A blood test for intestinal cancer is a mandatory test that allows you to identify severe pathology in the early stages and begin treatment on time. By regularly taking tests, the patient can monitor their health status and take timely measures if their health worsens.
The easiest way to monitor the development of the oncological process is with the help of a general and biochemical blood test. To successfully conduct the study, you need to explain the preparation rules to the patient.
If a patient has several main symptoms of intestinal cancer and at least one minor one, a clinical blood test will allow an accurate assessment of the degree of development of the pathological process in the body.
Causes and risk factors for colon cancer in women and men
Scientists believe that a diet high in animal fats and limited in fruit and vegetable fiber may contribute to the development of bowel cancer.
But the exact causes of bowel cancer are unknown. Experts have identified a number of risk factors that increase the likelihood of developing the disease. It will be promoted:
- if there is intestinal cancer in the family or polyps have been detected;
- if the patient has inflammatory bowel disease;
- Long-standing ulcerative colitis has been identified, but there is also an association with some cases of Crohn's disease.
If a person eats a high-fat diet, this is considered a contributing factor to the development of bowel cancer. The World Health Organization states that a diet high in processed and red meat (bacon, sausages, deli meats) is a contributing factor to the development of bowel cancer, including in children.
Colon cancer
Where does colon cancer come from and how does it start? This question is often asked by patients, and perhaps right now you are asking yourself this problem. Let's try to answer this question by studying the development of colorectal cancer and determining who is at risk.
Cancer is a disease characterized by uncontrolled cell division and growth. Under normal conditions, the cells of your body constantly reproduce themselves, with new cells replacing old ones that die over time. This process of obligatory and planned cell death is called “apoptosis.” When this process works as it should, the body maintains a balance between new and old cells, and you remain a healthy person.
The process of apoptosis is controlled by genes that are located in the nuclei of all cells. They consist of DNA (deoxyribonucleic acid) chains, from which information on the functioning of all body processes is read - from eye color to human height. Genes also make proteins that serve as signaling agents for cells, telling them when and how to grow, divide, and die.
Cancer can form when a specific set of these genes in a specific cell undergoes constant disruption (called mutation) throughout life. Mutations can be the result of hereditary factors, lifestyle (smoking, diet) or a combination of these.
Once mutated, the genes begin to function abnormally. They produce excess amounts of proteins that stimulate cell growth, and in some cases, their ability to suppress tumor growth is impaired. As a result, the process of apoptosis, which restrains tumor growth, stops working and the cells do not undergo self-destruction, as happens under normal conditions. These abnormal cells begin to divide very quickly, forming a tumor. This rapid division continues and the cancer grows and spreads away from where it started. This process is called metastasis.
Genes and colorectal cancer.
Genes that are involved in the formation of colon cancer include:
- APC or p53 (tumor suppressor genes). Normally, these genes suppress the process of cell division and are responsible for inhibiting the formation of tumors by controlling the rate of cell division. The loss or disruption of the function of these genes can be compared to the breakdown of the brake system of a car: when the gene does not work, uncontrolled cell growth occurs, like a car that rushes without stopping and control.
- k-RAS oncogene. Typically, oncogenes and suppressor genes work together to regulate normal cell division. Suppressor genes are responsible for turning off cell growth processes, oncogenes are responsible for turning on this process. But when an oncogene mutates and changes its structure, or accidentally duplicates during cell division, it can trigger rapid cell division that leads to the formation of a cancerous tumor. If the result of a suppressor gene mutation can be compared to a broken brake in a car, then an oncogene mutation is usually compared to the gas pedal being pressed to the floor. It causes cells to divide endlessly, and the process of abnormal cell division gets faster and faster.
- Genes hMSH2 and hMLH1. These genes produce signaling proteins that are responsible for repairing or repairing DNA that may have made mistakes when it is duplicated during cell division. Mutations of these genes lead to disruption of recovery processes. It is believed that these errors can accumulate and lead to changes in other genes responsible for regulating cell growth.
The sequence of polyp-cancer transformations.
It is believed that most colorectal tumors arise from benign polyps. Beginning in the 1980s, the importance of polyps in the formation of colon cancer became very relevant to the general public after US President Ronald Reagan was diagnosed with colon cancer. The president was tested for occult blood in the stool, after which they discovered polyps in the intestines, and one of them turned out to be malignant. Polyps are round formations that appear as a result of thickening of the inner lining of the colon and protrude into its lumen. Polyps can have different shapes: flat or mushroom-shaped (have a so-called stalk).
