Appendectomy is one of the most common interventions on the abdominal organs. It involves removing the inflamed appendix, so appendicitis is the main indication for surgery. Inflammation of the appendix occurs in young people (mostly 20-40 years old) and in children.
Appendicitis is an acute surgical disease manifested by abdominal pain, symptoms of intoxication, fever, and vomiting. Despite the apparent simplicity of the diagnosis, sometimes it is quite difficult to confirm or refute the presence of this disease. Appendicitis is a “master of disguise”; it can simulate many other diseases and have a completely atypical course.
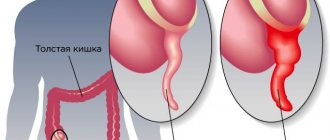
The vermiform appendix extends in the form of a narrow canal from the cecum. In early childhood, it participates in local immunity thanks to the lymphoid tissue in its wall, but with age this function is lost, and the process is a practically useless formation, the removal of which does not carry any consequences.
The cause of inflammation of the appendix has not yet been precisely determined; there are a lot of theories and hypotheses (infections, obstruction of the lumen, impaired trophism, etc.), but with its development there is always only one way out - surgery.
Based on the nature of changes in the appendix, destructive (phlegmonous, gangrenous) and non-destructive (catarrhal, superficial) forms of the disease are distinguished.
Acute purulent appendicitis, when pus accumulates in the wall of the appendix and its lumen, as well as the gangrenous variant, a sign of which is necrosis (gangrene) of the appendix, are considered the most dangerous, since peritonitis and other dangerous complications are likely. A special place belongs to chronic appendicitis, which occurs as a result of catarrhal disease that has not been operated on. This type of inflammation is accompanied by periodic exacerbations with pain, and an adhesive process develops in the abdominal cavity.
Appendiceal infiltrate is an inflammatory process in which the appendix merges with the surrounding areas of the intestine, peritoneum, and omentum. The infiltration is limited in nature and, as a rule, requires preliminary conservative treatment.
A special group of patients consists of children and pregnant women. In children, the disease practically does not occur until one year of age. The greatest diagnostic difficulties arise in young patients under 5-6 years of age, who have difficulty describing their complaints, and specific signs are less pronounced than in adults.
Pregnant women are more susceptible to inflammation of the appendix than others for a number of reasons: a tendency to constipation, displacement of abdominal organs by an enlarging uterus, decreased immunity due to changes in hormonal levels. Pregnant women are more prone to destructive forms that can lead to fetal death.
Indications and preparation for surgery
Appendectomy is one of the interventions that in most cases is performed as an emergency. Indication: acute appendicitis. A planned operation to remove the appendix is performed with appendiceal infiltrate after the inflammatory process has subsided, approximately 2-3 months from the onset of the disease. In case of increasing symptoms of intoxication, rupture of an abscess with peritonitis, the patient needs emergency surgical treatment.
There are no contraindications to appendectomy, except in cases of the patient's agonal state, when the operation is no longer advisable. If doctors have adopted a wait-and-see approach due to appendiceal infiltration, then severe decompensated diseases of the internal organs may be contraindications to surgery, but during conservative treatment the patient’s condition can be stabilized to such an extent that he can undergo the intervention.
The operation usually lasts about an hour, both general anesthesia and local anesthesia are possible. The choice of pain relief is determined by the patient’s condition, his age, and concomitant pathology. Thus, in children, people with excess body weight, which involves greater trauma when entering the abdominal cavity, with nervous overexcitation and mental illness, general anesthesia is preferable, and in thin young people, in some cases, it is possible to remove the appendix with local anesthesia. Pregnant women, due to the negative impact of general anesthesia on the fetus, are also operated on under local anesthesia.
The urgency of the intervention does not require sufficient time to prepare the patient, so the necessary minimum examinations are usually performed (general blood test, urine test, coagulogram, consultations with specialists, ultrasound, x-rays). To exclude acute pathology of the uterine appendages, women need to be examined by a gynecologist, possibly with an ultrasound examination. If there is a high risk of thrombosis of the veins of the extremities, the latter are bandaged before surgery with elastic bandages.
Before the operation, the bladder is catheterized, the contents are removed from the stomach if the patient ate later than 6 hours before the operation, and an enema is indicated for constipation. The preparatory stage should last no more than two hours.
