Malabsorption in the intestine (this disease is also called “malabsorption syndrome”) refers to a number of different conditions of the body, characterized by certain problems with the absorption of minerals and other beneficial substances obtained from food.
As a rule, such ailments do not develop on their own. Most often, they are just one of the symptoms of more serious problems with the body in general and with the gastrointestinal tract in particular. Accordingly, the clinical picture observed with intestinal malabsorption syndrome in each individual patient will largely depend on the course of the disease - the primary source of trouble.
Classification of the syndrome
Malabsorption syndrome can have hepatic and gastric forms.
According to the generally accepted classification of malabsorption syndrome, all diseases of this type can be divided into two large groups:
- disorders characterized by a decrease in the amount of digestive enzymes produced by the pancreas in the lumen of the small intestine;
- deviations in which there is a decrease in the concentration of bile acids in the abdominal cavity.
In turn, within the mentioned groups, the following clinical forms of the described syndrome can be observed:
- gastric;
- intestinal;
- hepatic;
- pancreatic.
Another popular option for classifying the described disease is to divide malabsorption syndromes into general and selective (or selective). However, such a system is far from perfect, since its use does not take into account the nature of the origin of the problem (congenital or acquired).
In addition, the described classification does not cover the whole layer of fairly common gastrointestinal diseases associated with membrane digestion. And finally, the last way to systematize the types of malabsorption syndrome known to doctors is to divide them into groups precisely according to the principle of the origin of the disease:
- Primary, or hereditary, disorders of intestinal absorption. This type of syndrome described is characterized by problems with enzymatic function. Simply put, the patient’s body does not produce enough compounds necessary for normal digestion. There are also known variants of hereditary disorders in which normal amounts of enzymes are produced, but their chemical composition differs from the standard one.
- Secondary, or acquired, intestinal absorption disorders. This type of malabsorption syndrome develops due to the patient developing other serious problems with the gastrointestinal tract. In this case, intestinal absorption disorders act only as a symptom of the underlying disease.
According to the type of occurrence, acquired malabsorption syndromes are divided into several independent groups:
- gastrogenic, developed as a result of stomach diseases;
- pancreatogenic, resulting from problems with the pancreas;
- hepatogenic, almost inevitable in case of certain disorders in the liver;
- enterogenous, naturally occurring in diseases of the small intestine;
- endocrine, arising due to problems with the thyroid gland;
- iatrogenic, which are a kind of side effect from the use of certain types of drugs (usually laxatives, antibiotics and cytostatics) or radiation therapy;
- postoperative, the name of which speaks for itself.
Causes of iron deficiency:
1.Increased need of the body for iron during pregnancy
During pregnancy, a woman’s body spends more than 1000 mg of iron. A woman’s need for iron during pregnancy can reach 15-18 mg/day, while outside of pregnancy the daily need is about 2 mg. This leads to a decrease in stored iron in all women by the end of pregnancy. It takes at least 2-3 years to restore iron reserves consumed during pregnancy, childbirth and breastfeeding.
2. Nutritional iron deficiency.
This type of iron deficiency occurs when there is insufficient supply of iron from food: vegetarianism, a passion for diets low in animal proteins. During pregnancy, a vegetarian diet is unacceptable.
- 3. Presence of a pathological background for the development of anemia
- use of intrauterine contraceptives (they increase menstrual blood loss);
- endometriosis
- uterine fibroids
- abnormal uterine bleeding;
- gynecological diseases accompanied by bleeding;
- heavy and prolonged menstruation;
- hypothyroidism and thyroid dysfunction;
- diseases of the gastrointestinal tract (peptic ulcer of the stomach and duodenum, erosive gastritis, nonspecific ulcerative colitis, etc.);
- diseases of the kidneys and urinary tract (chronic pyelonephritis, glomerulonephritis, etc.);
- multiple pregnancies and births (more than three) with an interval between births of less than two years;
- multiple births;
- pregnancy occurring during lactation;
- frequent abortions and spontaneous termination of pregnancy preceding this pregnancy;
- foci of chronic infection.
Features of the course of pregnancy in the early stages
- vomiting of pregnancy;
- bleeding.
- 5. Puberty and growth
- 6. Iron resorption deficiency
This type of anemia is caused by a decrease in the absorption zone of iron during gastritis, duodenitis, enteritis, resection of the stomach and large areas of the small intestine.