Although most polyps remain benign, some, if not removed, can degenerate or transform into malignant (cancerous) tumors. The process of transformation of polyps is most likely caused by genetic mutations in the cells. There are different types of polyps, but only one type is thought to develop into cancer. This type of polyp is called adenomatous polyp.
Until you have a special examination (colonoscopy), you cannot be sure that there are no polyps in your intestines, because polyps do not cause any symptoms. Large polyps or tumors may cause symptoms such as bleeding, blood in the stool, anemia, or bowel obstruction. These symptoms are quite rare and only begin to appear when the polyps become very large or cancerous.
Colon cancer does not develop overnight; it is believed that it takes 5-10 years for a polyp to transform into a malignant tumor. If an adenomatous polyp exists in your intestines for many years, and you do not know about it because you do not do a special examination, sooner or later it may turn into a tumor. As a tumor grows, it increases in size, grows deeper into the intestinal wall, and can even invade neighboring organs. If tumor cells enter the lymph nodes or blood vessels, they spread throughout the body and form tumor metastases in other organs - the liver, lungs, and brain. At this stage of the disease, treatment becomes very difficult.
In conclusion: Almost all colorectal cancers develop due to gene mutations. Many of the mutations that lead to colorectal cancer involve disruption or loss of genes that suppress tumor formation or support normal cell growth and division. It is widely believed that external factors do not directly cause the formation of cancer, but only trigger genetic mutations that lead to its appearance. In other words, if genes are compared to a light bulb that can be turned on, then external factors are a switch that, when pressed, turns on these genes. But even if you have inherited “bad” genes, you can reduce the risk of the disease by undergoing regular testing and leading a healthy lifestyle. Therefore, it is important to understand your personal risk factors for colorectal cancer—those conditions that increase or decrease your likelihood of getting the disease.
Five myths about colon cancer.
Myth one. Colon cancer occurs only in older people; young people do not get it.
According to statistics, the incidence of colorectal cancer increases with age, but even so, young people in their 20s and 30s can develop colon cancer. It is known that about 7% of colorectal cancer cases occur in people under 50 years of age. Young people who have already had colorectal cancer are at much higher risk of developing a second colorectal cancer. Therefore, although colon cancer most often affects people over 50 years of age, the disease can also happen to younger people. And you should always remember that if this disease is detected at an early stage, it can be completely cured in more than 90% of cases.
Myth two. Colorectal cancer affects mostly men. Don't believe it. Although there are diseases that primarily affect men or women, colorectal cancer is not one of them. This is a disease that occurs equally often in both men and women. Dear women, it is dangerous to think that only men get colon cancer. You need to know and be able to identify the main symptoms of this disease, just as you know the possible manifestations of breast or cervical cancer. It is necessary to include in regular examinations, along with mammography and vaginal smears, also special studies for the diagnosis of colorectal cancer.
Myth three. No one in my family has had colon cancer, so I am not at risk. So many people think this way and it's so sad! Indeed, if a person has had multiple family members from previous generations with colon cancer, this results in a significantly increased risk of the disease in subsequent generations. However, it is necessary to understand that about 80% of patients with colorectal cancer do not have a family history of this disease. Let's forget about statistics for a moment and talk about real life. Any coloproctologist surgeon will confirm that a very large number of people who have never had colon cancer in their family become ill with this disease and often consult a doctor at an advanced stage. They were not examined, thinking that they did not need this examination, since no one in their family had such a disease. However, if the disease could be diagnosed at an early stage, it could be cured without a trace.
Myth four. If I feel well, I don't have to worry about having bowel cancer. This is the most terrible myth of all. What do you think is the most common symptom of early stage colon cancer? Do you think it's blood in the stool or constipation? No. In fact, early stage cancer does not manifest itself in any way; it does not have any special symptoms. People with early-stage colorectal cancer feel well, their condition does not change in any way compared to normal health. Only when the tumor grows can it make itself felt. It is now believed that in the average person, intestinal cancer develops from polyps, which over a long period of time degenerate into a tumor. While this tumor is small, it does not cause pain or other symptoms. If a tumor is detected at an early stage, a person can be cured of cancer. There is no need to wait for symptoms of the disease; it is better to undergo regular examinations while you feel well.