When the diagnosis is beyond doubt, the patient is taken to the operating room, anesthesia is administered, and the surgical field is prepared (hair shaving, iodine treatment).
Classification of fever
To determine what exactly caused the system dysfunction, fever is classified:
- temperature 37 – 38 degrees – subfebrile;
- from 38 to 39 – febrile;
- from 39 to 40 – pyretic;
- from 40 and above – hyperpyretic.
To determine the graph of temperature fluctuations after removal of appendicitis, on the first day, drugs with antipyretic effects are not prescribed.
According to the type of fluctuations, hyperthermia is:
- constant (balancing within 1 degree);
- laxative (values are not stable, fluctuate by 1 – 2 degrees);
- intermittent – varies between low temperatures of 38 – 39 degrees;
- return – high numbers after a couple of days, decrease to normal limits;
- hectic - fever occurs with sudden temperature changes of 3 - 5 degrees;
- wavy - there is a smooth increase, decreasing to subfebrile values, with a smooth transition to normal limits;
- atypical – causeless increase;
- perverted - when the temperature rises in the morning, and in the evening there are no deviations from the norm;
- wavy in an acute form - short jerks without breaks between lifts;
- recurrent – after remissions, the fever returns.
Progress of the operation
The classic operation to remove appendicitis is performed through an incision in the anterior abdominal wall in the right iliac region, through which the cecum with the appendix is removed, it is cut off, and the wound is sutured tightly. Depending on the location of the appendix, its length, and the nature of pathological changes, antegrade and retrograde appendectomy are distinguished.
The course of the operation includes several stages:
- Formation of access to the affected area;
- Removal of the cecum;
- Severing the appendix;
- Layer-by-layer suturing of the wound and control of hemostasis.
To “get” to the inflamed appendix, a standard incision about 7 cm long is made in the right iliac region. The reference point is McBurney's point. If you mentally draw a segment from the navel to the right upper iliac spine and divide it into three parts, then this point will lie between the outer and middle thirds. The cut passes at right angles to the resulting line through the indicated point, a third of it is located above, two thirds - below the specified landmark.
on the left – traditional open surgery, on the right – laparoscopic surgery
After the surgeon has cut through the skin and subcutaneous fat, he will have to penetrate the abdominal cavity. The fascia and aponeurosis of the oblique muscle are cut, and the muscles themselves are moved to the sides without incision. The last obstacle is the peritoneum, which is cut between the clamps, but first the doctor will make sure that the intestinal wall does not get into them.
Having opened the abdominal cavity, the surgeon determines the presence of obstacles in the form of adhesions and adhesions. When they are loose, they are simply separated with a finger, and when they are dense, connective tissue, they are cut with a scalpel or scissors. This is followed by the removal of a section of the cecum with the appendix, for which the surgeon carefully pulls the wall of the organ, removing it out. Upon penetration into the abdomen, inflammatory exudate may be detected there, which is removed with wipes or an electric suction.
appendectomy: progress of the operation
The appendix is removed antegrade (typically) and retrogradely (less commonly). Antegrade removal involves ligation of the mesenteric vessels, then a clamp is applied to the base of the appendix, the appendix is sutured and cut off. The stump is immersed in the cecum, and the surgeon remains to apply stitches. The condition for antegrade removal of the appendix is the possibility of its unhindered removal into the wound.
Retrograde appendectomy is performed in a different sequence: first, the appendix is cut off, the stump of which is immersed in the intestine, sutures are applied, and then the vessels of the mesentery are gradually sutured and it is cut off. The need for such an operation arises when the appendix is localized behind the cecum or retroperitoneally, with a pronounced adhesive process that makes it difficult to remove the appendix into the surgical field.
After the appendix is removed, stitches are applied, the abdominal cavity is examined, and the abdominal wall is sutured layer-by-layer. Usually the suture is blind and does not imply drainage, but only in cases where there are no signs of the inflammatory process spreading to the peritoneum, and no exudate is found in the abdomen.
In some cases, it becomes necessary to install drains, indications for which are:
- Development of peritonitis;
- Possibility of incomplete removal of the appendix and insufficient hemostasis;
- Inflammation of the retroperitoneal tissue and the presence of abscesses in the abdominal cavity.
When it comes to peritonitis, 2 drainages are needed - into the area of the removed process and the right lateral canal of the abdomen. In the postoperative period, the doctor carefully monitors the discharge from the abdominal cavity, and if necessary, a repeat operation is possible.
