Antibiotics are substances of biological or semi-synthetic origin. They are used in medical practice to combat pathogenic microbes and viruses. Before the advent of these medications, typhoid fever, dysentery, pneumonia, and tuberculosis had the status of incurable diseases. Today, treatment of infectious diseases is possible with the use of 1-6 generations of antibiotics.
At this moment, the pharmacological industry produces more than 2000 varieties of drugs of this type. Doctors have described the effects of about 600 positions, and about 120-160 drugs are used in medical practice.
Important! For any disease, it is recommended to take antibiotics after consulting a doctor. Otherwise, antibiotic resistance may develop (decreased sensitivity of pathogenic microorganisms to antibacterial agents).
Classification of antibiotics
All antibacterial agents can be divided into 5 categories according to their characteristics and range of application. Let's take a closer look at this classification:
Mechanism of action:
- Bactericidal - the active substances of the drugs completely destroy bacteria and viruses. After taking such strong drugs, all pathogenic microflora in the human body dies.
- Bacteriostatic – inhibits the growth or spread of viruses. Thus, the cells remain “alive” without forming pathogenic flora.
Diagnosis of gastritis
- General clinical analysis of blood and urine
- Analysis of stool for coprogram
- Biochemical blood test (liver tests, cholesterol, alkaline phosphatase)
- ECG
- X-ray of the chest organs in 2 projections
- X-ray of the esophagus, stomach with barium mixture
- Ultrasound of the hepatobiliary system
- 24-hour pH monitoring in the lower esophagus and stomach
- EGDS
- Non-invasive tests for the determination of Helicobacter pylori (respiratory)
Spectrum of action
There are antibacterial agents:
Part II. Drug treatment of gastritis and gastroduodenitis. Other factors
Part II. Chronic gastritis and gastroduodenitis (end)
V.F. Privorotsky, N.E. Luppova Treatment of gastritis and gastroduodenitis Drug treatment (end)
2. Normalization of the motor function of the upper gastrointestinal tract is carried out with prokinetic drugs, mainly dopamine antagonists. They activate the contraction of the stomach and its transport function, and increase the tone of the LES.
1st generation drugs include metoclopramide (cerucal, raglan), the disadvantage of which is the ability to penetrate the blood-brain barrier and produce undesirable side antidopaminergic effects on the central nervous system in the form of extrapyramidal disorders. This limits the use of metoclopramide in pediatric practice.
Motilium
- second generation drug. Its prokinetic activity is superior to that of metoclopramide, and it does not have the side effects of the latter. Prescribed 0.25 mg/kg body weight 3-4 times a day 15-20 minutes before meals.
3. Increasing the protective properties of the gastric mucosa. The group of drugs that activate the protective properties of coolant includes medicinal substances with different mechanisms of action.
The cytoprotective effect of drugs can be achieved: by increasing the production of protective mucus (liquiriton, licorice root, carbenoxolone, biogastron), by improving the regeneration of the mucous membrane (methacyl, sea buckthorn oil, rose hip oil, solcoseryl, acgovegin, dalargin). Antipeptic drugs have a cytoprotective effect.
Antipeptic drugs. In the pathogenesis of diseases of the stomach and duodenum, in addition to HCl, proteolytic enzymes play an important role. Activation of pepsinogen into pepsin occurs with increased and continuous acid formation, which causes damage to the coolant and mucous membrane of the duodenum. Antipeptic drugs can inhibit the proteolytic effect of gastric enzymes. In addition, these drugs also have a cytoprotective effect. In the acidic environment of the stomach, they form a protective film on the damaged mucous membrane, protecting it from the aggressive effects of acid and pepsin.
De-nol is a cytoprotective drug that, in addition to the listed properties, has the ability to increase blood flow in the gastroduodenal mucosa and increase local endogenous synthesis of PG. As a result, the secretion of mucus and bicarbonate ions increases, which causes a kind of “antisecretory” effect. The drug is widely used in eradication regimens due to its bactericidal properties, which makes it possible to enhance the antibacterial effect of the regimen as a whole. In addition, to date there are no HP strains resistant to de-nol. Prescribed 1/2-1 tablet 4 times (1-2 tablets 2 times) a day 30-40 minutes before meals and at night.