Myth fifth. Cancer always starts with blood in the stool. There is some truth behind this myth. For all people, the appearance of blood in the stool causes fear. In most cases, bleeding from the rectum is associated with hemorrhoids. Yes, colon cancers can cause bleeding from the rectum. However, its amount may be small and even invisible without a microscope. In some cases, with intestinal tumors, there may be no blood in the stool at all. If there is bleeding, but it is not noticeable, then its manifestations may be increased fatigue, which is associated with anemia and a lack of iron in the blood. Anemia can only be detected by doing a general blood test, which calculates the number of red blood cells, hemoglobin content and hematocrit. Blood in the stool is just one possible symptom of large colon cancer. Remember that small tumors at an early stage may not manifest themselves in any way (see myth four). With a large tumor, characteristic symptoms may appear (see table). Impaired stool evacuation may occur because the tumor narrows the intestinal lumen and stool cannot pass through the narrowing. In this case, a person may suffer from constipation, nausea, bloating, the shape of the stool may change - it may become ribbon-like, and there may be a feeling of incomplete bowel movement. In more advanced stages, there may be loss of appetite and unexplained weight loss. These symptoms arise due to the fact that, as the tumor grows and spreads, it releases special substances into the blood. Therefore, if you have any of these symptoms, you should consult a doctor immediately.
Please do not let these myths stand in the way of possibly saving your or another life!
Colorectal Cancer Symptom Assessment Sheet. Like most people, you may not feel comfortable discussing your bowel function. However, you will have to change your views. If you don't tell your doctor about unusual symptoms, such as a change in the shape of your stool, he or she will never know about it and most likely won't even ask! Here's a quick rundown of what to look out for.
Please don't be scared! Most of these symptoms occur in many people and are not related to cancer. However, let your doctor decide this.
- * Changes in the mode and nature of bowel movements - one-time or chronic diarrhea or constipation, discomfort during bowel movements, changes in the shape of the stool (pencil-thin or thinner than usual), a feeling of incomplete bowel emptying.
- * Unusual sensations associated with the intestines, such as increased gas formation, pain, nausea, bloating, a feeling of fullness in the intestines.
- * Bleeding (light red or very dark blood in the stool).
- * Constant fatigue.
- * Unexplained weight loss.
- * Unexplained iron deficiency.
- * Unexplained anemia.
Hospitalization (patient stay in hospital).
At the preoperative stage, the necessary studies are performed to prepare for the operation, consultations with specialists, as well as preparatory treatment (intravenous infusions, special nutrition, treatment of concomitant diseases). The second stage is surgery. And the third (postoperative) stage is recovery after surgery and discharge home.
The length of a patient’s stay in the clinic depends on the type of disease and its severity, the number of necessary examinations, the type of operation, as well as the course of the postoperative period.
Due to the desire of clinics to reduce the costs associated with hospital stays in the preoperative period, there is currently a tendency to perform many examinations on an outpatient basis. This means that before surgery, the patient comes to the clinic only to perform prescribed tests, and then returns home. After all the studies have been completed, the doctor sets the day of the operation, and the patient is hospitalized at the clinic the day before (1-2 days before the scheduled date). In many European countries and the United States, patients scheduled for surgery arrive at the clinic early in the morning on the day of surgery, undergo a short preparation in a special preoperative ward, and are sent to the operating room 2-3 hours later. Keeping the patient at home with loved ones until the day of surgery can reduce the stress associated with the need for surgery. However, in our country, due to the peculiarities of legal registration of medical history, such a practice is difficult, and to perform a major colorectal operation, the patient must be hospitalized the day before or several days before the surgical intervention.
Preoperative examination. Once a patient is suspected of having colon cancer and surgery is planned, there are several other important tests that need to be done before surgery.
This survey has two main objectives. First, by performing several tests, the stage of the tumor and the extent of its spread can be determined. Determining the stage of the tumor in the preoperative period will help you choose the right treatment tactics. Obviously, treatment for colon cancer that has metastasized to the liver will be very different from treatment for a small tumor that does not extend beyond the intestinal wall. Secondly, additional studies will help evaluate overall health and tolerability of surgery. Since surgery is extremely stressful for the body and can worsen existing problems with the lungs, heart, kidneys and other organs, special testing will help identify those patients who are at increased risk for complications in these organs during and after surgery.
- Chest X-ray . The main purpose of this study is to evaluate the presence of cancer metastases to the lungs. This is a standard test that can determine with fairly high accuracy whether there are tumor nodes in the lungs. Chest X-rays can also look for signs of heart and lung disease. Therefore, this study is performed routinely in all patients before major operations.
