The main causes of spasms
The main reasons why doctors may recommend taking anti-spasm medications are:
- diseases of the esophagus, stomach, gall bladder, intestines;
- pathologies of the ureters, bladder;
- spasms of smooth muscles of the bronchi.
Spasms can also be caused by neurological diseases, including due to a deficiency of certain vitamins and minerals (for example, magnesium). It can occur as a side effect while taking certain medications or after stopping them.
Antispasmodics: from clinical pharmacology to pharmacotherapy
Drugs belonging to the group of antispasmodics are among the most popular and prescribed by doctors of various specialties. Dysfunction of smooth muscle cells of internal organs underlies both chronic and acute pain syndromes in various diseases of the digestive system and urinary system of the pelvic organs [1, 2]. The most common cause of pain in pathologies of internal organs that have a layer of smooth muscle cells is their excessive contraction. Symptoms of spastic dysfunction of the digestive organs occur in 30% of cases in the absence of organic damage to the stomach or intestines, which leads to the frequent independent (without medical prescription) use of antispasmodic drugs. The widespread use of drugs in this group dictates the need to constantly remind about their clinical pharmacology, especially properties and tolerability, in order to avoid both underestimation and overestimation of therapeutic capabilities.
It is important that, by eliminating or preventing spasms of smooth muscles, antispasmodics, although they have a pronounced analgesic effect, normalizing the functioning of the organ, do not interfere with the mechanisms of pain. Unlike non-narcotic and opioid analgesics, they do not pose a significant threat of “erasing” symptoms in severe organic damage (masking the picture and making it difficult to verify the diagnosis).
Antispasmodics are most often used for:
- symptomatic treatment if spasm is a characteristic accompanying symptom of the disease, but does not play a role in pathogenesis;
- etiotropic therapy if spasm underlies the pathological condition;
- premedication when preparing patients for various procedures.
The process of contraction of a muscle cell is determined by the concentration of calcium ions in its cytoplasm, entering from the extracellular space through calcium (slow) channels of cell membranes. Another source of calcium is intracellular depots, which are more present in the smooth muscles of the colon and much less in the small intestine, including the duodenum. The release of this fraction of calcium ions leads to a phase contraction of the muscle cell [3]. One of the most common mediators influencing the process of muscle contraction is acetylcholine. When it interacts with muscarinic cholinergic receptors (M-cholinergic receptors), sodium channels open, sodium ions enter the cell and, as a result, membrane depolarization occurs. Depolarization, in turn, leads to the opening of calcium channels and the entry of calcium into the cell, increasing its intracellular concentration and muscle contraction. Activation of M-cholinergic receptors by acetylcholine leads to an increase in tone and contraction of smooth muscle cells, and blockade leads to a decrease in tone and relaxation of smooth muscle cells, which underlies the prescription of M-cholinergic blockers as antispasmodics [4, 5].
Calcium interacts with calmodulin, activates myosin light chain kinase, which cleaves the phosphorus residue from the ATP molecule bound to myosin, which leads to the interaction of actin and myosin and cell contraction. The most important role in muscle functioning is known to be played by the system of cyclic nucleotides [6]. Cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP) inhibit the release of intracellular calcium and the entry of calcium ions into the cell (cAMP), weaken the interaction of calcium ions with calmodulin. The levels of cAMP and cGMP are controlled by phosphodiesterase (PDE), which breaks down these nucleotides. Thus, the higher the PDE activity, the lower the concentration of cAMP and cGMP, the higher the concentration of calcium ions in the cytoplasm and the tone of the muscle cell and, conversely, the lower the PDE activity, the higher the concentration of cAMP and cGMP, the lower the concentration of calcium ions in the cytoplasm and muscle cell tone. The physiological role of PDE is diverse. 11 isoforms of this enzyme have been identified [4]. The main types of PDEs that affect the tone of smooth muscle cells are presented in
.
The mechanisms described above for regulating the calcium concentration inside the muscle cell, which are disrupted under pathological conditions and lead to spasm of the smooth muscle cells of the internal organs, imply the presence of several targets for pharmacological action [7]:
- blockade of neurotropic effects, that is, blocking the effect of acetylcholine on the M-cholinergic receptor (atropine, hyoscine butyl bromide);
- inhibition of PDE IV activity (drotaverine (No-spa));
- blockade of calcium ion entry (calcium channel blockers);
- blockade of calcium release from intracellular stores (mebeverine).