Sucralfate (alsukral, venter). Aluminum, which is part of the drug, ensures its reparative activity and normalizes the processes of evacuation of contents from the stomach. Sucrose sulfate, interacting with the proteins of damaged tissues, forms a protective layer at the site of ulcers and erosion. The antacid effect of the drug is insignificant. Prescribed 1 tablet (0.5-1.0 g) 4 times a day 40-60 minutes before meals and at night.
True cytoprotectors (synthetic analogs of PG) are misoprostol, enprostil, etc. in pediatric practice they are used only in exceptional cases.
4. Helicobacter pylori eradication
We do not consider it advisable to carry out eradication therapy to all patients with HP-positive CGD, regardless of age. The absolute indications for its implementation, in our opinion, are:
1) HP-associated erosive form of gastroduodenitis;
2) CGD with atrophy (subatrophy) of the glands;
3) any endoscopic and morphological variants of CGD in children with a hereditary burden of ulcerative disease and gastric cancer.
Relative indications are:
1) any HP-associated variants of CGD, occurring with severe clinical symptoms and (or) extensive contamination of the gastric mucosa by HP;
2) any HP-associated variants of gastroduodenal pathology in patients who wish to undergo a course of eradication therapy.
The question of the need for eradication therapy in such situations should be decided individually. In all other cases of detection of HP in children, there are, as a rule, no convincing grounds for anti-Helicobacter therapy.
Drugs and regimens for eradication therapy are given in the corresponding section of the BU.
5. Normalization of autonomic homeostasis in children with GDD diseases is carried out according to the principles set out in the corresponding section of GERD.
6. Treatment of concomitant diseases occurs in accordance with the nature of the existing pathology.
Physical therapy treatment is a desirable component of a comprehensive treatment program. It is indicated during any period of the disease. In the acute stage of severe pain, electrophoresis of novocaine, papaverine, and zinc sulfate is prescribed to the epigastric area, including the pyloroduodenal zone.
In the stage of incomplete remission, applications of mud, paraffin, and ozokerite are effective. Considering the importance of the ANS in regulating the activity of the upper gastrointestinal tract, methods for correcting autonomic imbalance are also used, which were already mentioned in the GERD section.
The use of herbal medicine or mineral waters is indicated when the exacerbation subsides or during remission.
For CGD with increased acid-forming function of the stomach, the following herbal preparations are recommended;
1. Celandine (grass) - 10.0 g;
common yarrow (herb) - 30.0 g;
chamomile (flowers) - 25 g;
St. John's wort (herb) - 39 g.
Take 1/3-2/3 cup of decoction 3 times a day 30 minutes before meals.
2. Common fennel (fruit) - 30.0 g; .
chamomile (flowers) - 30.0 g;
cordate linden (flowers) - 40.0 g.
Take 1/3-2/3 cup of infusion 3 times a day 30 minutes before meals.
It is also possible to use herbal mixtures proposed in the GERD section.
For balneological treatment, waters of low and medium mineralization with a predominance of hydrocarbonate ions are usually used - “Borjomi”, “Luzhanskaya”, “Smirnovskaya”, “Essentuki 4”, “Essentuki 17”, etc.
To reduce the increased secretory function of the stomach, mineral water is prescribed at the rate of 3-5 ml/(kg/day) 1.5-2 hours before meals.
If necessary, stimulate the secretory function of the stomach, mineral water is taken in the same amount 20-30 minutes before meals.
A desirable attribute of the rehabilitation program for children with acid-related diseases is sanatorium-resort treatment (see section GERD).
Clinical examination
The issues of medical examination of patients with CG and CGD in pediatric practice have not yet been fully worked out. Previous recommendations require revision to take into account modern requirements.
The frequency of examinations of the child by a local pediatrician and (or) gastroenterologist is determined by clinical and endoscopic data and should be at least 2 times a year.
The need for FEGDS is determined individually, based on clinical and anamnestic data, the results of previous endoscopic studies and the duration of clinical remission.