- Computed tomography (CT) of the abdomen and chest. Using this study, you can evaluate the condition of the liver and abdominal cavity for the presence of foci of tumor metastasis. If a chest CT scan is performed along with an abdominal examination, then a plain chest x-ray is not required.
- Magnetic resonance imaging (MRI) of the pelvis . This study allows you to obtain clear images of the pelvic organs, assess the extent of spread of the rectal tumor, damage to the lymph nodes, and involvement of the anal canal muscles in the tumor. Unlike radiography and CT, MRI does not expose patients to ionizing radiation.
- Positron emission tomography (PET). This type of examination uses a contrast agent containing a radioactive form of glucose, which helps determine the location in the human body where the tumor is located. Although this method can accurately identify “occult” tumor metastases that cannot be detected using CT or MRI, PET is currently not the method of choice for the preoperative evaluation of patients with colorectal cancer.
- Ultrasound examination (ultrasound) of the abdominal cavity . Using this method, you can determine the condition of almost all abdominal organs and suspect the presence of tumor metastases in other organs, most often in the liver. You can also evaluate the condition of the kidneys, pancreas, and gallbladder. If it is not possible to perform a CT scan of the abdominal cavity, this study is the method of choice for assessing the presence or absence of distant metastases.
- Transrectal ultrasound (TRUS). This study is performed using a special sensor, which is inserted into the rectum through the anal canal. This method allows you to identify the degree of tumor invasion of the rectal wall, assess the condition of nearby lymph nodes and rectal sphincters. If it is not possible to perform an MRI of the pelvic organs, it is the method of choice for assessing the spread of a rectal tumor.
- Blood tests . A standard set of blood tests includes: a complete blood count, a biochemical blood test and a blood clotting test.
A complete blood count evaluates the total number of red blood cells (red blood cells), hemoglobin, leukocytes (white blood cells), and platelets. These cells play a crucial role in the functioning of the body. Red blood cells, with the help of the hemoglobin they contain, are an oxygen carrier and are responsible for supplying oxygen to all tissues and organs. In colorectal cancer, bleeding may occur from the tumor, so the number of red blood cells in such patients may be reduced. In severe cases, a blood transfusion may be required after surgery, and sometimes before surgery. Because platelets play an important role in normal blood clotting (blood clotting), counting these blood cells is a necessary test. If the patient has not had any episodes of abnormal bleeding in their lifetime, such as heavy nosebleeds or bleeding from the gums of teeth, there will likely be no abnormalities in this test. However, studying the platelet count is very important to determine the possible risks of bleeding during surgery.
As part of a biochemical blood test, plasma electrolytes, such as potassium and sodium ions, are assessed. Levels of these ions can be very low or high in patients taking medications for high blood pressure or other medications. Before surgery, it is necessary to restore the normal level of these ions in the blood plasma.
The blood clotting profile evaluates the effectiveness of clotting, which is important to know because blood clotting may be impaired in patients with hemophilia or other clotting factor disorders.
Also mandatory tests that are done to all patients before surgery are determination of blood group and Rh factor , since these data may be required for blood transfusion, and determination of markers of infectious diseases - viral hepatitis (B and C), syphilis, HIV infection. In the absence of all these tests, the operation is impossible.
- Electrocardiography (ECG) . This is a simple screening test that can determine heart function. It can help identify signs of atherosclerotic heart disease (narrowing of the arteries of the heart), which is a serious risk during surgery. ECG signs of a previous myocardial infarction or cardiac ischemia (lack of blood supply to certain areas of the heart due to insufficient blood flow) are signs of atherosclerotic damage to the coronary arteries (arteries of the heart). If you receive an abnormal ECG picture, you may need to perform additional tests, which will be prescribed by your doctor or cardiologist.
What to take with you to the hospital. You should be prepared to stay in the clinic for several days. Be practical and use common sense. Do not take valuables, fashionable clothes or large amounts of money with you. Bring a small bag with the essentials. You will need leg compression stockings, which help reduce the risk of blood clots during long surgery. This can include elastic bandages or special compression stockings. Immediately after the operation, to protect the sutures of the anterior abdominal wall, you will need to constantly wear a bandage - this is a special wide elastic belt that helps support the muscles of the anterior abdominal wall at times when there is strong pressure on it - when you stand up, cough, sit down or bend over. You will only be in bed for one or two days after surgery, after which you will be encouraged to get up and walk around. You may want to wear a robe or comfortable pajamas and slippers with non-slip soles. After surgery, for some time, a small amount of wound discharge may be released from the sutures, which, even through a sterile dressing, can stain clothing. Therefore, prepare two sets of clothes and do not take expensive or favorite things, as they may get damaged in the hospital.
