general description
Cholecystitis is an inflammatory disease of the gallbladder, a consequence of complications of gallstone disease. Inflammation occurs due to a violation of the outflow of bile from the gallbladder and the presence of pathogenic microflora in the wall of the bladder.
Cholecystitis often affects people over 50 years of age, but it also occurs at an earlier age. In the scientific literature, cases of an attack of biliary colic in children 11-15 years old have been recorded. Elderly people aged 60-75 years and senile people account for 35-55% of the total number of cases of cholecystitis.
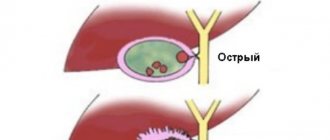
Cholecystitis can be: acute (according to the morphological picture it is divided into: catarrhal, phlegmonous and gangrenous) and chronic.
Causes
Causes of development of acute cholecystitis:
- Impaired outflow of bile from the gallbladder into the bile ducts, contributing to the development of pathogenic secondary microflora and impaired blood supply to the walls of the gallbladder
Blockage of the cystic duct with a stone
Causes of chronic cholecystitis:
- In the presence of a stone in the gall bladder, periodic inflammation occurs, followed by frequent exacerbations and remissions, ultimately leading to dystrophic changes in the wall of the gallbladder
- Parasitic diseases (giardiasis, opistarchosis)
- Atherosclerotic changes in the arteries supplying the wall of the gallbladder with impaired blood supply
According to the etiological factors, cholecystitis is:
- Calculous (with the presence of a stone or groups of stones in the gallbladder)
- Non-calculous (stoneless)
Folk remedies in the treatment process
Therapy of non-calculous cholecystitis with folk remedies includes the use of herbal decoctions and infusions with anti-inflammatory and antispasmodic effects. They are connected to the main treatment and have a good effect during the period of remission. All herbal decoctions are advised to be drunk warm before meals 30 minutes.
Patients are advised to alternate the intake of chamomile, calendula flowers, licorice root, rose hips, tea with mint and oregano. You can make combinations of them. You should take herbs in courses of 1.5–2 months, then take a break and repeat.
It is recommended to have chamomile in your home medicine cabinet; it will replace medications for many problems.
Symptoms
- Characterized by paroxysmal pain in the left hypochondrium, which can radiate to the right shoulder, scapula
- Nausea, vomiting
- Increase in body temperature to 38-38.5 C with chills
- The appearance of yellowness of the sclera, skin, itching
- Nausea.
- Dull aching pain in the right hypochondrium
- Bitterness in the mouth
- Possible prolonged low-grade fever
- Bloating
- Diarrhea
Diagnostics:
- General clinical analysis of blood and urine
- General analysis of stool for coprogram.
- Biochemical blood test (liver tests, cholesterol, alkaline phosphatase, amylase, glucose)
- Ultrasound of the hepatobiliary system
- ECG
- Cholecystocholangiography
- ERCP (endoscopic retrograde cholangiopancreatography)
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the abdominal organs (liver, gall bladder, pancreas, spleen) | 3 800 |
| Ultrasound of the abdominal organs with functional test | 4 000 |
| Gastroscopy (videoesophagogastroduodenoscopy) | 6 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Treatment
- Diet therapy (exclusion of foods that provoke symptoms of the disease: carbonated drinks, fatty foods, alcohol)
- Medications:
- Antispasmodic drugs: buscopan, dicytel, atropine, platifillin, no-spa
- Sorbents (activated carbon, enterosgel, smecta)
- Deoxycholic acid preparations (ursofalk, ursosan)
- Gastroenterological herbal collections
- Antibiotics: metronidazole, cephalosporins, fluoroquinolones
In case of acute cholecystitis, surgical intervention is required - emergency cholecystectomy.
The article was prepared by a specialist for informational purposes only. We urge you not to self-medicate. When the first symptoms appear, consult a doctor. We recommend reading: “Why you can’t self-medicate?”
Prevention of belching
To prevent the occurrence of pathological belching, you should undergo regular medical examinations. It is also recommended to limit the consumption of fried, fatty, spicy foods, legumes and foods high in yeast, fast food, confectionery, alcoholic and carbonated drinks. You should eat in small portions, avoiding overeating. It is not recommended to take a horizontal position immediately after eating.
