Share information with your Facebook friends
VK
Patients who have undergone endoscopy are concerned about the circumstance that arises as a result of a biopsy of the esophageal mucosa and is reflected in the histological report with the term “esophageal leukoplakia.”
Today, in order to take a critical and constructive approach to this term, it is necessary to understand and accept the following provisions not only for the patient, but also for doctors who present the definition of “esophageal leukoplakia” to the public:
- Leukoplakia is only a clinical term used to designate a white spot or plaque that occurs on the surface of the mucous membranes with squamous epithelium, which is not removable and cannot be characterized clinically like any other disease (for example, syphilis, lichen planus, lupus, etc. .).
- Leukoplakia has a wide range of possible histological appearances. This may be some degree of thickening of the upper layers of the epithelium (hyperkeratosis), thickening of the middle zone of the epithelium (acanthosis) or atrophy, inflammatory cell infiltration, dysplasia or cancer.
- Like any condition, the histological manifestations of leukoplakia can be of the nature of a normal simple lesion or atypical. In simple leukoplakia, normal squamous epithelium is found. With atypical leukoplakia - atypical epithelium, with dysplasia.
Leukoplakia of the oral cavity: causes of the disease
The reasons causing the development of the disease include:
- Smoking. When using tobacco, the oral cavity is exposed to various irritants, including thermal (incoming smoke has a temperature of about 60 degrees Celsius) and chemical (nicotine, tar and combustion products). No less dangerous is chewing tobacco, which is also a provoking factor.
- Eating either very hot or very cold food on a regular basis for a long time.
- Mechanical trauma (bad bite, sharp edges of teeth, orthopedic structures installed with violations).
- Metal seals that cause galvanic currents.
- Inhalation of vapors of gasoline, benzene, varnishes and paints, as well as other resins.
- Hormonal imbalance, constant stress and lack of retinol.
Symptoms
The first signs of the disease often go unnoticed because they do not cause any pain or discomfort in the patient. Nevertheless, a specialist will be able to determine the onset of leukoplakia by the appearance of the mucous membrane, lips and the area where the teeth meet.
The first sign of the disease is the appearance of a keratinized gray area, which can appear on the palate (in smokers), in the corners of the mouth, on the inside of the cheek, etc. An easily removable white plaque forms in this area, but after a few days the formation makes itself felt again . The patient may feel tightness in the mouth, but, as practice shows, most people simply do not pay attention to this.
Plaques with a diameter of no more than 4 centimeters are formed. They may appear:
- on the inner surface of the cheeks;
- on the tongue (on the back or sides);
- in the sky;
- on the gums;
- in the corners of the mouth.
The process of plaque formation takes up to one month. At the first stage, the area of the future formation seems slightly swollen; when you feel it with your fingers, the compaction is not felt. However, over time, another symptom of oral leukoplakia appears - the mucous membrane at the site of the swelling loses its original shine and becomes rough, which is noticeable when touched.
There is no pain in this case: only sometimes a feeling of dryness at the site of the outbreak is possible.
Gradually, the color of the spots changes from gray to bright white. The spots in most cases have clear boundaries. Their increase is possible when the disease enters its second stage, called verrucous.
The disease often causes candidiasis and malignant cancers. In an advanced state, leukoplakia is very difficult to treat: the affected areas become even more keratinized, ulcers can form, and the infection gradually spreads to other areas of the mouth.
Treatment methods
Treatment of leukoplakia may require a collegial approach: the participation of the oncologist in developing an action plan. The basis of therapy is the elimination of provoking factors: quitting smoking, changing jobs due to occupational hazards, following a soft diet with no spices, etc. According to indications, correction of dentures, replacement of fillings, treatment of caries, removal of teeth that cannot be restored and other measures are carried out .
As part of complex treatment, the doctor may prescribe the following medications:
- Preparations for restoring the normal structure of the oral epithelium. It is usually used in the form of applications to the affected areas.
- Antiseptics. Used for the prevention and treatment of inflammatory complications of the disease.
- Painkillers and symptomatic therapy. Systemic medications or applications of local anesthetics used in dentistry may be used.