Don't forget toiletries such as a toothbrush, toothpaste, comb, deodorant, perfume or cologne, they will help you feel more “human” after surgery. During surgery, patients should not wear contact lenses, so do not wear them on the day of surgery; instead, it is better to wear glasses and leave contact lenses for the period after surgery. Before the operation, give valuables and wallet to your family members, leave a small amount of money to pay for television or telephone. You may also benefit from a good book, some magazines or a craft kit to help pass the time during your final days in the clinic when you feel better.
If you regularly take any medications (for example, for high blood pressure or diabetes), be sure to take them with you. It is very important that you continue to take these medications until the day of surgery, unless your doctor prescribes something else.
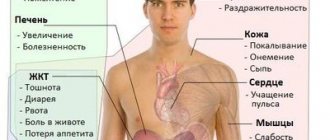
Symptoms
If a person's intestine is affected by cancer, the initial symptoms may not be noticeable and do not necessarily cause illness.
Often, the initial forms of the lesion are determined during screening or during examinations for other reasons. More than 90% of people with bowel cancer have 1 of the following combinations of symptoms:
- persistent changes in bowel function;
- more frequent urination, loose stools, and sometimes abdominal pain;
- blood in the stool without other rectal symptoms (when hemorrhoids or anal fissures are unlikely to be the cause);
- Abdominal pain, discomfort or bloating is always caused by food, which sometimes leads to a decrease in the amount of food eaten and weight loss;
- Constipation, rarely hard stools, is rarely caused by serious intestinal diseases.
It is important to see a doctor if a person has 1 or more symptoms of bowel cancer that persist for more than 4 weeks.
Rare bowel cancer syndromes are intestinal obstruction or intussusception. In some cases, bowel cancer can stop digestive waste from passing through the intestines. Symptoms of intestinal obstruction may include:
- periodic and sometimes severe abdominal pain that does not go away;
- unintentional weight loss with constant abdominal pain and swelling, bloating;
- lack of stool and passing gas, increasing general malaise.
Intestinal obstruction is a medical emergency. Without surgery or other urgent measures, this threatens death.
CEA in blood analysis
The antigen is contained in the intestinal glands in small quantities and does not have any particular effect on the functioning of the body. If a tumor develops in the intestine, the concentration of CEA increases significantly. In patients suffering from cancer, the antigen level is increased to 90%. The normal value is 3 ng/ml.
In smoking patients, the marker value is 5.5 ng/ml, and for patients with a benign intestinal tumor this figure is 40.0 ng/ml.
The test for determining CEA is highly sensitive and depends on the size of the tumor. The occurrence of a relapse of the disease is indicated by a marker level above 25 ng/ml. In cancer patients, a decrease in the amount of antigen is detected after a 6-week course of treatment.
If the marker value remains constant, the presence of metastases should be assumed. CEA is determined at intervals of several months and great attention is paid to a sudden rise in the concentration of antigen in the blood. In this case, the presence of an extensive tumor process in the intestine should be assumed.
Chemotherapy treatment does not affect the value of CEA in serum.
Forms of bowel cancer
A disease such as intestinal cancer involves damage to various parts of the intestine, from the duodenum to the rectum.
However, lesions of the small intestine or duodenal cancer are extremely rare, the stages of the process and symptoms are similar, and digestive disorders predominate. When doctors usually talk about intestinal cancer, they mean the colorectal form of the tumor. When bowel cancer is diagnosed, additional tests are performed to determine the extent of the disease. The stages of colorectal cancer are as follows:
- Stage I (least common cancer): A tumor that affects only the innermost layers of the colon or rectum. The cure rate for stage I cancer is more than 90%, which emphasizes the importance of early detection of pathology.
- Stage II: cancer demonstrating active growth and spread of the tumor through the wall of the colon or rectum to adjacent structures.
- Stage III: cancer associated with the spread of the process to local lymph nodes (metastases).
- Stage IV (the most common cancer): The tumor cells have spread to distant organs, usually the liver and lungs or lymph nodes far from the original tumor.
Colorectal cancer screening
Colorectal cancer screening
is a preventive observation of patients at risk.
Screening activities include visiting a proctologist
and collecting stool samples for testing for
occult blood
and
the tumor marker pyruvate kinase
. It's simple and cheap.