Peritonitis (inflammation of the peritoneum) can be suspected even at the stage of examining the patient. In this case, an incision in the midline of the abdomen would be preferable, providing a good view of the abdominal cavity and the possibility of lavage (washing with saline or antiseptics).
Duration of hyperthermia
The duration of temperature after surgery for appendicitis is above normal limits and should not exceed a decade, but if all signs indicate that the body is not recovering, it is worth focusing the doctor’s attention on this, since there is a more serious danger of developing postoperative pathology.
Reasons why the temperature does not stabilize after appendicitis removal a week later:
- large blood losses during removal of appendicitis;
- injuries to nearby organs;
- infection during surgery;
- against a background of suppressed immunity, acquisition of respiratory diseases;
- inflammation in the postoperative wound;
- if after surgery a drainage is placed in the wound;
- non-compliance with the recommended diet - adherence to the correct diet speeds up the healing process.
It is worth noting that if the drainage is in the wound for a long time, the temperature can persist for more than 10 days.
More serious causes are usually accompanied by additional symptoms:
- bowel dysfunction – mainly constipation;
- abdominal cramp;
- bouts of vomiting;
- excessive sweating;
- loss of consciousness.
Complications that maintain high temperature in the body can be caused by the negligence of medical personnel and insufficient competence of doctors. Before you decide to take a responsible step, you should familiarize yourself with the reputation of the clinic and doctor. Lack of sterility, improper dressing, earlier removal of sutures, drainage forgotten in the wound - reasons that can not only increase the readings on the thermometer, but also lead to more serious consequences.
Laparoscopic appendectomy
Recently, with the development of technical capabilities in medicine, minimally invasive techniques, also used in the surgery of abdominal diseases, are becoming increasingly popular. Laparoscopic appendectomy is a worthy alternative to classical surgery, but for a number of reasons it cannot be performed on every patient.
Laparoscopic removal of the appendix is considered a more gentle method of treatment, which has a number of advantages:
- Low morbidity compared to abdominal surgery;
- Possibility of local anesthesia in most patients;
- Shorter recovery period;
- The best result for severe diseases of internal organs, diabetes, obesity, etc.;
- Good cosmetic effect;
- Minimum complications.
However, laparoscopic appendectomy also has some disadvantages. For example, an operation requires the availability of appropriate expensive equipment and a trained surgeon at any time of the day, because the patient can be taken to the hospital at night. Laparoscopy does not allow a detailed examination of the entire volume of the abdominal cavity, adequate sanitation and removal of exudate in common forms of the inflammatory process. In severe cases, with peritonitis, it is impractical and even dangerous.
Through many years of discussions, doctors determined the indications and contraindications for laparoscopic removal of the appendix.
The following are considered indications:
- Doubts about the diagnosis requiring laparoscopy for diagnostic purposes. For example, in a woman with pain in the right iliac fossa, after several hours of observation, the diagnosis of appendicitis cannot be confirmed. The surgeon goes for laparoscopy and discovers inflammation of the uterine appendages, which can spread to the appendix, or it is already inflamed, in which case it is quite logical to remove it laparoscopically. The child may be diagnosed with catarrhal appendicitis, and the appendix is removed during laparoscopy. These operations are performed in the absence of contraindications (purulent process, peritonitis), in which, after laparoscopy, open abdominal surgery is performed.
- Severe concomitant pathology (severe obesity, diabetes mellitus, heart failure), in which major surgical trauma is undesirable, the risk of infectious complications is high, and abdominal surgery is inevitably accompanied by large incisions (in obese patients).
- The patient’s desire to perform the operation laparoscopically (of course, if this does not conflict with safety).
- Laparoscopic surgery for gynecological pathology, when in case of adhesions, purulent inflammation of the pelvic organs, leaving even an unchanged appendix is impractical and is fraught with secondary appendicitis.
If there are no risks, the patient’s condition is stable, and the inflammation has not spread beyond the appendix, then laparoscopic appendectomy can be considered the method of choice.
Contraindications to minimally invasive treatment:
- More than a day from the onset of the disease, when the likelihood of complications is high (perforation of the appendix, abscess).
- Peritonitis and the transition of inflammation to the cecum.
- Contraindications for a number of other diseases - myocardial infarction, decompensated heart failure, bronchopulmonary pathology, etc.