The secretory function of the stomach is constitutionally determined, and acidity levels in most children have fairly stable values, which makes it possible to avoid the appointment of pH measurements more than once every 2-3 years.
The ideology of anti-relapse therapy is also being revised. The prescription of antacids, antisecretory drugs, prokinetics, etc. during the period of stable clinical and morphological remission is, as a rule, not indicated. Prophylactic administration of these drugs does not guarantee a relapse-free course of the disease. It should be remembered that the prescription of antacids and cytoprotectors is mandatory while taking ulcerogenic drugs.
Autumn-spring courses of herbal and vitamin therapy and balneotherapy can be considered as anti-relapse therapy.
In cases where CGD occurs with frequent relapses, the above therapy should be enhanced by antacids with reparative properties.
The issue of deregistration can be resolved only if a stable three-year clinical and morphological remission is achieved.
Clinical examples
Sasha S., 14 years old, was admitted with complaints of intense, aching-stabbing pain in the abdomen (epigastric region, around the navel), of average duration (up to 1.5-2 hours), usually before meals or after 1.5-2 hours after meals, sometimes in the morning before breakfast. In the latter case, eating partially relieved the pain syndrome. The pain intensified after eating sour, spicy and fried foods (over the past 2 months the boy was on a diet with partial elimination of them). To relieve pain, I sometimes used antispasmodics and antacids (with a short-term effect).
Dyspeptic complaints: periodically there is belching, heartburn (according to the child, when overeating in the evening), a feeling of rapid satiety, a tendency to constipation.
The complex of “general” complaints is represented by severe asthenic syndrome.
From the anamnesis it is known that the boy has been ill for 3 years and has not been previously examined or treated. Among the factors that trigger an exacerbation, he names errors in diet and violation of the diet, as well as physical activity (practices martial arts). The frequency of exacerbations is 2-3 times a year, seasonality is not clearly visible, but in the summer the child’s well-being improves significantly.
Heredity is burdened by CGD (paternal grandfather) and DU (mother and maternal aunt).
Early history was unremarkable. I was not sick until I was 3 years old. Past diseases: ARVI (1-2 times a year), acute bronchitis, follicular tonsillitis, traumatic hemarthrosis of the right knee joint, rubella, chicken pox. There is no allergic history.
An objective examination showed that the child’s condition was satisfactory. The boy has a correct physique, satisfactory nutrition, and developed muscles of the upper shoulder girdle. The skin and visible mucous membranes are clean. The tongue is covered with a white coating, more at the root. Peripheral lymph nodes are not enlarged. Heart sounds are clear, rhythmic, 62 beats per minute; systolic murmur at the apex of the heart, moderate intensity. Blood pressure 100/b0 mm Hg. Art. Vesicular breathing. The abdomen is soft, accessible to superficial palpation in all parts. With deep palpation, pain is detected in the epigastric region, pyloroduodenal zone, right hypochondrium, Mayo-Robson point. Mendelian and cystic symptoms (Ortner, Kehr, Murphy) are positive. The liver and spleen are not enlarged in size, the sigma is not spasmodic. Stool, according to words, is daily, less often - every other day, formalized, without pathological signs. Urination is not impaired.
As a result of the survey, the following was revealed:
1) hemogram, biochemical blood test, general urine test - without any features;
2) coprogram - muscle fibers without striations (+), fatty acids (+), extracellular starch (++);
3) intragastric pH-metry
- the acid-forming function of the stomach is increased (pH range 1.2 - 1.4) while maintaining the compensatory capabilities of the antrum (pH 6.5-6.8), the rate of acid formation is increased;
4) Ultrasound - signs of biliary dyskinesia (BDSD), reactive state of the pancreatic parenchyma (echo-positive signals in the tail area with an increase in its size);
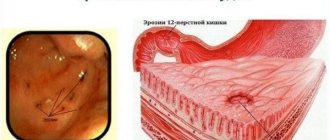
5) FEGDS - superficial fundal gastritis, erosive antral gastritis (8 “acute” erosions up to 0.3 cm in diameter), superficial bulbitis, cardia insufficiency;
6) help test (++);
7) Ultrasound of the heart - an accessory chord in the left ventricle was detected;
assessment of the initial autonomic tone - parasympathicotonia.