About the diagnosis of intestinal absorption disorders
Increased gas formation is a symptom of impaired intestinal absorption.
Like many other diseases, malabsorption syndrome can be diagnosed by some characteristic symptoms:
- frequent diarrhea, accompanied by copious mucus and stench;
- increased gas formation;
- sensations of discomfort, heaviness or even cramps in the stomach, which intensifies many times after each meal;
- fast fatiguability;
- obvious exhaustion, usually accompanied by noticeable weight loss;
- unhealthy pallor and other clinical signs of anemia;
- night blindness (as a rule, such a disorder develops when the body lacks vitamins);
- increased sensitivity of the skin to damage, expressed in the immediate appearance of bruises from almost any mechanical impact, which is a natural result of a lack of vitamin K in the body;
- characteristic bone aches and muscle pain, indicating calcium deficiency.
If you detect several of the above warning signs, the patient should immediately contact a good gastroenterologist to clarify the diagnosis.
The specialist will collect an anamnesis of the disease and prescribe all necessary additional examinations. Thus, today the following research methods are widely used to diagnose intestinal malabsorption syndrome:
- a blood test that determines the deficiency of certain useful substances in the body, as well as confirming (or refuting) the presence of anemia in the patient;
- stool analysis, which reveals the degree of digestibility of healthy fats obtained from food by the body;
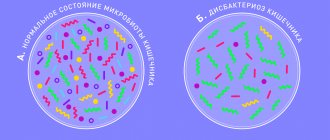
- analysis of the current state of the intestinal microflora obtained through a smear;
- a sample of the patient’s exhaled air, confirming or refuting the presence of lactose intolerance in the patient, and also allowing one to determine the approximate number of bacteria in the patient’s intestines;
- endoscopy, used primarily to obtain biological material for another study - biopsy of intestinal tissue;
- X-ray of the intestines (usually using a barium solution, which is necessary to obtain higher-definition images).
Publications in the media
Malabsorption syndrome can be caused by a defect in any stage of digestion or pathology of any of the gastrointestinal tract organs.
Etiology • Hypervitaminosis and hypovitaminosis E • Syndrome of impaired absorption of glucose and galactose (*182380, 22q13.1, transmembrane sodium glucose transporter gene SLC5A1, r).
Clinical manifestations vary, because malabsorption may involve one or more nutrients • Changed foul-smelling stool, films of fat or drops of oil can be observed on the surface of the toilet water • Loss of body weight • Edema and ascites secondary to hypoalbuminemia • Secondary anemia due to impaired absorption of iron, vitamin B12, folic acid or a combination thereof • Bone pain or fractures due to vitamin D deficiency • Paresthesia or tetany due to calcium deficiency • Bleeding due to vitamin K deficiency • Neuropathies and other manifestations of hypovitaminosis E • Muscle weakness due to potassium deficiency.
The diagnosis is based on clinical findings and confirmed by laboratory tests.
• Analysis of fat content in feces. A positive Sudan stain indicates fecal excretion of more than 15 g of fat per day. Fat content is determined in 72-hour stool samples. Normally, 93–95% of dietary fats are absorbed. Pancreatic disease is often associated with fat excretion in excess of 20–30 g/day.
• The d-xylose absorption test, which does not require enzymatic degradation or micelle formation for absorption, is used to assess the integrity of the intestinal mucosa. Take 25 g orally. Urine collected over a 5-hour period should contain at least 4–5 g of d-xylose.
• Test for unabsorbed carbohydrates. The entry of unabsorbed carbohydrates into the large intestine and their fermentation by bacteria reduces the pH of the stool; The condition is especially common in lactase deficiency, as well as in celiac disease and short bowel syndrome.
• Study of pancreatic functions. Bicarbonate content and total fluid secretion from the duodenum after secretin stimulation followed by the use of pancreatic chymotrypsin (bentyramide test) to release para-aminobenzoic acid excreted in the urine; urinary excretion of less than 60% suggests pancreatic insufficiency.
• Measuring the level of carotene in the blood. Vitamin A is fat soluble, and carotene levels are determined by vitamin metabolism; A low serum carotene level with normal vitamin A intake may be helpful in assessing fat malabsorption.