M-anticholinergics
This is one of the oldest groups of drugs used in medicine to affect the upper gastrointestinal tract. They are 5–10 times more effective in affecting the motility of the stomach than the large intestine, which is associated with the unequal density of M-cholinergic receptors in different parts of the gastrointestinal tract [8]. The largest number of receptors is in the stomach, much less in the intestines. The classic anticholinergic atropine has lost its value due to a large number of side effects. An attempt to increase the safety of therapy with M-anticholinergics was the creation of hyoscine butyl bromide, which is a relatively selective M-anticholinergic blocker acting on the M1 and M3 receptor subtypes, localized primarily in the walls of the upper gastrointestinal tract, gall bladder and biliary ducts. Unlike atropine, the drug does not penetrate the blood-brain barrier and has low (8–10%) systemic bioavailability, which leaves its mark on the variability in the manifestations of the effect.
Hyoscine butyl bromide accumulates in the smooth muscles of the gastrointestinal tract and is excreted unchanged from the body by the kidneys. It acts mainly on the stomach, duodenum, and gall bladder. The antispasmodic effect on the small and large intestines is realized in doses 2–10 times higher than therapeutic ones, therefore, for spasms of these parts of the intestine, use is not advisable (it is better to use myotropic antispasmodics, for example, drotaverine (No-shpa)) [9].
Anticholinergics are successfully used for abdominal pain caused by spasm in the upper gastrointestinal tract: sphincter of Oddi dysfunction, biliary dyskinesia, pylorospasm. Despite the fact that hyoscine butylbromide does not penetrate the central nervous system, it can cause side effects typical of M-anticholinergics (4% more often than placebo). This makes it, like other drugs in the group, contraindicated for glaucoma, benign prostatic hyperplasia, organic stenosis of the gastrointestinal tract, and tachyarrhythmias [10]. Since the drug is sold without a prescription and may cause unwanted effects in patients suffering from these diseases, it is important to inform them in advance. Unfortunately, the importance of selectivity of drug action is often unreasonably exaggerated. Thus, the statement that hyoscine butylbromide acts only at the site of spasm seems controversial, since M-cholinergic receptors are not located locally.
From the point of view of the breadth of effects on organs and systems of hyoscine, butyl bromide is no less effective than myotropic drugs (drotaverine (No-shpa)), but its action, unlike myotropic drugs, can increase the risks of its use: it should not be taken by children under 6 -years of age, simultaneously with antidepressants (especially tricyclics), antihistamines and antiarrhythmic drugs, as well as beta-agonists (high risk of negative interaction between these drugs). Hyoscine butylbromide, like other M-anticholinergics, worsens the condition of patients with reflux esophagitis, hiatal hernia due to relaxation of the lower esophageal sphincter and increased reflux of acidic contents into the esophagus. In elderly patients with chronic atonic constipation, in weakened patients, there is a risk of developing intestinal obstruction. In case of chronic lung diseases, when using M-anticholinergics, thickening of secretions may occur and the degree of bronchial obstruction may increase. In men, a decrease in potency is possible.
With prolonged use, the drug should be discontinued gradually; during treatment, it is strictly forbidden to drink alcoholic beverages, be in the hot sun, perform intense physical work or play sports (impairment of the functions of the sweat glands by the drug with simultaneous insolation can lead to heat stroke).
Thus, the status of hyoscine butyl bromide as an over-the-counter drug does not relieve the patient from the need for periodic medical monitoring. It is precisely these problems that are responsible for the fact that currently the M-anticholinergics known to us abroad are used less and less often. In addition, the severity of their effect depends on the initial tone of the parasympathetic nervous system, which determines significant individual differences in the effectiveness of drugs in patients with varying severity of vagotonia.
Phosphodiesterase inhibitors (PDEs)
The effect of traditional widely used antispasmodics, such as drotaverine (No-shpa), is based on the suppression of PDE IV activity. Since PDE IV is present in smooth muscle cells along the entire length of the intestine, biliary and urinary tracts, its blockade with drotaverine (No-shpa) has a universal antispasmodic effect, regardless of the degree of contraction or the cause that caused it. Drotaverine, unlike hyoscine butylbromide and other myotropic antispasmodics, has anti-edematous and anti-inflammatory effects (type IV PDE is actively involved in the development of inflammation).
Pharmacodynamic properties underlie the pathogenetic therapeutic effect of drotaverine and are widely used not only to relieve acute spastic syndrome, but also to provide long-term pharmacotherapy, for example, with biliary dyskinesias, cholelithiasis, chronic intestinal diseases with spastic syndrome accompanied by colicky or bursting pain. The absence of anticholinergic activity has a positive effect on the safety of drotaverine, expanding the range of people to whom it can be prescribed, in particular, restrictions on use in children are lifted (possible from the age of one year), in elderly men with prostate pathology, as well as with concomitant pathology and when taken together with other drugs.