Self-medication for leukoplakia in the mouth is strictly not recommended. Many drugs, including some anti-inflammatory drugs, are irritating and increase the risk of developing malignant tumors.
If the disease is severe, hospitalization may be required. The presence of ulcers and erosions is an indication for the use of hormonal anti-inflammatory drugs, proteolytic enzymes, etc. Surgery is indicated when conservative treatment is ineffective. Cryodestruction and excision with a scalpel are usually used.
Kinds
- The most common is simple or, as it is also called, flat leukoplakia . It is usually discovered by chance during an examination by a dentist, since the patient does not experience any subjective sensations. A burning sensation occurs extremely rarely, and the appearance of the mucous membrane may change. If the disease affects the tongue, loss of taste may occur.
- Hairy leukoplakia of the tongue resembles stomatitis. The shape of the spot that appears, as well as its size, can be different, the color - from pale gray to white. The surface of the mucous membrane at the site of the lesion becomes slightly rough, which can be felt to the touch. On the cheeks it appears as solid or broken lines. It can also be found on the lips, where it looks like thin paper pasted on.
- Verrucous leukoplakia is the second stage of the development of the disease. The keratinization thickens, the affected area seems to rise above the nearby tissues. When you touch it with your fingers, you feel a compaction.
- Erosive form . Untimely diagnosis of the two previous stages of the disease leads to a worsening of the situation - the person feels pain when exposed to any irritants, erosions or ulcers are visible in the mouth.
- Soft leukoplakia is a type of cancer. Its distinctive feature is peeling of tissue in the area of the lesion. To clarify the diagnosis, a histological method of studying cells is required.
- Tappeiner's leukoplakia . This form of the disease affects people who abuse smoking. According to studies, daily smoking 10 cigarettes a day increases the chance of developing the disease by 50 times (as the number of cigarettes increases, the risk also increases)
The disease begins with the formation of lesions on the roof of the mouth (sometimes they appear on the gums). The mucous membrane changes its color to a pronounced gray or bluish, which is noticeable to the naked eye, folds appear on it. Reddish nodules may begin to appear, which is accompanied by infectious inflammation of the oral cavity (caused by the accumulation of salivary gland secretions in the tissues).
Diagnosis of oral leukoplakia
Treatment of any disease begins with diagnosis: leukoplakia is no exception in this regard.
During the examination, the doctor interviews the patient to determine the factors contributing to the development of the disease. These include regular exposure to tobacco smoke, working in hazardous conditions, recent dental surgery, etc.
Next, laboratory tests are prescribed. The following procedures can be carried out:
- tissue sampling (biopsy). Accompanied by anesthesia;
- examination of the collected material under a microscope. The method allows you to determine the presence or absence of cancer cells in the formation;
- a smear of the mucous membrane is taken;
- A Schiller test is done (the mucous membrane is stained with a solution consisting of water and iodine - foci of leukoplakia are not stained);
- blood is taken for analysis (an increase in ESR may indicate the presence of malignant neoplasms).
In addition, the doctor may additionally prescribe a urine test, conduct a biochemical blood test and request the result of fluorography. You may need to consult an oncologist (if cancer is suspected), a therapist (to rule out infectious diseases) and a dermatologist (to look for other foci of disease).
Diagnosis of the disease
The diagnosis is made based on examination and questioning of the patient. Mandatory diagnostic studies confirming the diagnosis include:
- Cytology is the collection of epithelial cells to identify cancerous lesions.
- Histology is taken to perform a biopsy, which allows examination of the affected epithelial tissue to detect cancer cells.
- Blood from a vein.
Additional clarifying studies make it possible to distinguish leukoplakia from other pathologies.
Leukoplakia of the oral cavity: treatment with medications
Treatment involves the complete elimination of irritating factors that led to the development of the disease:
- to give up smoking;
- grinding down sharp edges of teeth;
- sanitation of the oral cavity;
- replacement of fillings;
- use of products to protect the surface of the lips.
Additionally, a course of vitamin A is prescribed, lasting at least a month, which inhibits the process of tissue keratinization.