• Bacterial growth •• Culture of jejunal aspirates. Deviation from the norm: >104 microorganisms/ml. It is safe to assume dysbiosis in the presence of obligate anaerobes (clostridium and bacteroides), facultative anaerobes (lactobacillus and enterococci) or coliform bacteria •• Breath tests for the presence of bile salts are based on the ability of bacteria to deconjugate 14C-labeled glycine cholate before it can suck in. 14C-Glycine is then transformed into 14CO2 and measured in the exhaled breath of patients to detect bacterial overgrowth •• Urinary indican and 5-hydroxyindoleacetic acid test: elevated levels due to increased tryptophan metabolism; the test is nonspecific, because changes in the levels of tryptophan metabolites are also detected in carcinoid syndrome and Whipple's disease.
• X-ray of the small intestine is an informative diagnostic method, especially with air contrast. Sequestration or flocculation of barium suggests celiac disease. Thickened folds are seen in Whipple's disease, lymphoma, amyloidosis, radiation enteritis, Zollinger-Ellison syndrome, and eosinophilic enteritis.
• Schilling excretory test. Used to diagnose vitamin B12 malabsorption. The first stage of the Schilling test is the intake of 57Co-labeled vitamin B12, followed by determination of urine radioactivity. The second stage is to repeat the test after introducing the internal factor. Incomplete urine collection is a common cause of underestimated results, so radioisotopes in the blood plasma are analyzed at the same time. Low levels in blood plasma and urine indicate decreased absorption. Normalization of the results after the second stage of the test indicates the presence of B12-deficiency anemia and intrinsic factor deficiency. Low second-stage excretory test scores are often due to severe celiac disease, bacterial overgrowth, resection, or inflammation of the terminal ileum where absorption occurs. The presence of a high titer of antibodies to intrinsic factor in the gastric juice can also cause an underestimated result in the test with the intake of intrinsic factor.
• Biopsy of the small intestine. Flattening of the villi with infiltration of inflammatory cells is characteristic of celiac disease; isolated flattening of the vills is observed in infectious enteritis, giardiasis, lymphoma and bacterial overgrowth.
Treatment tactics for specific causes of malabsorption • Pancreatic insufficiency occurs in chronic pancreatitis, pancreatic carcinoma, cystic fibrosis. Changes in tests with bentiramide or secretin (pancreatic function test) are possible. Pancreatic enzyme replacement therapy is performed • Bacterial overgrowth accompanies changes in peristalsis (eg, diabetes and amyloidosis), small intestinal diverticula, strictures (eg, lymphoma and Crohn's disease) or the formation of blind loops after Billroth-II gastrectomy. Antibacterial therapy with ampicillin or tetracycline is often successful, and surgical correction of anatomical changes is possible • Celiac disease - see Celiac disease • Whipple's disease - see Whipple's disease.
ICD-10 • K90 Intestinal malabsorption
Complications of pregnancy with iron deficiency anemia
Anemia in pregnant women is a pathological background that contributes to the development of a number of complications of pregnancy and childbirth.
- Premature abruption of a normally located placenta, anomalies of labor.
- Increased blood loss during childbirth and bleeding - in 10% of women.
- In 8–12% of cases, the postpartum period is complicated by purulent-septic diseases and uterine subinvolution.
- A lactation disorder was detected, and both quantitative and qualitative changes in breast milk were observed.
- Adverse effects on the condition of the fetus: contributes to the development of fetal growth retardation syndrome, chronic fetal hypoxia.
- A decrease in adaptation of newborns in the early neonatal period is recorded in half of the cases.
Manifestations of iron deficiency anemia
Manifestations of anemia consist of 2 main syndromes: sideropenic and general anemic.
Sideropenic syndrome manifests itself:
- Seizures in the corners of the mouth;
- Glossitis - characterized by a feeling of pain, distension in the tongue, redness of its tip, and subsequently atrophy of the papillae;
- Inflammation of the red border of the lips;
- Dystrophic changes in the skin and its appendages (dry and pale skin, premature wrinkles, brittle nails and hair, the appearance of small cracks);
- Difficulty and painful swallowing of dense foods;
- Muscle weakness;
- Perversion of taste (there is a desire to eat inedible objects - chalk, tooth powder, coal, clay, sand, raw dough, minced meat);
- Perversion of the sense of smell (attraction to the smells of gasoline, kerosene, acetone, varnish, paints, dampness);
- Blue sclera syndrome;
- A pronounced predisposition to acute respiratory viral infections and other infectious and inflammatory processes.