The therapeutic concentration of drotaverine in plasma when taken orally is observed within 45 minutes. After a single oral dose of 80 mg, maximum plasma concentration is achieved after 2 hours, and oral bioavailability is 60%. The drug penetrates well into various tissues, is metabolized (oxidized) almost completely to monophenolic compounds, the metabolites are quickly conjugated with glucuronic acid. The half-life is 16 hours. About 60% of drotaverine when taken orally is excreted through the gastrointestinal tract and up to 25% in the urine. The presence of a dosage form for both enteral and parenteral administration makes it possible to widely use the drug in an emergency situation, followed by a transition to oral administration for long-term use. Thus, parenteral administration of drotaverine (No-shpa) provides a quick and strong antispasmodic effect, which is especially important in the development of acute, intense colicky spastic pain.
Drotaverine (No-shpa, No-shpa forte) is effective in the treatment of various gastrointestinal diseases characterized by spasm of smooth muscles (biliary dyskinesia, spasm of the sphincter of Oddi, pylorospasm, irritable bowel syndrome), is actively used for urolithiasis, increased blood pressure, disorders of regional blood flow, including for self-medication.
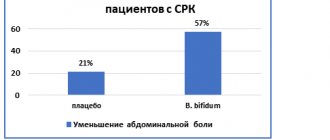
In a double-blind, placebo-controlled clinical trial, the use of No-shpa significantly reduced pain in sphincter of Oddi dyskinesia in 60% of patients, while placebo did not affect the intensity of pain in 55% of cases. In this study, No-shpa turned out to be 2 times more effective than analgesics. The research results showed that No-Spa is the drug of choice for spasms of the smooth muscles of the biliary system, both for monotherapy and in combination with other drugs and surgical methods of treatment. In a double-blind, randomized, placebo-controlled study in 62 patients with irritable bowel syndrome and constipation, abdominal pain (by 47%) and flatulence significantly decreased during 8 weeks of treatment with No-shpa. In another randomized, double-blind study, the effectiveness of No-shpa was studied in 70 aged patients with irritable bowel syndrome for 4 weeks. The results showed that No-shpa significantly reduces the frequency of pain compared to placebo - by 47% (p < 0.001), flatulence by 21% and dyspepsia - by 20% (p < 0.001), improves passage time in the colon [11] .
Long-term use of the drug is safe, which is associated with the absence of an effect on cholinergic structures and significantly improves its tolerability. No-spa is included in the standards for the diagnosis and treatment of diseases of the digestive system approved in the Russian Federation.
Sodium channel blockers
The action is based on disrupting the depolarization of the membrane of smooth muscle cells of the gastrointestinal tract, reducing the permeability of the membrane to extracellular sodium and, in addition, indirectly suppressing the release of potassium from the cell. The result of this is a disruption of the depolarization process and blocking of intracellular calcium stores. The most well-known drug is the veratric acid derivative mebeverine. It binds to the molecular structures of sodium channels without affecting the cholinergic receptor, reduces the outflow of ionized potassium from the cell, and therefore eliminates spasm without causing hypotension of the colon [12]. Metabolized when passing through the intestinal wall and liver, drug metabolites are excreted in the urine.
Mebeverine is prescribed mainly for functional diseases of the gastrointestinal tract (non-ulcer dyspepsia, irritable bowel syndrome), as well as for secondary spasms caused by organic diseases of the intestines and biliary tract. It is used exclusively as planned, i.e., only a course of treatment is provided, unlike drotaverine, which can be used both for the relief and prevention of spastic pain.
The effectiveness of mebeverine is not always observed with monotherapy. Thus, in an extensive pharmacoepidemiological study [13], it was shown that in irritable bowel syndrome in comparison with control (standard therapy), it requires more joint drug support than in control, which leads to increased costs (Table 2).
From the table 2 it is clear that the odds ratio is always higher in the mebeverine group, which indicates a greater likelihood of prescribing concomitant pathogenetic therapy in comparison with traditional treatment. In addition, using a representative group (n = 3431), it was found that when using mebeverine, the likelihood of hospitalization for various diseases increases, which indicates the variability of the therapeutic effect of the drug and is accompanied by an increase in treatment costs (Table 3).
IN
The main indications for prescribing antispasmodics for diseases and conditions of internal organs have been formulated.
Conclusion
Pain is a universal symptom for a wide variety of lesions of internal organs; its occurrence is often based on spasm of smooth muscles. Knowledge of the clinical pharmacology of drugs in this group allows for the most targeted choice of drug. Using the pharmacodynamics of drugs, it becomes possible to combine them rationally, effectively and safely. Of the entire group of antispasmodic drugs, the most popular is drotaverine (No-spa), which meets the criteria of effectiveness, safety and cost-effectiveness to a greater extent than the others. A review of research results shows that No-Spa is effective both for the rapid relief of acute pain caused by spasms, and for a fairly long-term treatment of patients with chronic pathology. Unlike other antispasmodics, the effect of No-shpa is not limited to the gastrointestinal tract, which makes the drug universal for relieving spasmodic conditions of any origin and location and the associated pain syndrome. An important feature of the pharmacodynamics of No-shpa is the lack of effect on cholinergic structures, which makes the drug safer compared to M-anticholinergics. The mechanism of action, which is different from other drugs in the group, provides opportunities for a wide effective combination both within the group of antispasmodics and with drugs from other pharmacological groups (antisecretory, non-narcotic analgesics, opioids).