If the measures taken do not cause complete disappearance of the manifestations of the disease, surgical intervention is allowed: the lesion is excised, depending on the degree of development of the disease, cryodestruction or electrocoagulation is used.
Ulcers deserve special attention, as they can develop into cancerous tumors. For their treatment, drugs are prescribed that enhance the process of tissue regeneration and epithelization. If there is no positive dynamics, surgical intervention cannot be avoided.
A person with leukoplakia must constantly visit the dentist for examination to prevent malignant degeneration of the cells.
In addition to quitting smoking, the patient’s diet is adjusted: during treatment, spicy and too salty foods are excluded from the diet, and it is recommended to eat more vegetables and fruits.
Drugs prescribed:
- products that restore the epithelium (the most effective was 30 percent tocopherol acetate, which is applied to damaged areas three times a day for 15 minutes, after which it is washed off with water);
- antiseptics (after each meal it is recommended to rinse your mouth with a solution of chlorhexidine at a concentration of 0.05%);
- analgesics (their use is justified in the presence of pain. Lidocaine, applied to the mucous membrane before meals, has worked well).
Under no circumstances should you use drugs that have an irritating effect, as otherwise this can lead to the formation of cancer cells.
If there is no improvement within a couple of weeks, surgery is prescribed: this can be either excision with a scalpel or the application of cold in the form of a liquid stream of nitrogen.
Causes
Different localizations of leukoplakia are caused by different reasons and require an individual approach in developing a treatment strategy.
Hairy leukoplakia develops against a background of reduced and weakened immunity, so most often this type of disease is diagnosed in patients with HIV, various immunodeficiencies and during rehabilitation after organ transplantation, when a course of immunosuppressants is prescribed.
- Leukoplakia of the external genitalia in women develops most often during menopause, when reverse development processes occur in tissues and cells. Mucous tissues and skin become drier, hair loss is observed, which is a normal physiological process.
- Leukoplakia of the esophagus develops after heartburn or burns of the mucous membrane of this organ; more than half of the cases of this disease cause the appearance of a cancerous tumor.
- Leukoplakia in the oral cavity is most often localized on the mucous membranes of the inner side of the cheek, the hard and soft palate, as well as in the angular folds of the mouth. Leukoplakia of the tongue is extremely rare in medicine.
To this day, official medicine does not know the exact reasons for the development of this disease in the mouth. However, a number of factors have been identified that increase the chances of developing leukoplakia:
- metabolic disorders;
- genetic predisposition;
- lack of vitamin A;
- smoking;
- chronic injuries to the mucous membranes (for example, due to improperly manufactured dentures);
- activities associated with direct contact with coal and coal tar, as well as their processing processes;
- HIV and AIDS;
- chronic inflammatory processes in the mouth associated with neurological disorders.
Leukoplakia of the bladder is a protracted chronic disease that is characterized by the degeneration of transitional epithelial cells into squamous epithelial cells. The keratinized epithelium is unstable to urine components, which causes inflammation in the bladder cavity. The main cause of the development of the disease is ascending infection with sexually transmitted pathogens. Therefore, leukoplakia in the bladder develops more often in women - their urinary canal is much shorter than the male one, so it is easier for infections to penetrate through it.
In some cases, the cause of leukoplakia can be a downward infection, when a pathogen penetrates through the bloodstream from nearby organs: staphylococci, Proteus, streptococci, E. coli and others. The development of the disease is favored by:
- chronic diseases of the abdominal organs located next to the bladder;
- all factors that reduce immunity: hypothermia, stress, bad habits, chaotic lifestyle;
- foci of chronic inflammation located at a distance from the bladder: tonsillitis, caries, sinusitis, etc.;
- disturbances in the functioning of the endocrine system;
- the IUD was not removed in time in the uterine cavity;
- promiscuous sex life without the use of barrier contraception.
Leukoplakia of the cervix is called whitish formations (spots or plaques) that appear on the mucous membrane. To diagnose the disease, a preventive examination using a gynecological speculum is sufficient.