In order for laparoscopic appendectomy to be a safe and effective treatment procedure, the surgeon will always weigh the pros and cons, and in the absence of contraindications to the procedure, it will be a low-traumatic treatment method with minimal risk of complications and a short postoperative period.
The course of laparoscopic appendectomy includes:
A small incision is made in the umbilical area through which carbon dioxide is injected into the abdomen for a good view. The laparoscope is also inserted through the same hole. The surgeon examines the abdomen from the inside, and if doubts arise about the safety of further manipulations, he proceeds to open surgery.- Instruments are inserted through incisions in the pubic area and right hypochondrium, with the help of which the appendix is captured, the vessels are ligated, the mesentery is cut off, then the appendix is cut and removed from the abdomen.
- Inspection and sanitation of the abdominal cavity, drainage if necessary, suturing the instrument insertion sites.
Laparoscopic surgery for appendicitis lasts up to one and a half hours, and the postoperative period takes only 3-4 days. Scars after such an intervention are barely noticeable, and after some time has passed for final healing, they can be difficult to find.
The suture after open surgery is removed after 7-10 days. A scar will remain at the site of the incision, which will thicken and fade over time. The scar formation process takes several weeks.
The cosmetic effect is largely determined by the efforts and skill of the surgeon. If the doctor treats the wound suturing conscientiously, the scar will be almost invisible. If complications develop, if it is necessary to increase the length of the incision, the surgeon will be forced to sacrifice the cosmetic side of the issue in favor of preserving the health and life of the patient.
Diagnosis
When diagnosing the causes of hyperthermia after removal of the appendix, a blood test is prescribed to determine the presence of an inflammatory process. In this case, the number of leukocytes matters. But a blood test is not the only diagnostic method.
Methods used
Medical professionals often use:
- Diagnosis using an ultrasound machine. The procedure allows you to surgically examine the abdominal cavity without additional penetration and examine whether there is any damage to the internal organs. In the absence of damage, the site of the former attachment of the process of the cecum is examined. The area is examined for the presence of an inflammatory process.
Appendix on ultrasound
- The postoperative suture is examined. Sometimes there may be inflammation at the edges of the suture, which can cause prolonged fever.
- It is possible to biopsy the material through an open wound after removal of the appendix.
- Taking urine for analysis. The analysis provides information on the presence of leukocytes and possible problems with the genitourinary system.
Interpretation of analyzes
The indicated diagnostic methods are sufficient to establish the exact cause of prolonged hyperthermia; additional studies are required in rare cases.
It should be understood that the values in the analyzes for men, women and children have different ranges and different variants of the norm.
Women, due to the way their bodies work, have a wider range of leukocytes than men. This is associated with a specific day of the menstrual cycle. In this regard, after 21 years of age, test results are divided based on gender.
When testing blood in children, the level of leukocytes is higher than normal not only in pathological conditions such as acute appendicitis, but also in other cases. The immune system of a child, in comparison with an adult’s body, is not as perfect. At the same time, infections and pathogenic environments more often enter the child’s body, which requires the immune system to increase the level of leukocytes.
Leukocytes in human blood
This is necessary to protect the body. If a child has appendicitis, the doctor must take blood for analysis not only before the operation, but also after it. The procedure is necessary to monitor your well-being and the proper healing process.
Postoperative period
In cases of uncomplicated forms of appendicitis and a favorable course of the operation, the patient can be immediately taken to the surgical department, in other cases - to the postoperative ward or intensive care unit.
During the rehabilitation period, wound care and early activation of the patient are of great importance, allowing the intestines to “turn on” in time and avoid complications. Dressings are carried out every other day, if there are drainages - daily.
On the first day after the intervention, the patient may experience pain and increased body temperature. Pain is a natural phenomenon, because both the inflammation itself and the need for incisions imply tissue damage. Usually the pain is localized to the site of the surgical wound, it is quite tolerable, and the patient is prescribed analgesics if necessary.
Antibacterial therapy is indicated for complicated forms of appendicitis. Fever may be a consequence of surgery and a natural reaction during the recovery period, but it must be carefully monitored, since an increase in temperature to significant levels is a sign of serious complications. The temperature should not exceed 37.5 degrees during the normal course of the postoperative period.
Many patients prefer to lie in bed, citing weakness and pain. This is wrong, because the sooner the patient gets up and starts moving, the faster intestinal function will be restored and the lower the risk of dangerous complications, in particular thrombosis. In the very first days after the operation, you need to gather your courage and at least walk around the ward.