Call our contact center at 8 (495) 230 03 09 and we will help you make an appointment with a specialist!
Types and symptoms of acute and chronic cholecystitis
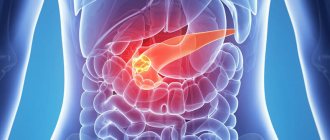
Cholecystitis is an inflammatory process in the gallbladder, most often provoked by infection of the organ with intestinal microflora against the background of a violation of the outflow of bile through a clogged cystic duct. Typically, cholecystitis is a complication of gallstone disease. The gallbladder is located next to the liver and is actively involved in the digestion process. The exit of bile occurs through the small intestine, but sometimes problems arise with evacuation, and the bile collects in the gallbladder, resulting in severe pain and an increased risk of infection.
Currently, Odeston has gained particular popularity. This is a drug for the treatment of most diseases of the biliary system, because... acts precisely in 3 directions.
First, it increases the formation and secretion of bile without stimulating gallbladder contractions, so it is safe even for patients with gallstones.
Secondly, it has a selective (targeted) antispasmodic effect, aimed only at the biliary tract.
And thirdly, it reduces bile stagnation, prevents cholesterol crystallization and the formation of gallstones.
As a rule, the disease occurs in combination with cholangitis - inflammation of the bile ducts. Cholecystitis is a common surgical pathology, especially among middle-aged and older women - they get sick three to eight times more often than their male peers.
The main reasons for gender predisposition to cholecystitis:
Chronic compression of the gallbladder during pregnancy provokes long-term consequences - an imbalance of cholesterol and bile acids, and, as a result, stagnation of bile;
Features of hormonal metabolism in women - it has been proven that progesterone, produced in large quantities during pregnancy and menopause, and other female sex hormones negatively affect the functioning of the gallbladder;
Women are prone to dieting, and strict dietary restrictions disrupt the motility (contractility) of the gallbladder.
The risk group, regardless of gender and age, includes people who have previously been ill:
Intestinal and/or liver infections;
Parasitic diseases (helminthic and protozoal infestations localized permanently or at one of the stages of development in the intestines and/or liver);
Gallstone disease (GSD) with obstruction (blockage) of the cervix and/or damage to the mucous membranes of the gallbladder;
Diseases that impair the blood supply to the walls of the gallbladder.
A reflex connection between pathologies of the gallbladder and anatomically unrelated abdominal organs has been proven - these are the so-called viscero-visceral reflexes. All of the above causes of cholecystitis are due to either a violation of the patency (obstruction) of the gallbladder, or a violation of its motility (dyskinesia).
Based on etiology, there are two large nosological groups of cholecystitis:
Calculous (lat. Calculus - stone);
According to the course, cholecystitis is divided into:
According to the nature of inflammation, they are:
Gangrenous and phlegmonous forms of the disease belong to the group of destructive cholecystitis.
The gallbladder is anatomically and physiologically close to the liver. The functions of the liver are varied, one of them is the continuous production of bile and its release into the duodenum. Excess bile accumulates in the gallbladder and is consumed in portions.
The role of bile in the physiology of digestion:
Dilutes food processed with gastric juice, changes gastric digestion to intestinal;
Stimulates peristalsis of the small intestine;
Activates the production of physiological mucus, which performs a protective function in the intestines;
Neutralizes bilirubin, cholesterol and a number of other substances;
Triggers digestive enzymes.
Symptoms of cholecystitis
The initial symptoms of cholecystitis, as a rule, are sharp pains in the right side below the ribs that occur unexpectedly. The reason for this is a stone that blocks the cystic duct. As a result, irritation and inflammation of the gallbladder develops.
The pain goes away after some time on its own or after taking a painkiller, but then it gradually increases, and then it becomes regular. The disease develops, which is accompanied by high fever, vomiting and nausea. The patient's condition continues to deteriorate.