According to statistics, a banal digital rectal examination can detect the presence of a tumor and its characteristics in 70% of cases, because the rectum is just the last 15 cm of the digestive system. In women, digital rectal examination is supplemented with vaginal examination.
Fecal occult blood test
Fecal occult blood test (Gregersen test)
It is recommended to take it annually for all people over the age of 40; if the result is positive, an unscheduled colonoscopy will be required.
Fecal pyruvate kinase test
Pyruvate kinase
– an enzyme that is produced by tumor cells and is used for the early diagnosis of precancerous diseases and colon cancer.
You can take all types of tests or arrange for them to be collected at home by contacting a medical office. We collect biological material in St. Petersburg and the Leningrad region: +7 (812) 323-07-49
And
+7
Diagnostics
If you have suspicious symptoms, you should consult a doctor immediately.
The doctor will ask some general health questions and may examine your anus (rectum). He does this by inserting a gloved finger into the anus (rectum) and feeling for lumps or swelling. The examination may be unpleasant, but it should not be painful. Blood tests may be ordered to look for anemia (which is common in people with bowel cancer) and to evaluate liver and kidney function. An X-ray of the chest and abdomen may be ordered.
A specialist may perform a sigmoidoscopy, which uses a small tube with a camera to look inside the anus and lower intestines. This tube also pumps a small amount of air into the bowel to slightly inflate it for clearer visualization of the bowel. The doctor will simultaneously take samples if he finds any abnormalities or polyps in the intestinal lining and send them for testing.
Colonoscopy is considered the “gold standard” of diagnosis, in which the entire large intestine is examined; the procedure will be similar to sigmoidoscopy and can take up to an hour. The doctor will examine the entire length of the intestinal mucosa and take samples if necessary.
CT colonography (or computed tomography) scans the entire abdomen and pelvis, looking for polyps or areas of bowel cancer. The specifics of bowel preparation depend on the age and condition of the patient, but ideally the entire bowel lumen should be cleansed with laxatives.
Sometimes a barium enema is required, which is an x-ray of the colon with contrast. Barium is a white liquid that mixes with water and goes into the anus (rectum). You will need to keep this fluid in your rectum while the x-ray is taken. The contrast easily reveals any lumps or swellings on the x-ray.
To detect metastases, an MRI of the whole body or specifically the lungs, liver, and abdominal cavity may be prescribed Source: Colorectal cancer: a guide for patients. Information for patients based on clinical guidelines from the European Society of Medical Oncology (ESMO). — 2016..
Types of colorectal cancer
by histological type
- Adenocarcinomas
. Most cases of colorectal cancer begin with the degeneration of secretory glandular epithelial cells lining the inner surface of the colon and rectum. When doctors talk about colorectal cancer, they almost always mean adenocarcinoma. Adenocarcinoma, as a rule, does not arise immediately, but with age from some subtypes of polyps or dysplasia at the site of their removal. However, there are also 2 aggressive subtypes of adenocarcinoma, such as signet ring and mucinous. Signet ring cell carcinoma (3-5% of cases) is diagnosed in young people under the age of 40. - Carcinoid tumors
. They start with a special type of cell inside the colon called the interstitial cells of Cajal. These tumors, which most often do not threaten to develop into cancer, can occur anywhere in the digestive tract. - Lymphomas
are cancers of immune system cells. Typically, non-Hodgkin lymphomas develop in the intestine from lymphoid tissue in the cecum and rectum. - Sarcomas
are malignant tumors that can arise in the blood vessels, as well as in the muscle layers or other connective tissues in the intestinal wall. Most often (from sarcomas) leiomyosarcoma is diagnosed, which develops from the muscular lining of the intestinal wall. - Scirrhous tumors.
During the growth of such a tumor, collagen is intensively formed, which gives the intestinal wall of the intestine hardness. - Neuroendocrine tumors
originate from neuroendocrine cells (APUD system). They have the appearance of a single (solitary) node.
Very rare, but found: gastrointestinal stromal tumor (GIST), adenosquamous carcinoma, small cell carcinoma, melanoma, squamous cell carcinoma in the transition zone between the rectum and anal canal.
Treatment methods
Modern medicine has made strides in recent years to develop effective treatments for bowel cancer once it has been diagnosed.