Like dysplasia, cervical leukoplakia requires mandatory treatment, since it is a precancerous disease. There are many reasons for the appearance of such tissue changes:
- decreased immunity for various reasons;
- injuries due to careless examination, termination of pregnancy, childbirth;
- interruptions in the functioning of the endocrine system;
- ovarian dysfunction;
- current or previous infectious diseases of the genital organs.
Oral leukoplakia: how to treat it at home
In addition to drug treatment, oral leukoplakia can be treated with traditional medicine.
There are many recipes, here are just the main ones:
- rinsing with herbs (infusions of oregano, chamomile, ginseng and other adaptogens that reduce the inflammatory process and increase the body’s resistance to harmful factors are suitable);
- regular consumption of nuts and tinctures based on them;
- rinsing with decoctions of calendula, St. John's wort, eucalyptus. Alternation works well - once the oral cavity is rinsed with a soda solution, after a couple of hours - with an infusion of herbs. This procedure should be repeated at least 5 times a day;
- lubricating the lesions with sea buckthorn and olives (the fruits must first be mashed in your hands so that the juice appears).
Timely detection of the disease and compliance with all doctor’s recommendations is the key to recovery in the shortest possible time and reducing the risk of complications. If you start treatment at the initial stage, you can reduce the likelihood of complications to almost zero.
Leukoplakia is a keratinization of the oral mucosa (OM), accompanied by inflammation of the stroma and usually occurring in response to chronic exogenous and endogenous irritations [15, 35].
The term “leukoplakia” was first used in the works of Schwinmer (1977), although detailed clinical characteristics of this process were proposed in the second half of the 19th century under different names: ichthyosis, psoriasis, keratosis, etc. [15, 41].
Epidemiology of leukoplakia of the oral mucosa
The overall prevalence of leukoplakia SOP, according to American authors, is 0.5-3.46%, and the incidence of malignancy is 0.7-2.9% [108]. Leukoplakia SOP is more common in India and the southern states of America, where smoking and other use of tobacco and betel nut are more common than elsewhere [81, 96, 116].
Leukoplakia SOP is usually diagnosed in middle age, and the prevalence of the disease increases over the years. Idiopathic leukoplakia of the oral cavity accounts for 10% of cases, and leukoplakia caused by exogenous and endogenous factors accounts for 90% [125]. Men are more often affected than women. The mucous membrane of the cheeks is affected in 25% of cases, the gingival edge of the jaw - in 20%, the tongue - in 10%, the floor of the mouth - in 10%; other areas account for the remainder of the lesions [77, 78, 121, 126].
Etiology and pathogenesis of leukoplakia SOP
There are many studies devoted to this disease [6, 36, 40, 48, 54, 80, 94], but the question remains open about the causes of abnormal keratinization of the oral cavity. Many authors [30, 49, 12, 123] consider tobacco smoke or chewing nas, hot food and alcohol to be one of the main exogenous factors. However, in some sources you can find a description of leukoplakia in patients who never smoke or rarely smoke [118, 134]. Hot, hot, spicy foods can also cause the development of the disease. With strict dietary restrictions, it is possible to prevent the development of leukoplakic plaques, and sometimes even cause their complete disappearance.
The reasons for the development of leukoplakia can be chronic traumatization of the oral cavity by sharp edges of decayed teeth, improperly manufactured dentures, or galvanic current that occurs in the presence of dentures made of dissimilar metals [19].
A certain role in the etiology of leukoplakia of the lower lip belongs to glandular cheilitis in combination with unfavorable meteorological conditions, as a result of which the red border is subject to constant irritation [7, 127]. In addition, when leukoplakia is localized on the red border of the lips, chronic injury from a mouthpiece, cigarette, pipe or cigarette is of great importance.
Leukoplakia SOP can occur as an occupational disease in people working in chemical production or in workshops with high temperatures [122].
Considering leukoplakia as a reaction of impaired keratinization of the oral cavity to various external stimuli, one cannot deny the influence of endogenous factors, which, in turn, disrupt the resistance of the mucous membrane to external stimuli [93].
The decrease in resistance, apparently, may be associated with pathology of the gastrointestinal tract - GIT [12]. According to other authors [13, 85], chronic gastritis, gastric and duodenal ulcers were observed in 90.3% of patients observed for leukoplakia, but the clinical picture of leukoplakia and gastrointestinal pathology did not reveal significant parallels between them.