The normal flow of bile into the intestines stops, a sign of which is the icteric coloration of the skin and eye sclera. The prerequisites for jaundice are precisely the presence of stones that block the bile ducts. The severity of the pathogenesis is characterized by the patient’s pulse: usually the heart rate ranges from eighty to one hundred and twenty to one hundred and thirty beats per minute (or even higher), which is a serious sign, meaning that dangerous changes have occurred in the body.
As for the chronic form of cholecystitis, the signs may not particularly manifest themselves; in the future, the disease may make itself known in a more advanced form or take an acute form. In this case, only treatment in a special medical institution will avoid worsening the condition.
Symptoms of cholecystitis are identified by taking anamnesis, physical examinations (inspection and palpation), laboratory and instrumental studies:
Symptoms identified during history taking. Based on the patient’s complaints, previous diseases of the gastrointestinal tract, liver and other organs, the nature of pain in the abdomen and digestive disorders (nausea and vomiting, diarrhea, constipation, bloating) are established;
Symptoms determined by physical methods. A coated tongue is a sign of stagnation in the gallbladder. The leading symptom of cholecystitis is pain, determined by palpation, manifested in different projections of the body;
Differential diagnosis based on laboratory and instrumental research methods. The instrumental diagnosis of cholecystitis is based on probing of the duodenum and various modifications of X-ray and ultrasound examinations. With their help, the peristalsis of the bladder, the passage of bile into the lumen of the duodenum and other important functional and morphological indicators are determined.
Nausea with cholecystitis is a common symptom. Nausea is a condition that usually precedes the gag reflex. In some cases, nausea and vomiting is the body's protective reaction to intoxication. With cholecystitis, nausea and vomiting are always part of the pathogenesis of the disease.
Nausea with cholecystitis should be differentiated from similar symptoms with other diseases and pathologies:
The previously quite rare pathology “cholecystitis” has become much more common in recent decades. She has become significantly “younger”.
This was caused by the dominance of fast foods, fatty foods, replete with preservatives and various harmful additives in the modern person’s diet, as well as a fanatical desire to lose weight quickly in order to meet the ideals of beauty imposed by the media.
- What is cholecystitis?
- What tests should be taken for cholecystitis?
- General blood analysis
- Biochemical blood test for cholecystitis
- Increased bilirubin
- Useful video
- Conclusion
The disease can be asymptomatic for a long time or disguised as other diseases of the gastrointestinal tract. Laboratory blood tests for cholecystitis help clarify the situation and clarify the diagnosis.
What disorders develop in the gallbladder?
Among doctors, there is an opinion that acalculous cholecystitis is a form of transformation of chronic inflammation into cholelithiasis. However, long-term observation of patients does not confirm this theory.
In the chronic course of the disease (on the right), the bubble turns into a thickened, deformed “bag”
The internal mucous membrane has a reticular pattern due to the alternation of thick folds, areas of atrophy and polypous growths. Replacing inflammatory tissue with scars leads to fibrosis and irreversible changes in shape.
The loss of muscle fibers is accompanied by a decrease in contractile capabilities, and the involvement of nerve endings in the process contributes to atrophy of the walls and cessation of the release of bile into the duodenum. All clinical signs of cholecystitis are associated with subsequent disruption of the digestive process.
Further spread of inflammation to adjacent tissues causes pericholecystitis, liver abscesses, intestinal pseudodiverticula, and the formation of adhesions.
What is cholecystitis?
Cholecystitis refers to inflammation of the walls of the gallbladder. The inflammatory process can be caused by impaired outflow of bile and the presence of pathogenic microorganisms in the lumen of the bladder. This pathology may be a complication of gallstone disease. Slightly less often, the disease is caused by circulatory disorders in the walls of the common bile duct (bile duct).
People at risk are:
- with infectious processes in the liver and intestines;
- with parasitic infestations, with nutritional disorders;
- abusing diets for weight loss.
All this leads to deviations that appear not only in tests: the person feels a significant deterioration in well-being.
Cholecystitis is distinguished according to etiological characteristics into:
- non-calculous (without the formation of stones);
- calculous (with the formation of stones).
According to the flow they are divided into:
- spicy;
- chronic.