The choice of treatment methods depends on what stage the cancer is at, this will help oncologists determine how best to treat it Source: Current aspects of surgical treatment of colorectal cancer. Dauletbaev D.A., Kaliaskarov E.Sh., Menayakov M.T., Serikov N.S., Aubakirov E.A. Bulletin of the Kazakh National Medical University No. 1, 2016, p. 226-229. Surgery to remove cancer cells is the only treatment needed for most people with stage I and II bowel cancer. Segments of the colon containing cancer are removed, and 10 to 20 lymph nodes are removed, which are examined to determine whether the cancer has spread to other parts of the body. Most types of colon cancer can be removed without creating a permanent colostomy Source: Locally advanced colon cancer - aspects of surgical tactics. Kutukov V.V., Sluvko L.V., Sevostyanov V.V. Tyumen medical journal No. 2, 2010. p. 79-80.
Chemotherapy is the most common treatment currently available to help prolong life expectancy and improve quality of life after bowel cancer has spread to other parts of the body (stages III and IV). Chemotherapy will likely be used if the cancer has spread to local lymph nodes (stage III) because the risk of the cancer returning is high even if all visible signs of cancer have been removed by surgery. The chemotherapy drug is usually given as tablets or an injection into a vein, or a combination of both, and can last for a total of 6 months.
Radiation therapy (radiotherapy) uses high-energy rays to kill cancer cells. It is not often used for colon cancer, but more often for rectal cancer. This is because tumors in the rectum are more difficult to remove surgically than in other parts of the intestine. However, advanced bowel cancer may require radiation therapy. The goal of treatment is not to cure cancer, but to shrink it or slow its growth. This relieves symptoms such as pelvic or rectal pain.
Radiation therapy is painless and takes only a few minutes. The main side effects of radiation therapy include fatigue and weakness, skin soreness, and hair loss in the treatment area. For many people, the side effects of radiation therapy go away within a few weeks of finishing treatment, and they can return to their normal lives. But for some people, radiation therapy can cause long-term side effects. The possibility of long-term side effects may depend on the type of cancer, its size, and location. It may also depend on how close the cancer is to nerves or other important organs or tissues.
Immunotherapy is another method. The immune system is the body's natural defense that seeks out and destroys anything non-body tissue, including infections and cancer cells, before they can cause disease. The immune system manages to destroy most cancer cells, but some of them overcome the defense. Immunotherapy uses drugs that tag cancer cells, helping to destroy them.
Blood sampling: general analysis
In the morning, capillary or venous blood is taken for research. A general analysis for intestinal cancer allows us to determine the stage of the oncological process. The patient must follow the rules before starting the procedure. You should not donate blood after mental and physical stress, as well as diagnostic procedures. It must be taken into account that the total number of leukocytes increases significantly in the following cases:
- after eating;
- with a sudden change in temperature;
- due to emotional stress.
It is unacceptable to smoke before taking a general test, as the blood becomes thick and viscous. Taking large amounts of fluid causes a decrease in hemoglobin concentration.
You should pay attention to the position of your hand when drawing blood. The patient should place it on the table at chest level. It is not recommended to take alcohol, fatty foods and medications that affect blood composition before the procedure.
A general blood test for intestinal cancer is one of the necessary diagnostic methods, which helps to carry out specific cancer therapy with synthetic and herbal drugs.
Prevention
Lifestyle factors can contribute to the development of bowel cancer, so the following lifestyle changes should help reduce your risks:
- body weight control;
- regular exercise;
- maintaining a diet rich in whole grains, cereals, fruits and vegetables;
- reducing consumption of fats, salt and sugar;
- to give up smoking;
- reducing or stopping alcohol consumption.
Bowel cancer develops slowly and, if detected early enough, is limited to parts of the bowel and can be successfully removed. If a person is over 50 years old, an annual screening test will help detect any changes Source: Preventing Stomach and Colon Cancer. V.V. Egorenkov. Practical Oncology, T. 12, No. 2 - 2011..
Article sources:
- Prevention of stomach and colon cancer. V.V. Egorenkov. Practical Oncology, T. 12, No. 2 - 2011.
- Colorectal cancer: a guide for patients. Information for patients based on clinical guidelines from the European Society of Medical Oncology (ESMO). — 2016.