Based on the totality of the child’s complaints, clinical history, and laboratory and instrumental data, the following diagnoses were made:
Basic diagnosis: chronic gastroduodenitis (superficial fundal gastritis, erosive antrum gastritis, superficial bulbitis), ulcer-like variant, HP (+), with increased acid-forming function, exacerbation phase.
Concomitant diagnosis: biliary dyskinesia of the hypertensive type; reactive pancreatitis with moderate excretory pancreatic insufficiency; minor cardiac anomaly (accessory chord in the left ventricle).
Treatment.
1. Diet - table 1-in.
2. Semi-bed rest.
3. Drug therapy: anti-Helicobacter triple regimen:
- Kvamatel - 20 mg 2 times a day - 2 weeks, then 20 mg - in the evening - 1 week, before meals;
— de-nol — 2 tables. 2 times a day - 2 weeks, before meals;
— flemoxin-solutab — 1 tablet. (500 mg) 2 times a day for 7 days, before or after meals.
When switching to a single dose of quamatela - phosphalugel, 1 sachet 3 times a day - 2 weeks, before meals;
— mezim-forte (3500 IU), 1 table. 3 times a day - 2 weeks, before meals;
- galstena 10 drops. 3 times a day - 4 weeks, after meals.
A control FEGDS was performed on an outpatient basis 3 weeks after the first study. All erosions were epithelialized, the inflammatory background of the gastric mucosa decreased somewhat; help test (+/-).
During treatment, the child’s well-being improved significantly: spontaneous abdominal pain and dyspeptic symptoms disappeared, and palpation pain decreased.
School attendance and preventive vaccinations are allowed. An exemption from physical education lessons and training was given for 1 month with a gradual introduction to the usual training rhythm.
Anya P., 13 years old, contacted a local gastroenterologist with complaints of abdominal pain (around the navel), stabbing and aching, lasting up to 30-40 minutes, occurring 20-30 minutes after eating, not depending on the nature of the food eaten, passing on one's own. There is pronounced belching, a feeling of heaviness in the stomach, and rapid satiety. Periodically there is bloating and rumbling in the stomach. Appetite is reduced. Signs of asthenia are moderately expressed.
From the anamnesis it is known that the girl has been ill for 1.5 years. She contacted the local pediatrician twice: a diagnosis of diarrhea was made, and choleretic herbal medicine was prescribed without significant improvement. Exacerbations of the disease occur 2-3 times a year and are seasonal (spring - autumn). Heredity for gastrointestinal diseases is not burdened.
Early history was unremarkable. I was not sick until I was 1 year old. She grew and developed according to her age. Past diseases: ARVI (2-3 times a year), bronchopneumonia (at 5 years old), enterobiasis (at 6 years old), chicken pox, scarlet fever. There is no allergic history.
An objective examination showed that the child’s condition was satisfactory. The skin and visible mucous membranes are clean. The tongue is covered with a white coating. Peripheral lymph nodes are not enlarged. Heart sounds are clear, rhythmic, 70 beats per minute. BP 110/75 mm pr. Art. Vesicular breathing. The abdomen is soft, accessible to superficial palpation in all parts. With deep palpation, pain is detected in the epigastric region, pyloroduodenal zone, left and right hypochondrium. Mendelian and cystic symptoms (Ortner, Kehr, Murphy) are positive. The liver and spleen are not enlarged in size, the sigma is not spasmodic. The stool, according to words, is daily, formed, without pathological signs. Urination is not impaired.
As a result of the outpatient examination, the following was revealed: 1) hemogram, general urine test - without features, 2) coprogram - muscle fibers without striations (++), fatty acids (++), intracellular starch (++), scraping for enterobiasis ( -); 3) intragastric pH-metry - the acid-forming function of the stomach is preserved (pH range 1.7-1.8) while maintaining the compensatory capabilities of the antrum (pH 6.7-7.0), 4) Ultrasound - an increase in the sagittal size of the liver, signs of phlebotomy , 5) FGDS - superficial widespread gastritis, superficial bulbitis, cardia insufficiency, grade I reflux esophagitis, grade II GHD, b) helpiltest (-), 7) assessment of the initial autonomic tone - parasympathicotonia, examination by an ENT doctor - diagnosis: chronic tonsillitis (compensated).