A very important role in interventions on the abdominal organs is given to diet and nutrition. On the one hand, the patient must get the calories he needs, on the other hand, he must not harm the intestines with an abundance of food, which during this period can cause adverse consequences.
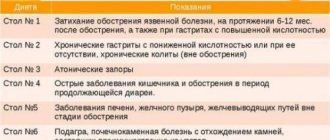
You can start eating after the appearance of intestinal peristalsis, as evidenced by the first independent stool. The patient should be informed what can be eaten after surgery and what is better to avoid.
Patients who have suffered acute appendicitis are assigned to table No. 5. It is safe to consume compotes and tea, lean meats, light soups and cereals, and white bread. Fermented milk products, stewed vegetables, and fruits that do not contribute to gas formation are useful.
During the recovery period, you should not eat fatty meats and fish, legumes, fried and smoked foods; you should exclude spices, alcohol, coffee, baked goods and sweets, and carbonated drinks.
On average, after surgery, the patient remains in the hospital for about a week in uncomplicated forms of the disease, otherwise longer. After laparoscopic appendectomy, discharge is possible already on the third day after the operation. You can return to work after a month with open operations, with laparoscopy - after 10-14 days. A sick leave certificate is issued depending on the treatment performed and the presence or absence of complications for a month or more.
High fever after appendicitis surgery
It is difficult to predict how a patient will react to organ removal and how long the temperature will last after surgery, since each patient is individual and the duration of the rehabilitation process is influenced by many different factors. First of all, it is necessary to understand that hyperthermia itself, after the intervention of a surgeon, is a normal and quite expected phenomenon. The indicators are influenced by the choice of method in which the operation was performed:
- Laparoscopic - the organ is removed through an incision in the abdomen. Since the tissue is minimally damaged, the healing process will not take much time. An increase in temperature after laparoscopy can last up to 3 days and disappear spontaneously. There is no need for long-term hospitalization and recovery time is short.
- Abdominal surgery is prescribed in difficult cases, with accumulation of pus in the organ, enlargement, or looseness of the structure. After opening the incision, stitches are placed and the requirements for rehabilitation become significantly more complicated. In such cases, hyperthermia can be either low-grade or high - varying between 37 - 38 degrees. It is worth noting that it can last for a decade.
Complications
After surgery to remove the appendix, some complications may develop, so the patient needs constant monitoring. The operation itself usually proceeds well, but some technical difficulties may be caused by the unusual location of the appendix in the abdominal cavity.
The most common complication in the postoperative period is suppuration in the incision area, which can be diagnosed in every fifth patient with purulent types of appendicitis. Other options for unfavorable developments are peritonitis, bleeding into the abdominal cavity due to insufficient hemostasis or sutures slipping off the vessels, suture dehiscence, thromboembolism, adhesive disease in the late postoperative period.
Sepsis is considered a very dangerous consequence, when purulent inflammation becomes systemic, as well as the formation of ulcers (abscesses) in the abdomen. These conditions are facilitated by rupture of the appendix with the development of diffuse peritonitis.
Causes of fever
Fever is a complication that occurs after surgery in the body. Under its influence, the body's barrier functions increase the production of interferon and interleukins. The task of proteins is to ensure the phagocytic function of leukocytes.
The temperature after appendectomy stimulates the production of proteins that reduce the vital processes of bacteria and builds a connection between the immune and other systems. High temperatures enhance the functionality of anti-inflammatory proteins.
The main reason why the temperature persists after removal of appendicitis is related to the operation, but it can also be a consequence of damage to organs and systems. Fever often occurs due to complications:
- abscess formation of the wound surface;
- phlegmon in the peritoneal wall;
- accumulation of infiltrate or abscesses in the peritoneum;
- peritonitis.
In more than 80% of cases, a negative factor causing hyperthermia is a wound infection.
How to treat postoperative inflammation
A high temperature after appendicitis associated with a complication puts especially strain on the functioning of the kidneys and liver. If the organs had pathological changes before the operation, then the additional load can cause an exacerbation.
In some cases, a general blood test indicates the development of a purulent process. It is important to correct the situation in a timely manner. Fever after purulent appendicitis consistently leads to repeat surgery. Excess inclusions are removed, local antibiotic therapy is carried out, and drainage is installed.