dies by the end of the first week of life. The prognosis of therapy is positive in 30-40% of patients, 11-60% of operations are accompanied by death. In case of delayed passage of feces or complete atresia, surgical intervention is necessary in the first two days after birth. For other types of it, proctoplasty and sigmostoma are performed. Closure of fistulas is carried out from the age of six months to two years. In the postoperative period, constant monitoring of the child’s diet and bowel movements is indicated. There may be a need for enemas, antibiotics, and physiotherapeutic measures.