Based on the totality of the child’s complaints, clinical history and laboratory and instrumental data, the following diagnoses were made:
The main diagnosis is: chronic gastroduodenitis (superficial pangastritis, superficial bulbitis, stage II GHD), gastritis-like variant, HP (-), with preserved acid-forming function, in the acute phase.
Concomitant diagnosis: reflux esophagitis degree I; biliary dyskinesia of the hypertensive type. Chronic tonsillitis (compensated).
Treatment.
1. Diet - table 1-in.
2. Semi-bed rest.
3. Drug therapy: Vikalin - 3 weeks, Motilium - 3 weeks, Chofitol - 3 weeks, then Mezim-Forte 2 weeks, Laminolact - 4 weeks, Complivit - 3 weeks.
Under the influence of the treatment, the girl’s well-being improved, the pain syndrome was relieved, pain on palpation disappeared, and dyspeptic symptoms decreased. School attendance and preventive vaccinations are allowed. Physical education classes in the preparatory group are allowed. Further observation by a district gastroenterologist and local pediatrician is indicated.
The examples given are taken from life and illustrate significant differences in key characteristics in two different children with the same, at first glance, diagnosis. As can be seen from the clinical examples, treatment tactics in each case were structured differently, in accordance with the individual picture of the disease. Deciphering all these features hidden under the abbreviation CGD is the task of the pediatrician and allows one to avoid erroneous judgments about the homogeneity of this disease.
By composition
Antibacterial drugs are divided into 6 groups:
- Penicillins are the first antimicrobial drugs, obtained back in 1928 from a biological substance (Penicillium fungi). For a long time they remained the most popular medicine for the treatment of infectious diseases.
- Cephalosporins belong to the group of the most powerful antimicrobial agents with a wide range of applications. They completely destroy pathogenic flora and are well tolerated by humans.
- Macrolides are the name of a group of narrow-range antimicrobial agents. They do not destroy the diseased cell, but only stop its growth. This category includes the following drugs: erythromycin, spiramycin, azithromycin.
- Tetracyclines are good drugs for the treatment of infectious diseases of the respiratory and urinary tract.
- Fluoroquinolones are antimicrobial agents with a wide range of effects. Completely destroy pathogenic microorganisms. You can find 1st-2nd generation medications on sale. Doctors usually prescribe them to combat Pseudomonas aeruginosa.
- Aminoglycosides are antimicrobial drugs with a wide range of applications. Popular drugs in this group - streptomycin (therapy of tuberculosis, plague) and gentamicin - are used as ointments, eye drops, and injections for ophthalmic infections.
Generations of drugs. Advanced antimicrobial drugs already have six generations. For example, penicillin was the first drug of natural origin, while the third or sixth generation is an already improved version, which includes the strongest inhibitors. The relationship is direct: the newer the generation, the more effective the effect of drugs on pathogenic microflora.
By method of administration. Oral – taken by mouth. These are various syrups, tablets, soluble capsules, suspensions. Parenteral - administered intravenously or intramuscularly. They work faster than oral medications. Rectal medications are injected into the rectum.
Important! Taking antibiotics is allowed only after consulting a doctor, otherwise antibiotic resistance will develop.
New generation antibacterial agents
The difference between the latest generations of antibiotics and their earlier versions is a more advanced formula of the active substance. Active components specifically eliminate only pathological reactions in the cell. For example, new generation intestinal antibiotics do not disrupt the microflora of the gastrointestinal tract. At the same time, they fight an entire “army” of infectious agents.
The newest antibacterial drugs are divided into five groups:
- Tetracycline – tetracycline.
- Aminoglycosides – streptomycin.
- Penicillin series - amoxicillin and others.
- Amphenicols – chloramphenicol.
- Carbapenem group – meropenem, imipenem, invaz.