Lack or disturbance of the metabolism of vitamins A and E, the role of which in the process of keratinization is well known [45, 58, 99], may be one of the causes of leukoplakia.
Some authors trace a connection between the development of leukoplakia and chronic candidiasis infection [72, 132]. During its life activity, Candida albicans
forms N-nitroso-benzymethylamine (NBMA), which can promote malignancy of leukoplakia lesions [62, 67, 70, 111].
Ya.L. Makarov (2004), R.I. Stryuk (2008) assigns a certain role in the occurrence and malignancy of the disease to endocrine disorders. Thus, when examining patients with leukoplakia, diabetes mellitus types 1 and 2 were detected in 15% of cases. And in women, in some cases, there was a connection between changes in progesterone levels and the occurrence of leukoplakic plaques in the mouth.
Genetic factors occupy a certain place in the pathogenesis of leukoplakia SOP, which is confirmed by the development of this disease in patients with congenital and hereditary dyskeratoses. The risk of developing leukoplakia was associated with p53 protein expression and the simultaneous presence of the GSTM1o and GSTT1o genotypes.
Currently, the question of whether there is a connection between the occurrence of oral leukoplakia and the detection of human papillomavirus (HPV) remains controversial [46, 47, 114].
HPVs that infect the oral cavity are divided into low-risk viruses for malignancy (HPV 6, 11, 13, 32) and high-risk (HPV 16, 18, 31, 33 and 35) [53, 97].
This division of HPV is universal for studies of oncogenic significance in all areas of the upper digestive tract [56, 68].
According to foreign authors [79, 110], high-risk viruses, especially HPV 16, were detected in verrucous leukoplakia. The probability of the presence of HPV in the intact mucosa in patients with simple leukoplakia and leukoplakia verrucous was 10, 20.2 and 26.2%, respectively [129].
In addition to the above, in patients suffering from various forms of leukoplakia, an imbalance of the immune system was sometimes detected [43, 102], characterized by the appearance of cytotoxic lymphocytes and macrophages in the peripheral blood. Interleukin-2 alone or in combination with monocytes exhibited increased cytotoxicity, especially in verrucous leukoplakia. When studying immune complexes in people chewing tobacco, compared to controls, their number was slightly higher, and the activity of natural killer (NK) cells decreased. Thus, it is possible that T-cell-mediated cytotoxic reactions may occur in leukoplakia, which is apparently explained by the general immunological response to the oncogenic form of the inflammatory process in the mouth [113].
Summarizing the data on this issue, it should be noted that this information is contradictory and fragmentary.
Clinical and morphological characteristics of leukoplakia
The clinical picture of leukoplakia depends both on the form of the disease and the factor causing it, as well as on the location. The course of leukoplakia from the moment of its appearance to the onset of malignancy is characterized by several stages [32, 115].
The process usually begins with the so-called pre-leukoplakic stage, which is characterized by inflammation of the oral cavity, and extremely rarely this stage can be observed on the red border of the lips [16].
Then flat leukoplakia develops, which is a uniform keratinization of a limited area of the mucous membrane, which is the result of epithelial hyperplasia and is accompanied by chronic inflammation of the stroma. More often, foci of flat leukoplakia are located on the mucous membrane of the cheeks, in the corners of the mouth, sometimes on the floor of the mouth, having the appearance of a plaque of color: from grayish to grayish-white; the plaque does not rise above the level of the surrounding mucous membrane and is not removed by scraping.
As the process progresses, foci of leukoplakia begin to rise above the level of surrounding tissues and can take on a lumpy appearance. Such a lesion is characteristic of verrucous leukoplakia.
Verrucous leukoplakia comes in two types: plaque and verrucous. In both of these forms, the plaques are grayish-white or milky in color, sharply protruding above the surrounding mucosa, and have a dense consistency upon palpation. Localization of lesions is most often the dorsal and lateral surface of the tongue, the buccal mucosa, rarely - the lingual surface of the alveolar process and the floor of the mouth. Malignancy is observed in 20–23% of cases [91, 130].