For questions regarding literature, please contact the editor.
M. V. Pchelintsev , Candidate of Medical Sciences, Associate Professor Institute of Pharmacology of St. Petersburg State Medical University named after. acad. I. P. Pavlova , St. Petersburg
Groups and types of antispasmodic drugs
According to the type of effect, antispasmodics are divided into:
- Myotropic - act directly on smooth muscles. This group of antispasmodic drugs includes products based on papaverine, dibazole, aminophylline, theobromine, magnesium sulfate, drotaverine hydrochloride (No-Shpa 40 mg).
- Neurotropic - stops the occurrence of nerve impulses that cause spastic muscle contractions. Such drugs include, for example, atropine. Some drugs from this group affect the functioning of blood vessels, so they should only be prescribed by a doctor.
To eliminate spasms and the pain caused by them in childhood, it is most often recommended to take drugs of the first group (for example, based on drotaverine hydrochloride).
Types of medications for spasms:
- tablets, capsules;
- candles;
- solutions for injections (in ampoules).
Sodium channel blockers
These drugs affect the contraction mechanism differently. They block sodium channels, which prevents sodium ions from entering the cell, and, as a result, the cell does not enter an excited state. Thus, they also prevent the replenishment of calcium stores in the cell5.
Representatives of this group include mebeverine. After taking the drug, the antispasmodic effect is associated with a decrease in the tone and contractile activity of the smooth muscles of the gastrointestinal tract, especially the large intestine. Prescribed for intestinal spasms of organic and functional origin3, 5, 7.
Prevention of spasms
To avoid cramps, you should take care of your health:
- organize nutritious meals;
- take multivitamin and mineral complexes;
- study the effects of drugs recommended by doctors, take medications from trusted brands;
- do not forget about physical activity, restorative procedures, hygiene;
- ensure timely and correct treatment of any diseases, preventing their chronicity.
On the MIS Pharmacy 9-1-1 website, at any time of the day, you can select and order all the necessary goods and medical products with delivery in Kyiv and all cities of Ukraine at a competitive price. Simply place the selected items in your cart and confirm your order. Cosmetics and some types of medical equipment are also available. Choose!
Popular questions
What to drink for a spasm?
If your stomach hurts, you can take antispasmodics to reduce pain before seeing a doctor. They practically do not distort the clinical picture if the pain is caused not by a spasm, but, for example, by an inflammatory process.
Why are antispasmodics taken?
Antispasmodics relax the smooth muscles of the hollow organs of the human body. This allows you to establish their proper functioning, eliminate pain, and effectively treat the underlying disease (for example, removing stones from the kidneys).
Spasms can be not only a consequence of the disease, but also the cause of its development. For example, due to prolonged spasm of the biliary tract, obstructive jaundice may develop. Therefore, patients with chronic diseases of the respiratory system and gastrointestinal tract should keep a package of antispasmodics in their home medicine cabinet.
Phosphodiesterase activity inhibitors
These drugs block the enzyme phosphodiesterase, which leads to an increase in the concentration of cyclic adenosine monophosphate (cAMP) in the cytoplasm of smooth muscle cells and, as a consequence, to a decrease in the concentration of intracellular calcium. The action of the drugs papaverine and drotaverine5 is based on the suppression of phosphodiesterase activity. This is the most universal class of antispasmodics, which help eliminate spasms not only in different parts of the gastrointestinal tract, but also in the biliary and urinary tracts.
The mechanism of action and safety profile of phosphodiesterase inhibitors have been well studied, so they are used to relieve acute painful spasms and can also be used as long-term therapy after consultation with a physician to ensure long-term antispasmodic effects11, 13.
There are significant differences between papaverine and drotaverine. drotaverine (no-shpa®14 and no-shpa® forte15) blocks the action of exactly that type of phosphodiesterase that acts in the muscle cells of the abdominal organs12.
The selectivity of drotaverine is 5 times higher than that of papaverine12. At the same time, drotaverine has a more favorable safety profile compared to papaverine12. In addition, drotaverine (No-shpa® and No-shpa® forte) has additional mechanisms of action similar to antispasmodics from other groups: closing sodium and calcium channels13.