Let's consider several well-known antimicrobial agents of imported and Russian production.
Amoxicillin is an imported antimicrobial drug from the penicillin group. Used in medical practice to treat bacterial infections. Effective for intestinal infections, sinusitis, sore throat, Lyme disease, dysentery, sepsis.
Avelox is the latest generation of medications from the group of fluoroquinolones. It has a strong effect on bacterial and atypical pathogens. Does not harm the kidneys and gastrointestinal tract. Used for acute and chronic diseases.
Cephalosporins are third generation antibiotics. This group includes Ceftibuten, Ceftriaxone and others. Used to treat pyelonephritis and pneumonia. In general, these are safe products with few side effects. However, they should be taken only after consulting a doctor. There are many medications, but a specialist will recommend which one to choose.
Doriprex is an imported antimicrobial drug of synthetic origin. Showed good results in the treatment of pneumonia, advanced intra-abdominal infections, pyelonephritis.
Invaz is an antibacterial agent from the carbapenem group. Available in ampoules for parenteral administration. Shows a rapid effect in the treatment of bacterial disorders of the skin, soft tissues, urinary tract infections, pneumonia, septicemia.
Augmetin is a third generation semi-synthetic penicillin with the addition of enhancing inhibitors. Pediatricians recognize it as the best comprehensive medication for the treatment of childhood sinusitis, bronchitis, tonsillitis and other respiratory tract infections.
Cefamandole is a Russian-made antibacterial agent. Belongs to the group of third generation cephalosporins. Used to treat intestinal infections, pathogens of genital infections. As an antimicrobial agent with a wide range of effects, it is used for colds.
Additional methods and means of treating gastritis
When treating gastritis, it often becomes necessary to involve specialists from other fields of medicine. This is due to the fact that diseases of the gastrointestinal tract rarely go away without leaving a trace for the body as a whole, which requires treatment of complications. In addition, the disease can be triggered by factors unrelated to the gastrointestinal tract. Thus, erosive gastritis in the acute stage is often accompanied by gastric bleeding, leading to anemia, which makes it necessary to involve a hematologist in the treatment. And the cause of damage to the gastric mucosa can be allergic reactions or endocrine disorders - the area of influence of an immunologist-allergist and endocrinologist.
The best broad-spectrum antibacterial drugs
New generation antimicrobial agents are usually synthesized from natural raw materials and stabilized in laboratories. This helps enhance the effect of the drug on pathogenic microflora.
What drugs are the most powerful? Doctors classify these as broad-spectrum antibacterial agents. Below is a short list of drugs by name:
- AMOXICLAV - belongs to the group of aminopenicillins. It has a mild effect and is used to treat infectious diseases. The drug can be used with caution and only after consultation with a doctor during pregnancy, as well as during breastfeeding. Available in tablets or in bulk form for oral administration, as well as in powders for injection.
- SUMAMED is a popular antimicrobial drug for the treatment of infections of the gastrointestinal tract, genitourinary system, respiratory tract diseases - sore throat, bronchitis, pneumonia. It affects the liver and kidneys, so it is not prescribed for patients with hypersensitivity to macrolides.
- CEFOPERAZONE – belongs to the group of cephalosporins. Prescribed by doctors for the treatment of urinary tract infections, prostatitis, skin disorders, and respiratory diseases. A good drug for recovery after gynecological, orthopedic and abdominal surgeries. Available in a form for parenteral administration - injection.
- UNIDOX SOLUTAB is the latest generation tetracycline. Used for extensive treatment of gastrointestinal infections, colds, prostatitis. It acts gently, without causing dysbacteriosis.
- LINCOMYCIN is a drug prescribed for the treatment of osteomyelitis, sepsis, and staphylococcal infections. It has a strong effect on pathogenic cells, therefore it has a long series of side effects. Among them are hypotension, weakness, dizziness. Do not use during pregnancy, or in patients with hepatic-renal insufficiency.
- RULID is a fourth generation macrolide. The main substance is roxithromycin. Prescribed for urogenital infections, diseases of the gastrointestinal tract and upper respiratory tract. Available in tablets.