With the verrucous form of leukoplakia, cracks and erosions may appear, which are systematically exposed to thermal or mechanical irritation. This is the so-called erosive form, the most prone to malignancy (up to 25-27% of all cases of other forms of leukoplakia) [34].
Tappeiner's smokers' leukoplakia, or nicotine stomatitis, occurs mainly on the mucous membrane of the hard palate in patients who smoke regularly and frequently use a pipe. The mucous membrane of the hard palate is whitish or white, against which reddish dots are clearly visible - the gaping mouths of the excretory ducts of the minor salivary glands. This disease was described by Grutz in 1928, and in 1941 Thoma described a similar clinical picture called “nicotine stomatitis”. But in 1949, it was Tappeiner who gave a detailed clinical and histological description of this form of leukoplakia, noting that this pathology is based on damage to the excretory ducts of the minor salivary glands, and not the salivary glands themselves.
A characteristic feature of leukoplakia, found in all its forms, is diffuse inflammation, often accompanied by significant infiltration of the upper part of the stroma [103].
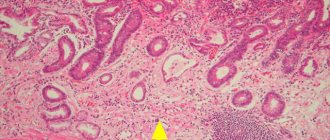
In the flat form of leukoplakia, parakeratosis is observed, the thickness of the spinous layer is 40-50 rows of cells, and acanthosis is noted. There is no granular layer. Thus, parakeratosis in leukoplakia is often combined with epithelial hyperplasia.
With verrucous leukoplakia, severe hyperkeratosis is determined, rarely combined with small foci of parakeratosis, sometimes the stratum pellucida is involved in the pathological process; the granular layer consists of 4-5 rows of cells with well-defined granularity, the spinous layer - of 8-12 rows of cells. Sometimes atypical cells are detected. In some cases, acanthosis is expressed, accompanied by elongation and expansion of epithelial processes.
Much more often, such discomplexation of the cells of the spinous layer and cellular atypia are expressed in the erosive form of leukoplakia, in which the inflammatory reaction in the stroma reaches a maximum (dilated lymphatic and blood vessels, a sharp change in the walls of deep-lying stromal vessels) [92].
When malignancy of leukoplakia begins, in addition to the elongation of epithelial processes far beyond the physiological border, discomplexation of the cells of the lower rows of the spinous and basal layers, destruction of the basement membranes is observed, and an increase in the number and size of nucleoli in the cells of the lower rows of the spinous layer occurs.
Thus, the features of malignant transformation of the epithelium of the oral cavity can be difficult to assess, so it is necessary to look for additional diagnostic criteria that allow more accurately determining the degree of dysplasia of the epithelium of the oral cavity [18, 42, 103].
Currently, to diagnose dysplasia of the epithelium of the oral mucosa, an immunohistochemical (IHC) method is used, which makes it possible to more accurately determine the degree of dysplasia (SIN1, SIN2, SIN3). Markers of malignant transformation are the Ki-67 protein, the acanthosis marker - p53 protein, the cytoskeletal proteins - cytokeratin-8 and -19, E-cadherin and β-catenin, as well as the basement membrane protein - type IV collagen and the enzyme that breaks it down - matrix metalloproteinase-9. Histological and IHC research methods are necessary for the diagnosis of various forms of leukoplakia.
One of the main trends in modern medicine is the improvement of non-invasive methods for diagnosing pathological processes accompanied by changes in tissue structure. The standard method, as already mentioned, is histological examination of tissue biopsies. Taking a biopsy from the periphery of the tumor, where all stages of the process from cancer in situ to dysplasia of various degrees can be observed, according to G. Ghurani (2001), is the most common cause of false negative biopsy results. Therefore, information about the internal structure of biological tissues is important both for diagnosing diseases and for adequate monitoring of treatment results.
Routine imaging methods - computed tomography and magnetic resonance imaging - allow one to assess the structural features of tissues with a spatial resolution of no higher than 100-1000 µm [60, 128]. Recently, attempts have been made to bring the resolution of methods closer to the cellular level (≈10 μm), which became possible for nuclear magnetic resonance, confocal optical microscopy and optical coherence tomography (OCT) [39, 51, 52, 57, 65, 66, 105 ].