Acute cholecystitis is characterized by:
- severe pain in the right hypochondrium;
- nausea;
- vomit;
- bloating;
- Diarrhea is common.
The pain can be very intense and can only be relieved with antispasmodics. Body temperature rises to 38 degrees Celsius.
Painful sensations in this case become unbearable and force the patient to seek qualified medical help. The skin and sclera of the eyes become intensely yellow. In this case, the condition must be differentiated from other pathological processes in the gallbladder and internal organs. Laboratory tests, instrumental studies and ultrasound will help to do this most accurately.
What tests should be taken for cholecystitis?
Tests for cholecystitis help clarify the diagnosis, as well as assess the condition of the liver and pancreas. Changes in laboratory test parameters indicate the severity of the inflammatory process. Research is carried out throughout the treatment to confirm the effectiveness of treatment procedures.
What studies help confirm cholecystitis? A clinical blood test is prescribed for any deterioration in health, including if there is a suspicion of an inflammatory process in the body.
A biochemical blood test for cholecystitis often changes only with deep disturbances in the common bile duct and nearby organs. The acute and fresh process is practically not reflected in this study. If inflammation in the gallbladder is suspected from biochemical tests, it is advisable to prescribe:
- liver tests - thymol, ALT, AST (not to be confused with ASD for cholecystitis - Dorogov's antiseptic stimulant), bilirubin;
- protein fractions;
- alkaline phosphatase;
- GGTP (gamma-glutamyl transpeptidase) is an enzyme that is involved in the process of amino acid metabolism;
- amylase in blood and urine.
Urine and feces are also examined. In addition to a general urine test, which may reveal signs of kidney inflammation, which may indicate infection has penetrated into the kidney tissue, a test for urobilin and bile pigments, and the presence of bilirubin is prescribed.
Feces are tested for stercobelinogen. If the analysis reveals unprocessed bilirubin, this may be a sign of dysfunction of the gallbladder, its obstruction with stones, or an inflammatory process in it.
The meaning of atypical forms
The atypical course of noncalculous cholecystitis can imitate signs of disease of the intestines, heart, esophagus, kidneys, and stomach. Accordingly, the following manifestations take first place in clinical manifestations.
With the esophageal type - difficulty swallowing, constant heartburn, heaviness in the sternum; in the case of intestinal manifestations - pain along the intestines, diarrhea or constipation, constant bloating.
Similar manifestations are characteristic of the intestinal form of pathology.
The cardialgic form is characterized by anginal pain in the chest, attacks of rhythm disturbances from extrasystoles to attacks of paroxysmal atrial fibrillation, abnormalities are detected on the ECG; in young people, chronic cholecystitis can simulate a rheumatic process and causes pain in the joints.
The lumbar and pyelonephritic types occur under the guise of kidney inflammation or osteochondrosis in the lumbar region, the pain is greatest in the kidney area, a positive Pasternatsky sign is detected on the right, but during the examination there are no signs of inflammation in the urine or changes in the x-ray of the spine.
The gastroduodenal type is very similar to the course of a gastric or duodenal ulcer, gastroduodenitis with increased gastric secretion, pain occurs more often at night. Fibrogastroscopy reveals no changes.
Biochemical blood test for cholecystitis
Biochemical tests for cholecystitis may vary depending on the course and form.
Tests for cholecystitis for amylase (blood and urine) have increased results only if the pancreas is involved in the process. GGTP rarely deviates from the norm; only in severe advanced cases can increased numbers of this enzyme be obtained in the analysis. A quarter of patients with cholecystitis have elevated alkaline phosphatase. In the study of protein fractions - dysproteinemia, the globulin fraction increases.
Increased bilirubin
Bilirubin in inflammation of the gallbladder is usually normal. A slight deviation in this indicator may confirm the addition of toxic hepatitis.
In this case, increased indirect bilirubin may be observed in a biochemical blood test for cholecystitis. If hyperbilirubinemia is significant with a predominance of the direct fraction, one may suspect:
- blockage of the bile ducts with stones;
- vascular spasm;
- extrahepatic cholestasis;
- destructive changes in the gallbladder.