- CEFIXIM – by name, it is a drug from the group of cephalosporins. Has a bactericidal effect on pathogenic cells. Helps with gastrointestinal infections, prostatitis, and also treats colds. It is quite toxic, so it should not be taken if you have kidney or liver problems.
- Cefotaxime is the last group of cephalosporins. The drug is indicated for the treatment of gynecological, urological, and colds. It copes well with inflammatory processes and suppresses pathogenic microflora.
Gastritis with low acidity
Due to the significant disruption of the functional activity of the stomach in gastritis with low acidity, the leading one is dyspeptic syndrome. Patients complain of a feeling of heaviness and fullness in the epigastrium, bad breath, belching rotten and large amounts of air. Appetite is significantly reduced, up to complete refusal to eat. Nausea, increased salivation, and a feeling of bitterness in the mouth are bothersome.
Pain syndrome with gastritis with low acidity may be absent. Pain in hypoacid gastritis is not associated with spasm of the muscle layer, but with stretching of the stomach. Most often, patients complain of dull, aching pain that intensifies after eating. The severity of the pain syndrome is directly dependent on the quantity and quality of food - eating hot, spicy foods leads to increased pain. Dyskinetic syndrome with gastritis with low acidity leads to frequent changes in constipation and diarrhea, increased gas formation, and dumping syndrome.
Atrophy of the mucous membrane in gastritis with low acidity entails impaired absorption of vitamins and nutrients, the formation of polyhypovitaminosis and protein-energy deficiency, B12- and folate-deficiency anemia. Weight decreases progressively; Arterial hypotension, increased fatigue and depression, dry skin, and vascular bleeding are noted.
With a long course of the disease, achylia develops - a complete cessation of hydrochloric acid production. In addition to dyspeptic symptoms, it manifests itself as glossitis and gingivitis. The tongue is bright red, varnished; Gums are inflamed and loose. Achilles diarrhea is associated with a significant decrease in the functional activity of the gastric glands and pancreas, due to which the processes of putrefaction and fermentation are activated in the intestines.
Gastritis with low acidity is classified into clinical forms: chronic rigid, hypertrophic and polypous gastritis. Rigid gastritis is characterized by damage to the antrum of the stomach. This variant of hypoacid gastritis is characterized by increased smooth muscle tone, spasms, sclerosis and rigidity of the gastric wall. Ultimately, the antrum becomes deformed and takes on the appearance of a narrow, dense tube. The clinic is dominated by pain, uncorrectable dyspepsia, and achlorhydria.
A study of biopsy specimens for hypertrophic gastritis reveals atrophy of the main gastric glands, proliferation of the integumentary epithelium, muscle layer and connective tissue. The polypous variant is most often the outcome of any gastritis with low acidity. An endoscopic examination reveals epithelial growths in the lumen of the stomach; the only clinical manifestations are recurrent bleeding. Gastric polyps very often become malignant, so the prognosis for polypous growths is serious.
Complications of gastritis with low acidity include: ulceration of the mucous membrane in antral gastritis, malignancy in 30% of patients with gastric polyposis and in 10-40% of patients with other types of atrophic gastritis. Atrophy of the gastric epithelium provokes inflammatory changes in the distal parts of the digestive tract, intestinal dysbiosis, pancreatitis, cholecystitis. Impaired absorption of vitamins and nutrients leads to anemia, polyhypovitaminosis, and food allergies. Prolonged course of gastritis with low acidity, especially without proper treatment, can lead to persistent neuropsychiatric disorders.
Summary
We reviewed Russian and imported broad-spectrum antibiotics and briefly described the classification of drugs. Let's answer the question: which antibacterial agents to choose?
It is important to understand that antimicrobial drugs for extensive use are toxic and therefore negatively affect the microflora. In addition, bacteria mutate, which means the drugs lose their effectiveness. Therefore, antibacterial agents with the latest structure will be a priority over their earlier counterparts.
Self-medication with antibiotics is dangerous to health. In case of an infectious disease, the first step is to consult a doctor. The specialist will determine the cause of the disease and prescribe effective antibacterial agents. Self-medication “at random” leads to the development of antibiotic resistance.