The essence of the OCT method is to display the structure of biological tissues of the body (in particular, the SOP) in a cross section with a high level of resolution, which provides intravital morphological information at the microscopic level. The operation of OCT is based on the principle of low-coherence interferometry [17, 20, 28, 71].
Possessing all of the listed characteristics, OCT in the coming years may find wide application in dentistry as a non-invasive method for diagnosing various degrees of oral dysplasia.
Treatment of leukoplakia SOP
Treatment of leukoplakia is a difficult task, since this disease is a precancerous condition [37]; it is necessary to talk about a differentiated medical approach to different forms of the disease, because each of them has a different potential for malignancy. It follows that treatment methods can be divided into: medical, surgical and combined [74].
However, an indispensable condition for the treatment of various forms of leukoplakia is, first of all, the cessation of exposure to exogenous stimuli. This primarily applies to smoking, chewing tobacco, drinking alcohol and eating irritating, hot and spicy foods.
No less important in the treatment of leukoplakia is sanitation of the oral cavity, removal of decayed teeth, grinding of sharp edges of teeth, orthopedic treatment, including rational prosthetics and replacement of dentures made of dissimilar metals.
Local treatment consists of prescribing keratoplasties (vitamin A, E, β-carotene), which normalize the processes of keratinization and improve metabolism in the affected tissue.
A number of authors note a pronounced effect of topical application of antifungal agents (10% borax in glycerin, Clotrimazole cream, etc.). J. Epstein, F. Wong [64] used the cytostatic drug bleomycin locally as an additional treatment for severe forms of leukoplakia SOP, when surgical excision for one reason or another was impossible.
General drug therapy includes the administration of large doses of vitamin A. It is known that vitamin A helps normalize the synthesis of DNA and RNA of epithelial cells, accelerating the proliferation and differentiation of keratinocytes.
Currently, vitamin A derivatives—retinoids—are widely used [64]. By influencing the genetic apparatus of the cell, they normalize the processes of proliferation and differentiation of the epithelium and mesenchyme, and affect the condition of cell membranes.
In medical practice, tigazone is used, isatretinoin (13-cis-retinoic acid) in a daily dose ranges from 25 to 50 mg; course of treatment up to three weeks.
In addition to vitamin A and its analogues, some authors [38, 117] prescribe vitamin E and C in combination with B vitamins and folic acid. It is well known that vitamins B and C are natural antioxidants, regulate redox reactions, regenerate tissues, normalize hypoxin and regulate cell proliferation processes.
As mentioned above, work in recent years indicates the role of some biotypes of Candida albicans in the processes of malignancy and a decrease in local immunity, which contribute to the development of leukoplakia, therefore the inclusion of anti-candidiasis drugs in the treatment process is justified [100].
A number of authors [89, 95] include general antimycotic agents (Flucostat, Diflucan, Nizoral, etc.) in complex treatment. The drugs are prescribed orally for 7-10 days, the dose varies from 50 to 100 mg/day.
Some domestic and foreign authors [11] in their works in the treatment of leukoplakia SOP mention drugs called “adaptogens,” in particular the phytomixture Fitomix-40. This drug contains 40 components that have anti-inflammatory, diuretic, choleretic, and sedative effects.
According to the work of I.K. Evseeva [10], drugs such as clanin and phytolan were included in the complex treatment of leukoplakia SOP. Belonging to the group of dietary supplements, they are made from extracts of pine needles and kelp and have pronounced antioxidant properties. The drugs are taken 2 tablets 3 times a day or 50-60 drops 2-3 times a day after meals.
Speaking about the occurrence of leukoplakia in men and women at a certain age, L.V. Petrova et al. (2004) used the drug spironolactone, which is a competitive antagonist of aldosterone. The drug was prescribed at 200 mg/day with a gradual dose reduction to 50 mg/day. General course - 4 months.