- Expression of the icam-1 gene in tumor cells of patients with colon cancer. Knyazev D.I., Novikov D.V., Sakharnova T.A., Presnyakova N.B., Kuznetsova O.S., Kazatskaya Zh.A., Spiridonova N.A., Alyasova A.V., Novikov V. .IN. Bulletin of Nizhny Novgorod University named after. N.I. Lobachevsky No. 2, 2010. p. 528-531
- Modern aspects of surgical treatment of colorectal cancer. Dauletbaev D.A., Kaliaskarov E.Sh., Menayakov M.T., Serikov N.S., Aubakirov E.A. Bulletin of the Kazakh National Medical University No. 1, 2016, p. 226-229
- Locally advanced colon cancer – aspects of surgical tactics. Kutukov V.V., Sluvko L.V., Sevostyanov V.V. Tyumen medical journal No. 2, 2010. p. 79-80
The information in this article is provided for reference purposes and does not replace advice from a qualified professional. Don't self-medicate! At the first signs of illness, you should consult a doctor.
Additional Research
In the vast majority of cases, a standard examination is sufficient. In difficult situations, if there are contraindications, additional research may be necessary.
Trephine biopsy under ultrasound control
Trephine biopsy
— tissue sampling using a special needle under ultrasound control. It is carried out when there is a suspicion of the presence of cancer cells in the lymph nodes. The doctor may also prescribe a biopsy of metastases based on CT and MRI data, if this is important when choosing treatment tactics.
Ultrasound of the abdominal organs
Ultrasound of the abdominal organs
will allow not only to conduct a trephine biopsy, but also to examine from different angles the degree of growth of a cancer tumor through the intestinal wall, to examine the exact characteristics (shape, size, mobility) and the presence of metastases in the abdominal cavity.
Transrectal and transvaginal ultrasound
In addition to assessing tumor invasion, transrectal (in men) and transvaginal (in women) ultrasound
allows you to determine the distance from the lower edge of the rectal tumor to the anal canal. This extremely important study will help decide the question of performing sphincter-sparing surgery. TRUS will also be prescribed when planning local excision of colon tumors.
Abdominal MRI
MRI of the abdominal cavity with intravenous enhancement
performed when planning liver resection (about 25% of patients with primary diagnosis of colorectal cancer already have liver metastases). CT does not always allow us to fully express the extent of the process.
X-ray studies
- Irrigoscopy
is a radiopaque examination of the intestine. Prescribed when endoscopic examination is impossible or has low information content (for strictures, deformities of the colon). - A survey radiography of the abdominal cavity
is prescribed if there are complaints of severe pain. X-ray allows you to visualize contractions, stretches, and displacements. - Two-view chest x-ray
is an alternative to chest CT for diagnosing metastatic colorectal cancer.
Diagnosis of distant metastases
- PET-CT (if metastases are suspected based on CT data), osteoscintigraphy (if metastatic lesions of the skeletal bones are suspected), radioisotope scanning of the liver
is prescribed to confirm distant metastases, if this determines treatment tactics. - MRI or CT scan of the brain with intravenous contrast
is performed if metastatic lesions of the brain are suspected. - Diagnostic laparoscopy
(if tumor dissemination through the peritoneum is suspected) helps to remove tumors, adhesions and take a sample of altered tissue for analysis.
Before the procedure, the patient is given an MRI, ultrasound, CT and X-ray of the digestive organs, biomaterial is taken for testing, and an ECG is also performed
.
Determination of mutations
- MMR microsatellite instability (MSI) analysis
plays a role in predicting and determining the potential sensitivity of tumors to chemotherapy. Tumors with a high degree of MSI are not prone to metastasis. - Analysis of a tumor biopsy for the RAS mutation (exons 2,3,4 of the KRAS and NRAS genes)
is carried out if distant metastases of adenocarcinoma are diagnosed or suspected. Patients with colorectal cancer need to determine the status of KRAS gene mutations when prescribing targeted treatment with panitumumab and cetuximab. In the absence of mutations in the KRAS gene, the effectiveness of treatment for metastatic colorectal cancer is very high. - Molecular genetic studies
are prescribed for patients with adenomatous polyposis, in the presence of a family history, high microsatellite instability and a relatively young (under 50 years) age of the cancer patient. The US National Cancer Network recommends testing 22 genes associated with hereditary forms of colorectal cancer, endometrial cancer and tumor syndromes. To diagnose Lynch syndrome, which accounts for 3% of all colon cancer cases, testing is performed for mutations in the MLH1, MSH2, MSH6, and PMS2 genes. Lynch syndrome can be suspected in cases where cancer is detected in a patient under the age of 50, as well as in several of his blood relatives of any age. If familial adenomatosis is suspected - the second most common hereditary polyposis syndrome, usually characterized by the presence of 20+ polyps in the patient - testing is carried out for mutations of the APC and MYH genes.