The works of some authors [24], as indicated above, are devoted to the detection of changes in the gastrointestinal tract and diabetes mellitus in patients with oral leukoplakia; therefore, treatment of these background types of pathologies is necessary. B.M. Pashkov (1969), A.L. Mashkilleyson [15], V.M. Abramova (1984) recommend treatment of patients with leukoplakia SOP by a gastroenterologist, endocrinologist, general practitioner with the prescription of drugs panzinorm, pyridoxine and their analogues.
Based on the results of studies on disorders in the immune system in patients with leukoplakia SOP, a number of authors [98, 107, 131] used interferon-α, which, in their opinion, controlled the course of leukoplakia and prevented its malignancy, which can probably be associated with its effect on NK activity.
Thus, the data presented indicate that the elimination of exogenous factors and the use of local therapy gives a positive result in the treatment of flat leukoplakia and Tappeiner’s leukoplakia. In severe forms of leukoplakia, in addition to local therapy, the prescription of general medications and surgical treatment methods is required. Surgical intervention, especially for verrucous and erosive forms of leukoplakia, is a common method of treatment today [2-5], especially when the size of the lesion allows it to be excised within healthy tissue and at the same time it is possible to conduct a thorough histological examination to identify the onset of malignancy of leukoplakia [133] .
According to some authors [69], the main method of surgical treatment is excision of the area of leukoplakia with a scalpel. It should be noted that this method is indicated when the size of the leukoplakic lesion clearly contours to the healthy mucosa and access to them is not difficult.
At one time, electrocoagulation and cryodestruction, which can be classified as physical methods of treating leukoplakia, were widespread [84, 101, 106].
A number of authors [73] have successfully used helium-neon laser in combination with cryotherapy on lesions. L. Gaspar, G. Szabo (1990) used laser surgery in 126 patients with leukoplakia SOP and clinical cure was obtained in 118. But subsequently, in 98 patients, within 5 years, a relapse of the disease occurred at the previous sites of the lesion. A relatively high relapse rate was observed by M. Schoelch et al. (1999): 41 out of 70 patients had a relapse, and 5 had malignancy of the process.
Nevertheless, laser surgery is widely used in the treatment of this pathology of the oral cavity [44]. The use of modern laser methods [50, 104, 109] makes it possible to achieve high-quality results in the treatment of severe forms of leukoplakia (verrucous and erosive).
The rapid development of laser technologies in the 90s of the last century made it possible to introduce into widespread practice gentle, minimally invasive methods of treating leukoplakia SOP, one of which is photodynamic therapy (PDT) [8, 33, 60].
PDT is based on the ability of a photosensitizer to selectively accumulate in tumor tissue [21, 22, 26, 29]. In the presence of oxygen, under the influence of laser light with a wavelength corresponding to the type of absorbed photosensitizer, a photochemical reaction develops, which leads to the formation of singlet oxygen and other oxidants, followed by selective death of tumor cells. Healing of the tissue defect occurs with the formation of a gentle scar, which preserves the surrounding healthy tissue [55, 120].
In Russia, the domestic drug Photogem is used for PDT [23, 25], developed at the Moscow State University of Fine Chemical Technologies named after. M.L. Lomonosov, as well as the photosensitizer Photoditazin, which has several absorption bands at wavelengths of 400, 504, 534, 608 and 662 nm.
A number of authors used Photosan, administered intravenously at a dose of 2.0 mg/kg in a darkened room. The PDT session was performed 3 hours after drug administration; The irradiation time for 1 field was 10 minutes, the power did not exceed 167 mV/cm2. As a rule, a delicate whitish scar formed at the site of the resorbed tumor.
Currently, PDT is used as a stand-alone method or in combination with chemoradiotherapy or combined treatment for cancer of the oropharynx, oral cavity, tongue and lower lip [59, 60, 81]. PDT has shown positive results in the treatment of leukoplakia SOP as a precancerous disease [27, 83, 87, 88].
A number of American scientists [75, 86, 119] attempted to treat verrucous leukoplakia using local PDT with the photosensitizer Photofrin and ALA.
Today, PDT is approved by oncologists as a method of polytherapy for the initial stages of cancer, “inconvenient” localizations of lesions on the face, ears, as well as for combined and complex treatment in cases of recurrent cancer of the skin, lower lip and tongue [124].